
Abstract
Aim:
To evaluate safety and efficacy of 5-mm Hem-o-lok clips in children undergoing retroperitoneoscopic nephrectomy.
Material and Methods:
Twenty-four retroperitoneoscopic nephrectomies were performed between September 2004 and August 2007. The indications of nephrectomy were ureteropelvic junction obstruction, reflux nephropathy, ectopic ureteral opening with renal dysplasia, and stone disease with pyonephrosis and primary obstructed megaureter with renal dysplasia. Nine cases were on right side and others on left side. Multiple 5- or 10-mm Hem-o-lok clips were used to control renal artery and vein separately in each case. The specimen was mobilized and removed either by extension of a port site incision or by a separate incision at ipsilateral iliac fossa at the lateral border of the rectus muscle.
Results:
Hem-o-lok clips were deployed on renal pedicle separately in each case. Two clips were deployed on the body side and one on the specimen side. On the left side lumbar, gonadal and adrenal tributaries were also clipped by 5-mm Hem-o-lok clips. No clip dislodgement was observed in any patient. Mean operative time was 111 (80 ± 47) minutes, and mean blood loss was 25 (10 ± 45) mL. Mean hospital stay was 2.4 (1.9-3.1) days.
Conclusion:
Five- and 10-mm Hem-o-lok clips are safe and effective for renal pedicle control during retroperitoneoscopic nephrectomy in children.
Introduction
Laparoscopic nephrectomy has emerged as a standard of care in adult population. 1 However, there is limited experience of laparoscopic nephrectomy in children. Several methods are described to control the renal artery and vein during laparoscopic nephrectomy, including titanium clips, Hem-o-lok clips, staplers, and vessel sealing systems like Ligasure and suturing. 2 -5 Safe pedicle control is the key point of laparoscopic nephrectomy, and at present the best method of pedicle control is not clear in pediatric patients undergoing laparoscopic nephrectomy. We present our experience of control of renal artery and vein by 5- or 10-mm Hem-o-lok clips during retroperitoneoscopic nephrectomy in children.
Materials and Methods
We retrospectively analyzed 24 retroperitoneoscopic nephrectomies in children performed between September 2004 and August 2007. The youngest child was 1.8 years old. Table 1 shows age distribution, and Table 2 shows etiology for nonfunctioning kidney. Five children had pyonephrosis (four with renal stones and one with ureteropelvic junction obstruction) and had percutaneous drain tube placement before subjecting for nephrectomy. Decision of performing nephrectomy was based on renal scan showing glomerular filtration rate less than 10 mL/min. Preoperatively, children were kept nil per orally for 4 to 6 hours. Following method was used to operate patients.
Age Distribution
Etiology of Nonfunctioning Renal Unit
Surgery was carried out under general anesthesia with an endotracheal tube insertion. Patient was secured in lateral position. Warmer was used to keep the body temperature within normal limits. Three 5-mm ports were used for retroperitoneoscopy; the first port was placed by open access to the retroperitoneum by making 1-cm-long incision to skin only. Muscle fibers were split, and dorsolumbar fascia was opened by scissors. A peanut was used to create a space in the retroperitoneum to place the balloon, and balloon was inflated (20 mL of saline/kg of body weight) to create an adequate space to place other ports under laparoscopic guidance. An anterior 5-mm port was placed at anterior axillary line, and a posterior 5-mm port was placed at the renal angle. In three older children, instead of a 5-mm port, a 10-mm port was placed at the renal angle to deliver 10-mm
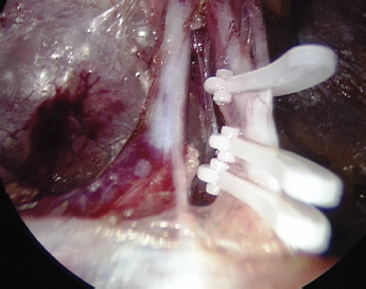
Multiple 5-mm Hem-o-lok clips on the renal artery.
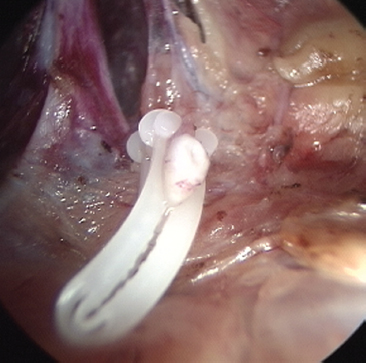
Divided end of renal artery. Note that vessel is close to the locking.
Results
The procedure was successful in 23 patients, without conversion to open surgery. Two patients had accessory renal arteries found intraoperatively that were clipped and divided. In one patient with calculous pyonephrosis pedicle could be dissected and controlled by Hem-o-lok clips, but kidney was adherent to peritoneum medially and there was potential threat to traction injury to duodenum and right colon during kidney mobilization; hence, terminal part of procedure was converted to open surgery. Operative time was defined as time of making the incision for port placement till the closure of all the wounds. Mean operative time was 111 (80 ± 47) minutes, and mean blood loss was 25 (10 ± 45) mL. Mean time to start oral intake was 5.3 hours (range, 4-8.3), and mean hospitalization was 2.4 days (range, 1.9-3.1). In one patient injury to peritoneum occurred during kidney mobilization, but the procedure could be completed without conversion to open surgery.
Multiple 5-mm clips were used in 20 patients and 10-mm clips were used in others for control of renal pedicle. None of the clip was displaced after application. However, on three occasions, a 5-mm clip was self-locked while passing through a 5-mm port before deploying on the vessel.
Discussion
The renal hilum deserves the special consideration during laparoscopic nephrectomy. 6 Several methods have been used to control the renal artery and vein during laparoscopic nephrectomy in adults. The most commonly used method of venous control in adult patient is use of stapler. In small children, however, due to the small size of the ports and small caliber of vein, bulky staplers are cumbersome to use for control the renal pedicle. The jaw length of stapler is long, and sometimes there is no adequate space in retroperitoneum to deploy it. This raises concerns about the safety of various other methods of controlling the renal pedicle. Titanium clips, Hem-o-lok clips, vessel sealing system, and suturing of the pedicle are the other options.
Transfixation of renal vessels by suture is the most secure method of controlling the renal pedicle during open surgery. However, the laparoscopic suturing skill in small working space in children could be a demanding and time-consuming task and may risk bleeding. 5,7
The nonlocking titanium clip applier often gets jammed and does not deliver the clips. 8 The clips applied often form scissor-like closure at the tip, while the shaft and ‘‘U''-turn part show gap between the two arms of clips, and hence it may not work as hemostatic. 8 Falling off of metallic clips after their deployment is known. Titanium clip slippage that resulted in catastrophic complications, including death, had been reported. 9,10 The Auto Suture Endo Clip disposable clip applier (US Surgical, Norwalk, Connecticut) package insert indicates that this device must not be used on the renal artery for primary vascular hemostasis. 11
In porcine model LigaSure® (Valleylab, Boulder, CO) vessel sealing system is a viable option for control of arteries upto6mmandveinsupto12mmindiameter. 12 However, it causes peripheral tissue damage up to 2 to 3mm. Further, thermal damage is more extensive in the vein than in the artery. 12,13 The right renal vein is short, and the renal artery is in close relation to inferior vena cava. Hence, this device should be used with caution especially during right-side laparoscopic nephrectomy, where inadvertent lateral thermal damage to inferior vena cava may occur. There is limited clinical experience of vessel sealing device use in pediatric nephrectomy. 5 In an animal model, failure of vessel sealing system during both open surgery and laparoscopic surgery has been demonstrated, demanding further improvement in sealing system. 14 Vessel sealing system may be suitable for smaller-size renal vessels, but larger vessels must be controlled by methods other than vessel sealing system.
Hem-o-lok clip has teeth within its jaws to ensure tissue security, and locks firmly in place. Safety of Hem-o-lok clip has been tested to control the renal artery both in physiological and supraphysiological conditions in a laboratory model. 15 In an experimental model, the mean bursting pressure of Hem-o-lok clip and titanium clip was found to be above 1200 mm Hg, while that of linear cutting stapler was about 260 mm Hg; application of two Hem-o-lok clips with 2-mm cuff of the artery was not associated with failure of Hem-o-lok clip. 16 The mechanisms of failure of titanium clip, Hem-o-lok clip, and stapling device were, however, different. 16 In another experimental study, Lamberton et al 17 have found that the bursting pressure of harmonic scalpel, Ligasure, Gyrus PK, and EnSeal to seal 5-mm bovine artery is less than 400 mm Hg. Landman et al, 12 in a porcine model, found Ligasure failure before both titanium clips and a stapler devices. These experiments have proved that the bursting pressure of Hem-o-lok clip is superior to stapling devices and any energy used as a vessel sealing system.
In a clinical setup, a 5-mm Hem-o-lok clip can control renal artery in children easily. Further, caliber of the renal vein is not a problem since renal vein blood flow reduces markedly after clipping of the renal artery. Further, elevating the kidney by a retractor stretches and empties the renal vein, which reduces the caliber of vein. We did not find any difficulty in deploying a 5-mm Hem-o-lok clip on renal vein in small children. In older children, instead of a 5-mm port, we preferably place a 10-mm port at the renal angle and deploy 10-mm Hem-o-lok clips. Observation of the locking tip of the clip around the vessel before final deployment, narrow profile, resistance to closure when intervening tissue is present at the level of jaw of the clip, the tactile feedback, and peculiar clicking sound of the locked jaw at the time of application help in making this clip user-friendly and safe.
Locking clips were reported to malfunction in 18 reports according to the U.S. Food and Drug Administration. 8 In 2006, Teleflex Medical issued a warning stating that Hem-o-lok clips are contraindicated in the control of the renal artery during laparoscopic donor nephrectomy after publication of the recall survey by Friedman et al. 9 The common problems with the clips are as follows: it dislodges from the applier, it gets caught up in adventitial tissue easily, and the locking mechanism can lock even if it is passing through tissue; the latter is the most likely mechanism of most failed clip applications. Dissection of the renal vessels completely off the surrounding tissue, avoiding the surrounding tissue, while applying the locking clips, observation of locking mechanism during application of clips, and leaving behind 1 to 2 mm of tissue of the vessel adjacent to the deployed clips are necessary steps to prevent failure of the locking mechanism of Hem-o-lok clips. A more recent multiinstitutional retrospective review on 1600 nephrectomies performed using Hem-o-lok clips on renal artery and few cases in renal vein did not show failure in a single case, and authors have concluded that, despite manufacturer's release of contraindications, when applied correctly by laparoscopically trained urologists, Hem-o-lok clips are safe, effective, and reliable for use in all types of laparoscopic nephrectomies. 18
In conclusion, in our initial experience, 5-mm self-locking Hem-o-lok clips are safe and effective for vascular control of the kidney during simple nephrectomy in children. Clips can be applied through 5-mm ports and hence postoperatively give better cosmetic appearance.
Footnotes
Disclosure Statement
No competing financial interests exist.