
Abstract
Abstract
Promoting access to safe drinking water or access to nutritious food, each independently contribute uniquely to positive gains in human health. Nexus analysis—a systems-based approach to study interconnection and interdependence—provides a framework to expose interactions and interventions in linked food–water systems. Interactions result in unintentional changes in efficacy or toxicity creating poorer-than-expected health outcomes while synergistic interventions targeting both “water, sanitation, and hygiene” as well as “food security, nutrition, and safety” yield greater-than-anticipated improvements in health and wellness. Herein, we describe a case study of linked food–water systems, where discovery, integration, application, and the scholarship of teaching and learning, collectively enhanced child health through convergence research—a transdisciplinary approach to solve a compelling and specific problem. The method integrates five techniques predominant in the field of health care, including: (1) community-based participatory research, (2) structured reviews, (3) mixed methods, (4) structural equation modeling, and (5) interprofessional education—at multiple study sites in east Africa, Guatemala, Brazil, and South Africa. The compelling problem explored is, “the lack of an overarching framework to achieve improvements in interdisciplinary environmental health practice and policy,” to ultimately solve specific problems such as, “the eradication of childhood stunting.” Results demonstrate that convergence research improves environmental health practice and policy by exposing insights to be measured, validated, and disseminated.
Introduction
Nexus analysis of linked food–energy–water systems (FEWs) has expanded over the past 40 years from calculations of eminent Malthusian catastrophe (Commoner, 1971; Ehrlich and Holdren, 1971), to definitions of sustainable development (Brundtland, 1987; Sachs, 2012), to increasingly complex, multivariate tools to guide decision making (James, 2015). Recently, the National Academies of Sciences, Engineering, and Medicine (NASEM) proposed that environmental engineers and scientists are uniquely positioned to contribute to sustainably delivering food, water, and energy, local to global (NASEM, 2019). Rather than independent approaches to understanding food, water, or energy separately, nexus analysis employs a systems-based approach to understand, predict, and react to interconnection and interdependence shared among food systems, water systems, and energy systems (Lighty et al., 2015). Nexus analysis facilitates synergistic interventions to yield greater-than-anticipated improvements in health and wellness (High Level Panel of Experts, 2015; General Assembly, 2016; Rosegrant, 2019; Willett et al., 2019).
Previously, we demonstrated the utility of structural equation modeling (SEM) to hypothesize, test, and disseminate causal mechanisms of food–water interaction—unintentional changes in efficacy or toxicity (Rodvold and Kraus, 2010)—correlating to unanticipated poor health outcomes among children (Divelbiss et al., 2013; Voth-Gaeddert et al., 2018a, 2018b, in review). Our use of SEM as a tool for nexus analysis is an example of “convergence research,” which the National Science Foundation defines as research (1) driven by a specific and compelling problem, and (2) leveraging deep integration across disciplines (Tornow et al., 2018).
Three theories underpin our conceptualization of linked food–water systems, namely: (1) “let food be thy medicine and medicine be thy food,” (2) “water as the first nutrient,” and (3) “food and water as universal human rights” (Black et al., 2003; Checkley et al., 2004; Russell and Azzopardi, 2019). Our case study explores these three theories as we examine the statistical relationships among water, food, and four characteristics of child health, including: (1) environmental enteric dysfunction (EED), (2) systemic inflammation, (3) diarrhea, and (4) child stunting (Voth-Gaeddert et al., 2018b).
Child stunting, defined as child height that is two standard deviations below the mean height-for-age as compared with the World Health Organization (WHO) growth chart (World Health Organization, 2010), correlates closely with both acute and chronic health outcomes (Johnson et al., 1987; Martorell, 2010). Recent reviews of the literature call into question the effectiveness of providing improved water, sanitation, and hygiene (WaSH) interventions to reduce diarrhea and eliminate stunting among children in low- and middle-income countries (Cumming and Cairncross, 2016; Gera et al., 2018). However, others argue that inflammation—including from consumption of unimproved drinking water—corresponds to stunting through a mechanism mediated by EED, an acquired subclinical disorder of the small intestine that prevents proper nutrition (Harper et al., 2018). Furthermore, a prior longitudinal study in Benin, West Africa documented a correlation—although, without elucidating an underlying mechanism—between impaired growth and consumption of elevated levels of aflatoxin—a family of toxins produced by fungi found on agricultural crops such as maize, peanuts, and tree nuts (Gong et al., 2004). The lack of clarity within the literature suggests current research methods are insufficient to expose necessary insights in complex systems.
The compelling problem explored through convergence research is the need to identify an overarching framework to achieve improvements in interdisciplinary environmental health practice and policy. The specific case study demonstrates that the interaction of insufficient drinking water treatment and consumption of toxin-laden food are co-contributors to childhood stunting through EED among the non-Spanish-speaking rural population living in the western highlands of Guatemala—the sixth most stunted nation in the world (World Health Organization, 2010; ICF International, Inc., 2014; U.S. Agency for International Development, 2016).
To achieve transdisciplinary integration, this method integrates five techniques prevalent in health care, including: (1) community-based participatory research (CBPR), (2) structured reviews, (3) mixed methods, (4) SEM, and (5) interprofessional education (IPE)—at multiple study sites in east Africa, Guatemala, Brazil, and South Africa. Through an iterative approach, where the results from one or more techniques at one or more study sites were used to improve subsequent and ongoing efforts, we sought to achieve unity among Boyer's four models of “scholarship” in higher education, namely: (1) discovery, (2) integration, (3) application, and (4) the scholarship of teaching and learning (Boyer et al., 2015). Because the ultimate objective is to improve environmental health practice and policy, the case study highlights explicit efforts at translational research—“the process of turning observations in the laboratory, clinic, and community into interventions that improve the health of individuals and the public,” (National Center for Advancing Translational Sciences, 2015). To support translational research, we recruited diverse partners—including community health practitioners in developing countries and in the United States—and we adopted a transdisciplinary approach—integrating health care research into engineering practice and policy.
In this article, we describe our efforts to improve environmental health practice and policy through a scalable method of convergence research. Although the details of our case study highlight efforts to dramatically reduce—and perhaps even eliminate—rampant stunting among the children in the western highlands of Guatemala, in the summary we argue that this scalable method may be replicated for a variety of pressing societal issues of linked food–water systems.
Techniques
Community-based participatory research
CBPR is used to solve problems. In a recent study, the NASEM reported that CBPR is used effectively to eliminate disparities in health among communities negatively impacted by inequities (NASEM, 2017). As described by Wallerstein and Duran (2006), “…CBPR is an orientation to research that focuses on relationships (emphasis added) between academic and community partners”; thereby aligning researchers with embedded community knowledge to craft context-relevant questions, which later aid in the acceptance and dissemination of findings. A fundamental trait of CBPR is to include participating research communities at the initiation of the study as equal partners in exposing and prioritizing intervention research (CBPR Program of the National Center on Minority Health and Health Disparities, 2005). The Detroit Community-Academic Urban Research Center is an example of a longstanding and highly regarded CBPR (Israel et al., 2010).
Increasingly, those who employ CBPR are recognizing the importance of decolonizing a dominant Western research paradigm when engaging with first-nation communities (Koster et al., 2012). Prior research explored the use of CBPR to address food insecurity within Native American communities living on a reservation in the United States (Jernigan et al., 2012) as well as rural subsistence farmers in the highlands of Guatemala (Arnes et al., 2018), and CBPR was used to address water insecurity among rural communities living in Oaxaca, Mexico (Rowles et al., 2018). An important consideration for the use of CBPR is co-ownership of results, and researchers must be aware of best practices for authoring and disseminating the results of CBPR (Bordeaux et al., 2007; Grieb et al., 2015). A benefit of the CBPR approach is that student researchers can play an active role in all phases of the undertaking (Martinez et al., 2012).
Structured reviews
Structured reviews (i.e., “systematic reviews” and “meta-analyses”) are undertaken to synthesize the literature. In a recent study, the Institute of Medicine reported that structured reviews provide the most reliable manner of evaluating interventions (Institute of Medicine, 2011). As described by Young and Solomon (2009), “To practice evidence-based medicine, clinicians need to apply the findings of scientific research to the circumstances of individual patients … must be able to select and appraise scientific literature that is relevant to their field, understand the implications of the research findings for individual patients, elicit patients' own preferences and develop an appropriate management plan based on the combination of this information.” Cochrane, a British charity established in 1993, enjoys a worldwide reputation for publishing systematic reviews of health care interventions as part of the Cochrane Library (de Vrieze, 2018).
Consensus guidelines for the performance of structured reviews include overall frameworks such as PRISMA (a.k.a., preferred reporting items for systematic reviews and meta-analyses) (Moher et al., 2009), rubrics to rate the quality of scientific evidence such as GRADE (a.k.a., grading of recommendations assessment, development and evaluation) (Dijkers, 2013), and tools for the evaluation of well-defined types of research studies such as MOOSE (a.k.a., meta-analysis of observational studies in epidemiology) (Stroup et al., 2000). Structured reviews were employed to evaluate interventions to improve water quality for preventing diarrhea illness (Clasen et al., 2007, 2010), disposing human excrement to prevent diarrhea (Clasen et al., 2015), and nutritional interventions to reduce child stunting (Dewey and Adu-Afarwuah, 2008; Goudet et al., 2015). Structured reviews form the basis for further research such as the recent work of Humphrey et al. (2019) employing randomized control trials to expose the independent and combined effects of WaSH interventions coupled with complementary feeding to reduce childhood stunting.
As summarized by Garrard (2017), “One way to master [the art of conducting a structured review] is to realize that a review of any body of literature actually consists of four fundamental tasks, after the subject of the review has been decided: 1) make decisions about which documents to review; 2) read and understand what the authors describe in those documents; 3) evaluate the ideas, research methods, and results of each publication; and 4) write a synthesis that includes both the content and a critical analysis of these materials.”
Mixed methods
Mixed methods integrate the results of quantitative and qualitative research. In their highly cited articles, Johnson and Onwuegbuzie (2004) describe an effective framework for designing and conducting mixed methods research and in collaboration with Johnson et al. (2007) they subsequently describe the unique aspects of three major “research paradigms”—namely quantitative research, qualitative research, and mixed-methods research. On the one hand, “Quantitative purist … articulate assumptions that are consistent with what is commonly called positivist philosophy … contend[ing] that the observer is separate from the entities that are subject to observation,” (Johnson and Onwuegbuzie, 2004). On the other hand, “Qualitative purist … contend that multiple-constructed realities abound, that time- and context-free generalizations are neither desirable nor possible, that research is value-bound, that it is impossible to differentiate fully causes and effects, that logic flows from specific to general … and that the knower and known cannot be separated because the subjective knower is the only source of reality,” (Johnson and Onwuegbuzie, 2004).
The mixed-methods research approach is pragmatically promoted as an “all-welcoming” middle ground that rejects the incompatibility theory of polarized purist to overcome the limitation of either approach alone (Johnson et al., 2007). The message, “numbers numb, stories sell,” is central to the value of mixed-methods research (Pluye and Hong, 2014), where a single observational case study may receive a similar emphasis as a double-blind randomized control trial. Rich data resources such as the, “Baseline Study for the Title II Development Food Assistance Programs in Guatemala,” provide a comprehensive resource for quantitative research (ICF International, Inc., 2014); whereas the “one-on-one interview” has been demonstrated as a valuable source of qualitative data in environmental health (Scammell, 2010).
Recently, mixed-methods research has exposed interventions for improving infant and young child feeding in rural Guatemala, including education about nutrition and promoting behavior changes to encourage consumption of fortified foods rather than “junk food purchases,” (Brown et al., 2014). Additionally mixed-methods research has exposed causes of hunger among subsistence farmers in rural Nicaragua (Bacon et al., 2014), and to define and predict food insecurity in Costa Rica (Ruiz et al., 2017). While mixed methods are not common in engineering research, there is a significant and growing trend to use mixed methods within engineering education (Borrego et al., 2009), where it is argued that, “… we take the view that the approach used by a given study should be driven by the research questions of that study…” and thereby encourage a full toolkit of techniques spanning all relevant disciplines.
Structural equation modeling
A form of causal modeling, SEM includes a diverse set of mathematical models and statistical techniques that fit researcher-defined networks to gathered data (Kaplan, 2008). SEM employs confirmatory factor analysis, path analysis, partial least squares path modeling, and latent growth modeling to fit hypotheses to data (Grace, 2006; Kline, 2015), and has been used previously to study the nexus of environmental determinants and social determinants of health (Sanchez et al., 2005; Fyhri and Klaeboe, 2008; Silva et al., 2010). As a modeling tool, SEM provides a number of advantages, including: (1) visualization of relationships among variables, (2) the concurrent use of observable variables and latent variables—inferred phenomena that are not directly observed, (3) the use of mediation variables which demonstrate potential influences among variables, and (4) the ability to incorporate existing knowledge into the model definition. It should also be noted that there is no general consensus determining sample size, and that sample size required to yield useful results is impacted by the number of observations per parameter and number of observations per degree of freedom in the model (Kaplan, 2008). Like all statistical techniques, the proper use of SEM requires in-depth knowledge of the relevant literature; otherwise spurious findings could be interpreted from the study.
Interprofessional education
The chief purpose of IPE is the improvement of patient-centered health care through collaborative practice. Motivated, in part, by predicted worldwide shortages in health care providers, the WHO convened the, “Study Group on International Education and Collaborative Practice,” that presented their consensus findings in the form of a “framework for action” (Health Professions Network Nursing and Midwifery Office, 2010). A key definition of IPE is, “… when students from two or more [healthcare] professions learn about, from, and with (emphasis added) each other to enable effective collaboration and improve health outcomes … [where] collaborative practice [is defined as] health workers from different professional backgrounds work[ing] together with patients, families, carers, and communities (emphasis added) to deliver the highest quality of care,” (Health Professions Network Nursing and Midwifery Office, 2010).
Recently, Mihelcic et al. (2017) presented a detailed argument calling for leadership by environmental engineers to achieve a broad definition of sustainability, including—inter alia—the historical area of WaSH as well as the areas of health, climate, water, energy, and food security; economic development; and reduction of social inequalities. Oerther (2017) presented a case for and examples of the high degree of similarity among the Environmental Theory of Florence Nightingale and the origins of sanitary engineering with an emphasis on the value to future engineers who are trained alongside future nurses delivering high-quality community health. As concluded by Nandan and London (2013) in their review of the IPE literature, “… [educational] experiences can enable students to engage in generative and transformational learning, which can later facilitate in creation of innovative solutions for society's recalcitrant physical, social, and environmental issues.”
Examples of these “educational experiences” include didactic programs, community-based learning, and interprofessional simulation (Bridges et al., 2011), which can be used in low-resource environments (Busari et al., 2017). In addition, a critical “first-step” for successful IPE is candid assessment of the readiness of professionals, educators, and students to explore the unfamiliar area known generally as “team science” (Hall et al., 2008).
Results
To develop an overarching framework to achieve improvements in interdisciplinary environmental health practice and policy, five techniques predominant in the field of health care were used to study causal mechanisms of food–water interaction correlating to unanticipated poor health outcomes among children at multiple study sites in east Africa, Guatemala, Brazil, and South Africa. Figure 1 provides an overview of the approach.
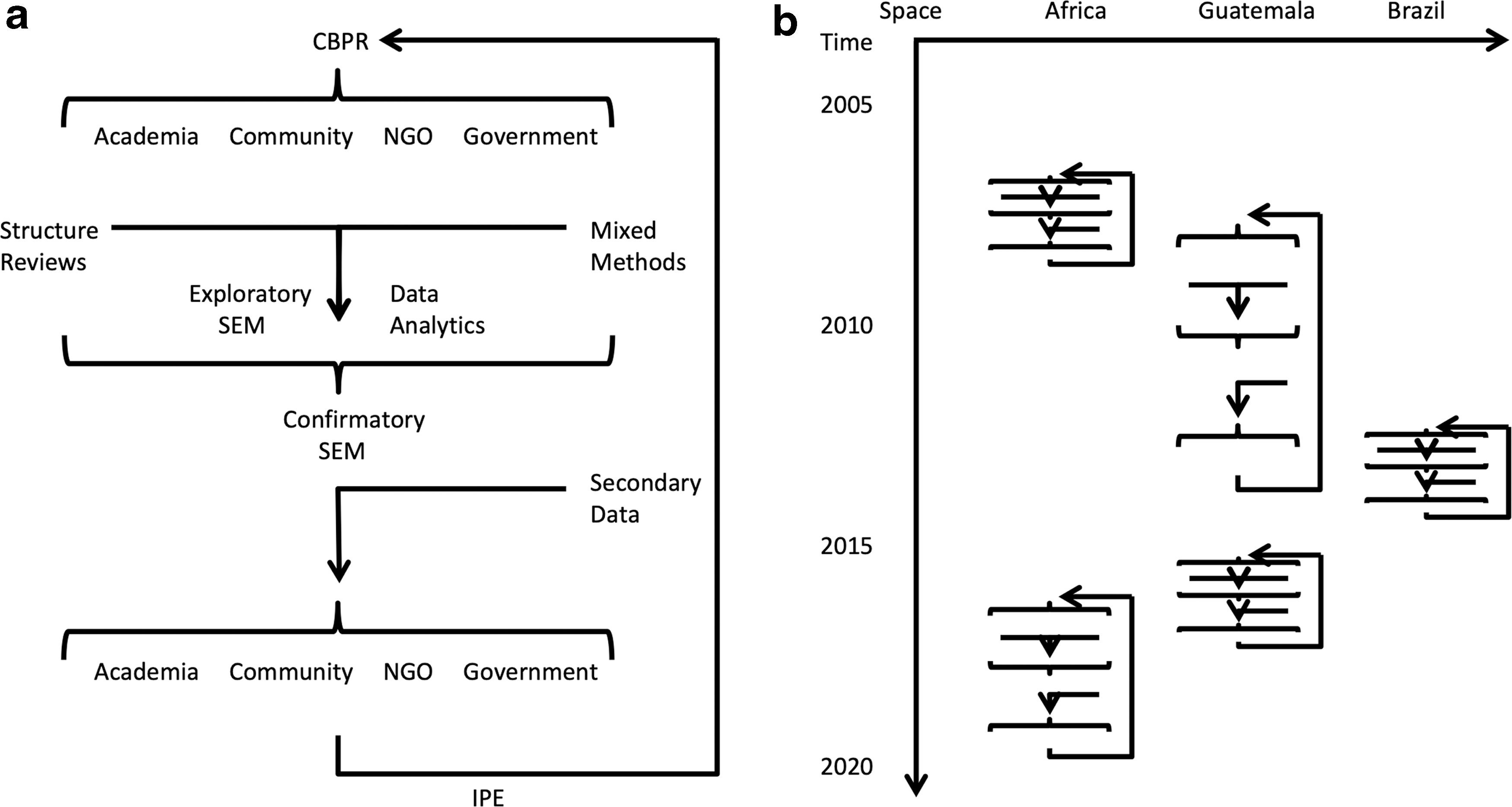
Integration of five techniques predominant in the field of health care to create an overarching framework to achieve improvements in interdisciplinary environmental health practice and policy.
The first step in the approach, detailed in Fig. 1a, employed CBPR to recruit diverse stakeholders, including: (1) members of academia, (2) community members, (3) members of nongovernmental organizations, and (4) representatives of the government. Subsequently, stakeholders screened structured reviews to expose knowledge gaps, and mixed methods were employed to consider both the results of quantitative studies (i.e., double-blinded randomized control trials) as well as qualitative studies (i.e., interviews and focus groups). Additional sources of insight were exposed through the judicious use of exploratory SEM and other techniques of data analytics (i.e., network analysis or NA).
Ultimately, the academic researchers formed testable hypotheses structured as confirmatory SEMs using all of the inputs—structured reviews, mixed methods, and additional insights. Secondary datasets were collected, the strengths of the correlations in the confirmatory SEM were measured, and the results were presented to all stakeholders for validation. Alongside the research effort, IPE was used simultaneously to gather information from the community and to disseminate results to the community, which contributed to a virtuous feedback loop informing the composition of the stakeholder community. The iterative approach presented in Fig. 1a was employed over a period ∼15 years in diverse geographic locations, including east Africa, Guatemala, Brazil, and South Africa. Figure 1b provides a schematic indicating the temporal and spatial distribution of the efforts considered in the case study, below.
In prior publications (Divelbiss et al., 2013; Voth-Gaeddert et al., 2018a, 2018b) and in unpublished work (Voth-Gaeddert et al., in review), SEMs were used to evaluate the nexus of linked food–water systems in the context of interprofessional environmental health research, practice, and policy recommendations. These studies measured the effect of environmental determinants and social determinants on diarrheal health burden in families with access to a CAWST (Centet for Affordable Water and Sanitation Technology, Alberta, Canada) biosand filter in Guatemala (Divelbiss et al., 2013) and in Brazil (Voth-Gaeddert et al., 2018a). Two interrelated SEMs examining childhood stunting as well as EED were developed for Guatemala (Voth-Gaeddert et al., 2018b). Finally, SEMs were used to evaluate gender differences on diarrheal health burden as well as inflammation in males versus females in South Africa (Voth-Gaeddert et al., in review).
The essential results from each of these prior studies were adapted to a common format, and the results are presented in Fig. 2 for comparison. Rectangles represent indicator variables, whereas ovals represent latent variables—inferred phenomena that are not directly observed. Lines represent statistically significant relationship at the 90% confidence interval, whereas variables that have failed to demonstrate statistically significant relationships with other variables are shown as crossed-out text. Terms not surrounded by a shape represent observable variables (i.e., measured directly rather than calculated). The gray lines represent a special relationship of moderating variables, whereas the dashed lines represent a special relationship dependent upon gender.
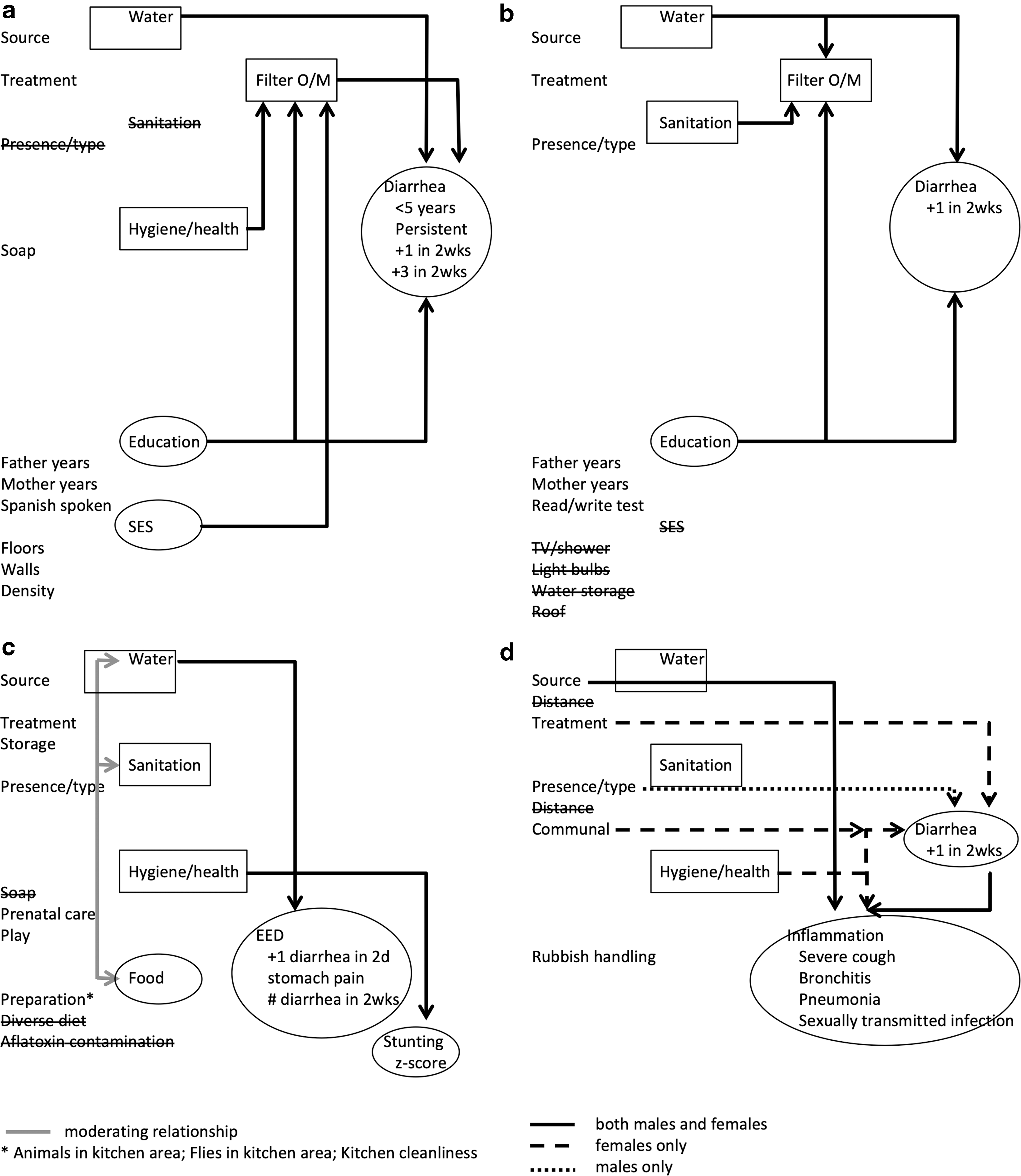
Summary SEMs developed in each of four studies using a common layout for ease of comparison. Comprehensive summary of all the outputs for all four SEMs.
Figure 2a summarizes the chief findings for Quiche, Guatemala reported in Divelbiss et al. (2013). While the details of the SEM are provided in depth in the original publication, the summary presented in Fig. 2a shows that the occurrence of diarrhea is impacted directly by three mechanisms, namely: (1) access to improved water, (2) better operation and maintenance of CAWST biosand filters, and (3) a higher level of education among the parents in the household. The solid lines connecting the variables “water,” “Filter O/M,” and “education” to the variable of “diarrhea” represent these direct impacts (at the 90% confidence limit). Rectangles (i.e., “water” and “Filter O/M”) represent indicator variables; whereas ovals (i.e., “SES” and “diarrhea”) represent latent variables. Finally, the variables “source” and “treatment” refer to the observable variables that make up the indicator variable “water”; the observable variables “Father years (of formal schooling),” “Mother years (of formal schooling),” and “Spanish spoken (in the household)” refer to the observable variables that make up the latent variable “education”; and the observable variables “Floors (composition),” “Walls (composition),” and “Density (i.e., number of household residents per room)” refer to the observable variables that make up the latent variable “SES.”
Using this nomenclature, Fig. 2a shows that the occurrence of diarrhea is also impacted indirectly through better operation and maintenance of CAWST biosand filters that mediates three indirect mechanisms, namely: (1) hygiene, (2) education, and (3) socioeconomic status. Finally, the “presence” and the “type” of any “sanitation” facility failed to show statistically significant impact as represented by the crossed-out text. The results expose that policy makers should consider return on investment and realize that both additional biosand filters (i.e., “treatment” of “water”) as well as additional “education”—especially additional education of girl children achieved, in part, due to policies that discourage child marriage—likely have a significant impact on diarrhea occurrence [i.e., through “Mother years (of formal schooling)”].
Figure 2b presents a brief summary of the chief findings in Brazil reported by Voth-Gaeddert et al. (2018a), and shows that only access to an improved water source and higher household education levels have a direct impact on diarrhea occurrence as shown by the solid lines connecting the indicator variable “water” and the latent variable “SES” with the latent variable “diarrhea.” Furthermore, while the presence of a pit latrine, access to an improved water source and higher household education levels impact filter operation and maintenance, there is no statistically significant impact on diarrhea occurrence as reflected by the lack of a line connecting the indicator variable “Filter O/M” and the latent variable “diarrhea.”
Finally, despite using four directly observable variables to make up socioeconomic status, there was no statistically significant impact as represented by the crossed-out text. The differences between the results observed in Quiche, Guatemala (Fig. 2a) and the results observed in Brazil (Fig. 2b) suggest that practitioners should consider the local conditions when designing an intervention because results observed in one local condition (i.e., in Guatemala as reported in Divelbiss et al., 2013) may not apply in another local condition (i.e., in Brazil as reported in Voth-Gaeddert et al., 2018a).
Figure 2c summarizes briefly the chief findings in Totonicapan, Guatemala reported by Voth-Gaeddert et al. (2018b), and shows a direct relationship between access to improved drinking water and EED, a direct relationship between health and hygiene interventions and stunting, but failed to show a statistically significant relationship between EED and stunting. Furthermore, the manner in which food is prepared, the presence of a pit latrine and access to improved drinking water share a moderating relationship with each other meaning that these variables influence each other. Finally, the latent variable “food” was influenced by preparation—inter alia—animals and flies in the kitchen and general kitchen cleanliness—but was not influenced by diet (diversity) or the presence of aflatoxin in the food stuff.
The results demonstrate that interdisciplinary environmental health professionals should consider a separate but equal approach to EED (as measured by diarrhea) and stunting (as measured by height for age) because no statistically significant synergies were observed among the interventions.
Figure 2d highlights the chief findings in South Africa of Voth-Gaeddert et al. (in review), and shows access to an improved water source and the occurrence of diarrhea are directly related to systemic inflammation for both males and females (i.e., solid line); whereas, females alone (dashed line for diarrhea and inflammation) were impacted by the type of water treatment, the presence of communal pit latrines, and the handling of rubbish; and males alone (dashed line for diarrhea and inflammation) were impacted by the presence of a pit latrine. Finally, the observable variable “distance” from a water supply or pit latrine did not show statistically significant influence in this model. These results suggest that practitioners and policy makers should consider sex-specific responses to interventions.
Discussion
Pilot effort in east Africa
Our approach began with recruitment of diverse stakeholders as part of CBPR.
From 2006 to 2009, a pilot study—including partner organizations, namely: (1) Village Life Outreach Project, (2) Shirati Health and Education Development Foundation, (3) Okullo Family Trust, (4) Engineers Without Borders student chapter at the University of Cincinnati, and (5) Nurses Without Borders student chapter at Xavier University—worked alongside rural communities among the Luo-speaking tribe of Kenya and Tanzania (Pumphrey et al., 2006, 2007; Pumphrey, 2008; Oerther, 2009). Altogether, health care providers and engineers were trained side by side through regular community visits in an early effort of IPE (Oerther and Oerther, 2013, 2015; Oerther, 2017). The short-term interventions by health care providers (i.e., week-long medical brigades) gained trust with the community, and the long-term interventions by the engineers (i.e., household access to improved drinking water) helped to reduce diarrhea burden among children.
As the team gained experience in CBPR and in IPE, it became clear that this pilot work was strongly guided by the theory of, “let food be thy medicine, and medicine be thy food,” where synergies of health care interventions and engineering interventions yielded greater-than-anticipated improvements in health and wellness. It also became clear that a technique was needed to hypothesize, test, and disseminate causal mechanisms. Therefore, SEM was tested in a new study site in Guatemala.
SEM of CAWST biosand filters in Quiche, Guatemala
Leveraging the ongoing pilot work conducted in east Africa—where we explored CBPR and IPE—an SEM was created using a new study site in Guatemala. From 2007 to 2009, a CBPR approach—including partner organizations, namely: (1) Hechos 2:8, (2) Mission Impact, (3) local representatives of the Government of Guatemala (GoG), (4) CAWST, and (5) the Centers for Disease Control—was used to construct the initial SEM for Guatemala by working alongside rural communities—including: (1) local political leaders, and (2) women's self-help groups—in the department of Quiche (Divelbiss and Oerther, 2010; Divelbiss, 2011; Oerther and Oerther, 2013; Oerther, 2016, 2017). Incorporating both the priorities expressed by members of local households and an approach of sweat equity and sustainability strongly advocated by the local partner organization, research in Guatemala focused on “learning by doing” and included the establishment of a cottage industry to construct CAWST biosand water filters.
Due to existing evidence on limited effectiveness of household water treatment devices (Sobsey et al., 2008)—often attributed to recent maintenance, access by children or animals, depth of fine sand bed falling below 46 cm, and using extremely poor-quality source water (Fewster et al., 2004)—the next 2 years of research, 2010–2012, focused on improving techniques for exposing the effectiveness of the intervention using a mixed-methods approach, and training up community health workers to build capacity throughout the region (Oerther and Oerther, 2015; Oerther, 2016).
The CBPR team in Quiche refined the initial SEM using mixed methods, which included structured review as well as one-on-one interviews of members of individual households who had installed a filter (Divelbiss, 2011). A survey instrument was created and used to collect data from 286 households selected from a randomized sample of convenience. Subsequently, these data were used to, “… test the hypothesized model with the collected data to determine the strength of statistical correlations among demographic and environmental health factors that influence biosand filter operation and maintenance and household diarrhea burden,” (Divelbiss et al., 2013). To translate the SEM findings to practice and policy, IPE was utilized to improve capacity within the region to understand, promote, and educate the community about the importance of improved water quality. Engineering students were trained alongside members of the local health care system through workshops facilitated by Hechos 2:8 and local representatives of the GoG. Approximately one-third of the community health workers throughout Quiche received training in this manner. Subsequently, these community health workers built the local capacity to maintain and operate CAWST biosand filters, and increased the demand for improved water quality within members of the community.
The cross-disciplinary training—including students of engineering and members of the local health care system, which included nurses, midwives, health advocates, and peer coaches—improved the capability to share results within the community. For example, the presence of a student of engineering from the United States and an official from the GoG added both an assurance of quality and an assurance of authority during community presentations, whereas delivery of the information by a female from the local health care system speaking an indigenous language increased the authenticity of the message. By including local partners—especially women and political leaders—the CBPR stakeholders attempted to reduce the impact of the Hawthorne effect—where individuals modify an aspect of their behavior in response to their awareness of being observed (McCambridge et al., 2014). From 2012 through 2015, more than 3,500 CAWST biosand filters were distributed providing improved water quality to more than half of the 70,000 residents of Quiche (Oerther, 2016).
SEM of CAWST biosand filters in Brazil
While experiencing positive results in Quiche, Guatemala, our next effort was to demonstrate the portability of the approach through replication. To this end, SEMs were created at a second study in the state of Para, Brazil. From 2012 through 2014, a CBPR approach, including partner organizations, namely: (1) Project Amazon; (2) University of Western, Para; and (3) Brazil Fulbright Commission—was used to construct an initial SEM for Brazil by working alongside rural communities—including: (1) local political leaders; and (2) community members—around the city of Santarem (Voth-Gaeddert, 2014; Voth-Gaeddert and Oerther, 2014, 2015a; Voth-Gaeddert et al., 2014).
A mixed-methods approach was utilized beginning with interviews, conducted through a translator, of individual households with existing CAWST biosand filters provided through a prior intervention in the region by Rotary International. A household survey instrument was created and used to collect data from 20 households—selected in consultation with local political leaders—in the village of Enseado do Aritapera (Voth-Gaeddert et al., 2015b). Through an iterative process, a second round of household surveys were collected from 17 representative homes in the village of Carapanatuba and 24 representative homes in the village of Cabeca D'onca (Voth-Gaeddert et al., 2015c). To further refine the SEMs, from 2015 through 2017, the CBPR approach was expanded to include additional researchers from the Missouri University of Science and Technology (Missouri S&T), and the mixed-methods approach was expanded to include Demographic and Health Surveys (DHS) data (U.S. Agency for International Development, 2016).
Following recommendations from the additional researchers at Missouri S&T, the DHS data were analyzed with three statistical techniques—namely: (1) Mahalanobis–Taguchi Strategy, (2) canonical correlation analysis, and (3) latent factor regression—and these results were compared with the results of the SEM tested with survey data collected from a further 65 households (Voth-Gaeddert et al., 2018a). As further evidence of the value of the mixed-methods approach, DHS data were also acquired for Guatemala, analyzed with three statistical techniques, and a favorable comparison of results to the prior SEM in Quiche, Guatemala (Divelbiss et al., 2013) provided further confidence in both the SEM results as well as the value of the overall approach (Voth-Gaeddert et al., 2018a). The collective results—in Quiche, Guatemala, and Brazil—increased our confidence in the general approach and supported the theory of, “water as the first nutrient,” meaning that an engineering emphasis on WaSH was appropriate.
SEM of stunting in Totonicapan, Guatemala
To expand beyond water systems and to demonstrate SEMs for nexus analysis of linked food–water systems, in 2015 our team began CBPR at a second study site in Guatemala. The department of Totonicapan was selected because it adjoins the department of Quiche and provides a population that shares many similarities. Partners in Totonicapan, included: (1) the staff of the San Vicente Health Clinic, (2) community health workers throughout Totonicapan, (3) U.S. Peace Corps, (4) U.S. Agency for International Development (USAID), (5) additional researchers at Missouri S&T, (6) local political leaders, and (7) community members around the city of San Vicente Buenabaj (Voth-Gaeddert et al., 2018b). Leveraging prior experience, an initial SEM was constructed using a structured review of the available peer-reviewed literature as well as interviews with nutrition experts provided through relationships within the U.S. Government (USG) (Voth-Gaeddert, 2017).
A mixed-methods approach was used to refine the SEM, including NA of historical data extracted from the Food for Peace Baseline Survey conducted by the USAID (ICF International, Inc., 2014) as well as confirmatory SEM using survey data collected from a population of 372 individuals who voluntarily participated in a health assembly hosted by the San Vicente Health Clinic (Voth-Gaeddert et al., 2018b, 2019a). IPE included cross-disciplinary training of students of engineering and members of the local health care system along with development professionals from the USG. These teams were then responsible for conducting health assemblies encouraging improved water quality as well as promoting local understanding of food security, defined as, “Food security exists when all people, at all times, have physical, social, and economic access to sufficient, safe, and nutritious food which meets their dietary needs and food preferences for an active and healthy life,” (Food and Agriculture Organization, 1996).
From 2016 through 2018, efforts at translation science included health assemblies targeting tens of thousands of non-Spanish-speaking indigenous rural villagers throughout the eastern municipalities of Totonicapan (Voth-Gaeddert et al., 2018c, 2019b; Oerther, 2019; Smethurst, 2019).
An important aspect of the work in the western highlands of Guatemala was our recruitment of non-Spanish-speaking villagers as stakeholders in CBPR. These descendants of the Mayan empire suffered decades of systematic discrimination, including armed conflict, forced relocation and expropriation of lands, and discrimination against indigenous languages and customs, and collectively, these inequities are believed to contribute to a hostile environment yielding poor health outcomes, including stunting (World Health Organization, 2010; ICF International, Inc., 2014; U.S. Agency for International Development, 2016). Therefore, our work in Guatemala has been motivated increasingly by the theory that “food and water are universal human rights.”
If as argued by Mihelcic et al. (2017)—environmental engineers have the ability to reduce social inequalities—our work adopts the view that engineers also have a professional obligation to reduce social inequalities. To this end, we returned to Africa with our new approach—“an overarching framework to achieve improvements in interdisciplinary environmental health practice and policy.”
SEM exploring sex differences in South Africa
Girls, especially in the global South, from lower socioeconomic status and with less education, tend to be one of the most marginalized populations, globally. Therefore, to demonstrate gender-specific differences observed in SEMs for nexus analysis of linked food–water systems, in 2016 our team began CBPR at a new study site in a township near Cape Town, South Africa. Partners in South Africa include: (1) researchers at the University of the Western Cape, (2) researchers at the University of Witwatersrand, (3) local community health workers, and (4) community members of Soweto (Voth-Gaeddert et al., in review). A recently published structured review coauthored by members of the CBPR team analyzed the peer-reviewed literature to evaluate changes in the prevalence of stunting among children in South Africa (Said-Mohamed et al., 2015), and a recently published mixed-methods study coauthored by members of the CBPR team reported on weight and physical activity in South African children as measured directly in 341 individuals under 6 years of age as well as discussed in focus groups involving 55 teachers and parents/caregivers (Draper et al., 2017).
Combined with prior experience using SEMs in Guatemala and Brazil, the team developed a refined SEM (Voth-Gaeddert et al., in review). Ongoing efforts in South Africa included the establishment of IPE in partnership with the local community health workers, health care providers studying at the Faculty of Health Sciences of the University of Witwatersrand, and engineering students. While these efforts are still in their formative stage, the early results support the belief that environmental engineers may contribute to eliminating disparities in health among populations negatively impacted by inequities (Mihelcic, 2017; NASEM, 2017).
Linking to Boyer's four definitions of scholarship
As described in the results above, CBPR is a technique to eliminate disparities in health, and coupled with IPE, the two techniques improve health by exposing and sustaining interventions to benefit the partner community. SEM was used as a technique to hypothesize, test, and disseminate causal mechanisms, and both structured reviews and mixed methods were shown to be useful to refine SEMs. The general approach we have developed—integrating five techniques predominant in health care—is called, “systems thinking,” and it has been shown to have value as a framework for sustainable development (Amadei, 2015). In our approach, knowledge creation is captured in the form of a confirmatory SEM, and mixed methods are used to refine a confirmatory SEM by infusing the results of structured reviews (i.e., “systematic reviews” and “meta-analyses”), additional insights from analysis of quantitative data (i.e., exploratory SEM and data analytics), and the results of qualitative findings from interviews and focus groups. Finally, IPE facilitates cross-disciplinary training, which is used subsequently to provide community education offered by teams, including engineers and health care providers.
Based upon our experience, CBPR ensures that the voice of community members directly influence the hypotheses captured in the confirmatory SEMs. Structured reviews provide the voice of history, while mixed methods provide the voice of quantitative data from historical sources or data recently collected as part of the study as well as the voice of qualitative data recently collected as part of the study from interviews and focus groups. In addition, we found that sharing the structured reviews among the CBPR stakeholders stimulated ideas among local experts and created new opportunities to refine the SEM. Our approach to mixed methods often consisted of parallel use of “big data” collected and made publically available by national or international agencies (i.e., the DHS, or the Baseline study for the Title II development food assistance programs in Guatemala) as well as semistructured interviews with stakeholders, including household assessments with standardized surveys. We found it helpful to engage the CBPR stakeholders in the development of the IPE approach as community health workers were both a valuable asset of localized knowledge used to refine the confirmatory SEMs as well as the solution to the challenge of sustainability; because community health workers are embedded within the community and often outlast the research partnership.
Limitations
While our approach shows promise as an overarching framework to achieve improvements in interdisciplinary environmental health practice and policy, each of the five techniques integrated into the approach suffers from limitations. For example, CBPR suffers from the Hawthorne effect—where individuals modify an aspect of their behavior in response to their awareness of being observed—often because of the power imbalance among stakeholders from different educational and socioeconomic backgrounds. IPE is limited by the availability of resources for transdisciplinary training (i.e., “interaction” is a term with specific meaning within health care, and therefore the meaning of “food and water interaction” is significantly different for engineers and health care providers). As recently described in a special issue of Science magazine, structured reviews often create as much controversy as they claim to resolve through definitive synthesis of the literature (de Vrieze, 2018), and similarly, mixed methods produce incongruent results when what appears as anecdotal data from a face-to-face interview with one or a few individuals is compared with statistical analyses of “big data.” Finally, SEMs suffer a number of limitations, including missing variables, limitations in judging model fitness, and the inaccuracy of some commonly used “rules of thumb.”
Beyond the techniques, our first-hand experience over the past 15 years exposes a significant challenge in the performance of convergence research; namely, the unfamiliarity of academic stakeholders translating research results into evidence-based practice and informing policy recommendations. Anticipating this challenge, in 1990 Ernst Boyer advocated for the expansion of the traditional definition of “research” in higher education to include four types of “scholarships,” namely: discovery, integration, application, and the scholarship of teaching and learning (Boyer et al., 2015). Boyer's model has been debated, rejected (Schweitzer, 2000), and adopted across a variety of institutions of higher education with varying degrees of success (Boyd, 2013).
The apparent dichotomy of these different forms of scholarship and the argument to separate “pure research” from “community advocacy” is an area of active and ongoing conversation within the field of environmental engineering. Some faculty argue that the current systems of higher education research is significantly flawed (i.e., Edwards and Roy, 2017; Mihelcic, 2017), whereas other faculty see value in separating “research” from “service” or “advocacy” (Sedlak, 2016). The case study we presented agrees with Boyer and emphasizes the value of translational science to impact child health.
Summary
Recognizing the compelling need to create an overarching framework to achieve improvements in interdisciplinary environmental health practice and policy, we demonstrate a new method integrating five techniques predominant in the field of health care—CBPR, structured reviews, mixed methods, SEM, and IPE—through the presentation of a case study to improve environmental health practice and policy by exposing insights to be measured, validated, and disseminated. Our results demonstrate that a systems-based approach to study interconnection and interdependence supports nexus analysis of linked food–water systems. Furthermore, our approach represents convergence research where problems are solved through transdisciplinary collaboration.
While our case study is focused primarily upon solving a specific problem, such as the eradication of childhood stunting in the western highlands of Guatemala, the approach is scalable and may be replicated for a variety of pressing societal issues of linked food–water systems. For example, exposing food miles—the distance food is transported from the time of its production until it reaches the consumer—or virtual water—the hidden water in food or other commodities traded from one place to another—are examples of such pressing societal issues. Perhaps no other recent example is as significant or as profound as the Eat-Lancet commission on healthy diets from sustainable food systems, where Willett et al. (2019) argue for a “diet” to save the planet from “climate change.”
We expect that the field of environmental engineering will benefit greatly from further scaling up of our overarching framework because the holistic approach encourages researchers to integrate all four of Boyer's models of “scholarship” into a single translational effort by: (1) adopting the rigorous hypothesis generation and testing that is a hallmark of discovery research in the form of confirmatory SEM; (2) linking across diverse disciplines required of integrative research, including structured reviews and mixed methods; (3) incorporating engagement research with a diversity of stakeholders through CBPR; and (4) facilitating the training of future environmental engineers in partnership with health care professionals through IPE.
Footnotes
Acknowledgments
The authors wish to thank three anonymous reviewers; Roger Watson, Professor of Nursing, University of Hull; and Sarah Oerther, Nursing Instructor, Saint Louis University for valuable criticism. The authors wish to acknowledge the financial support of the National Science Foundation award numbers 0538532 and 1102690; the John A. and Susan Mathes Endowment from Missouri S&T; the University of Missouri South Africa Exchange Program; the Schowalter Foundation; and the Conflict and Development Foundation of Texas A&M.
Because the CBPR approach is a partnership with shared ownership of result, it is important to acknowledge individuals who were co-contributors to the work, including: Dominic Boccelli (University of Cincinnati); Vince Broady (Nexos Locales, Guatemala); Diana Castellanos-Bucey (self-employed, Guatemala); Martin Chapas (self-employed, Guatemala); Devin Cornell (Missouri S&T); Elizabeth Cudney (Missouri S&T); Omar Dary (USAID, Washington, DC); Samuel Ortiz Diaz (self-employed, Guatemala); Elizabeth Dixon (University of Cincinnati); Tommy Goodwin (Missouri S&T); Coretta Jonah (University of the Western Cape, South Africa); Tomas Leon (self-employed, Guatemala); Baudilio Lopez (USAID, Guatemala); Julian May (University of the Western Cape, South Africa); Tom Mboya (self-employed, Tanzania); Doug Momberg (University of the Witwatersrand, South Africa); Christian Ngandu (University of the Witwatersrand, South Africa); Shane Norris (University of the Witwatersrand, South Africa); Connie Paraskeva (Nexos Locales, Guatemala); Ramon Pedro (self-employed, Guatemala); Gerber and Michele Perez (Healthy Communities, Guatemala); Roduel and Hilda Perez (self-employed, Guatemala); Rihlat Said-Mohamad (University of the Witwatersrand, South Africa); Andrew Schranck (Missouri S&T); Alene Seiler-Martinez (USPC, Guatemala); Gil Serique (Amazon River Cruise, Brazil); Matthew Stoker (self-employed, Guatemala); and Paul Succop (University of Cincinnati).
Author Disclosure Statement
No competing financial interests exist.