
Abstract
Background and Purpose:
To decrease intraoperative and perioperative morbidity that is associated with laparoscopic partial nephrectomy (LPN), clamping of the renal hilum has been advocated. It has been suggested, however, that renal hilar control is not necessary in all patients. We compared the perioperative and pathologic results of 21 consecutive patients who underwent LPN with or without renal hilar clamping at our institution.
Patients and Methods:
Twenty-one patients underwent LPN over a 24-month period. Of these, 11 LPNs were completed without hilar control while 10 needed hilar clamping. Renal hilar control was deemed necessary if the depth of tumor invasion was greater than 50% of the renal parenchyma on CT or MRI. Only the artery was clamped. We retrospectively analyzed the intraoperative, perioperative, and the pathologic results.
Results:
The mean tumor size was 2.6 cm (range 0.8–4.2 cm) in the nonclamped group and 2.3 cm (range 1.5–3 cm) in the clamped group. The mean operative time was 174 minutes (range 95–270 min) in the nonclamped group and 232 minutes (range 180–270 min) in the clamped group. The mean ischemia time was 29 minutes (range 21–45 min) in the clamped group. The mean postoperative serum creatinine level was 1.1 mg/dL (range 0.7–2.0 mg/dL) in the nonclamped and 1.1mg/dL (range 0.7–1.8 mg/dL) in the clamped group. Postoperative transfusion was not needed. In one patient in the nonclamped group and in three patients in the clamped group, urine leak occurred. In the nonclamped group, 7 of the 11 procedures were for benign tumors while only 2 of the 10 lesions in the clamped group were benign.
Conclusions:
LPN can be performed safely in selected patients without clamping the hilum. Tumors that need cross-clamping of the renal hilum were more likely to be malignant. We suggest that the decision to clamp the hilar vessels should be made based on each patient's characteristics and radiologic findings.
Introduction
Although open partial nephrectomy has demonstrated acceptable oncologic control, the associated perioperative morbidity can be significant. With the advent of laparoscopy, laparoscopic partial nephrectomy (LPN) has gained acceptance among urologists as a viable alternative to the open approach because of decreased perioperative morbidity. Nevertheless, LPN is still performed at limited institutions because of many technical challenges.
One of the major controversial issues in LPN is the question of renal hilar vascular control. Although cross-clamping the renal hilum leads to decreased blood loss and better oncologic control, 5,6 this technique is also associated with increased renal ischemia and renal failure. Thus, some surgeons have argued that cross-clamping of the renal hilar vessels is not always necessary. Indeed, it has been reported that exophytic lesions can be safely removed laparoscopically without controlling the renal hilum. 7 –9 During the last 2 years, our institutional philosophy has been to avoid cross-clamping the renal vessels, if possible. Here, we report our experience.
Patients and Methods
Patients
Approval from the Institutional Review Board at The Cancer Institute of New Jersey/Robert Wood Johnson Medical School was obtained for this retrospective study. From January 2006 to December 2007, charts of all patients who underwent LPN at The Cancer Institute of New Jersey/Robert Wood Johnson Medical School were reviewed retrospectively. A total of 21 patients with small renal tumors underwent LPN by one surgeon (IK). Of these, 11 LPNs were completed without hilar control (group 1) while 10 needed hilar clamping (group 2). Patient characteristics are compared in Table 1.
BMI = body mass index; SD = standard deviation.
Surgical technique
The decision concerning renal hilar control was made based on imaging studies. If the depth of tumor invasion was greater than 50% of the renal parenchyma on CT or MRI, the renal artery was cross-clamped; the renal vein was not clamped in any patients (Fig. 1). Because of the potential for significant blood loss, the renal artery and vein were exposed in all patients. In patients in group 1, the renal mass was resected using a harmonic scalpel. An argon beam coagulator (ABC) was then used to obtain adequate hemostasis. Subsequently, hemostasis was obtained using the sandwich technique. 7 Briefly, Floseal (Baxter Corp, Deerfield, IL) followed by Surgicel (Ethicon, Somerville, NJ) followed by Tisseel (Baxter Corp, Deerfield, IL) is applied.
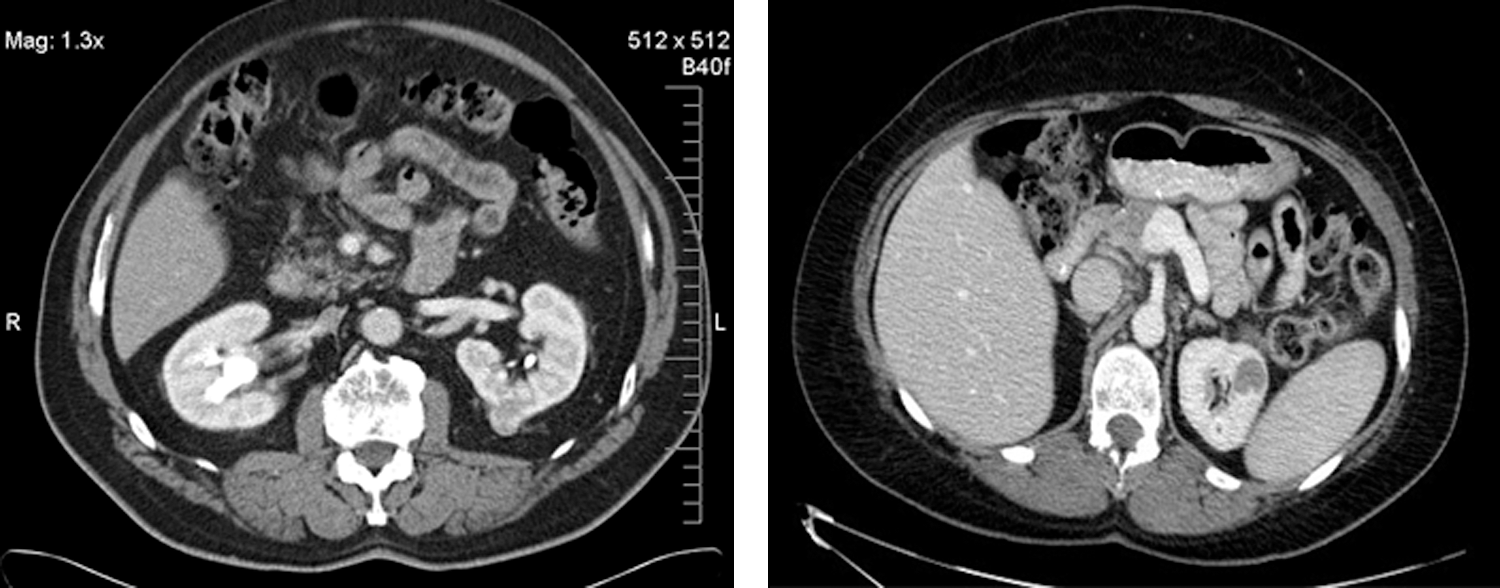
Representative CT scans. The right panel shows a tumor with less than 50% involvement of the renal parenchyma while the left panel shows a tumor with more than 50% involvement of the renal parenchyma. Final pathology findings demonstrated that both tumors were clear cell renal-cell carcinoma.
When renal hilar control was deemed necessary, renal artery was cross-clamped using a laparoscopic bulldog. The renal mass was then resected using cold scissors. Hemostasis was then obtained at the tumor bed using the ABC. Next, 3-0 polyglactin suture was used to oversew the bottom of the tumor bed. One application of Floseal was applied followed by the placement of a Surgicel cigar roll. The defect in the kidney was closed over using 2-0 polyglactin suture followed by one application of Tisseel. Laparoscopic bulldog clamp is then removed.
After achieving adequate hemostasis, the tumors were entrapped in a specimen retrieval bag and sent out for frozen section analysis. Surgical margins were determined in all cases on the tumors themselves. Once a pathologist confirmed a negative surgical margin, a drain was placed, and all ports removed. Because only dilating trocars are used in our operating rooms, the fascia was closed only for 12-mm port sites lying over the midline. For all other ports, only skin was closed.
Data collection and statistical analysis
Charts of all 21 patients were reviewed retrospectively. The perioperative parameters, including operative time, blood loss, transfusion rate, surgical margin status, and complication rate, were obtained and compared. Final diagnosis and the pathologic stage were obtained from the pathology report. Statistical analysis was carried out using analysis of variance and considered statistically significant if P ≤ 0.05.
Results
As shown in Table 1, the mean ages were 58.0 years (standard deviation [SD] 15.1) in group 1 and 63.7 years (SD 12.4) in group 2. Body mass index—mean 28.8 kg/m2 (SD 4.7) and mean 29.6 kg/m2 (SD 4.9) in groups 1 and 2, respectively—and mean tumor size —2.62 cm (SD 1.40) and 2.31 cm (SD 0.24) in groups 1 and 2, respectively—were not significantly different between the two groups.
Intraoperative parameters are shown in Table 2. The mean operative time was significantly longer in the cross-clamped group than in the nonclamped group (232 min vs 174 min, P = 0.007). Estimated blood loss was similar between the two groups (159 ml vs 165 ml in groups 1 and 2, respectively). No patients needed intraoperative or postoperative transfusion. The mean ischemic time in group 2 was 28.9 min (SD 7.65). In one patient in the cross-clamped group, intraoperative frozen-section analysis demonstrated a positive surgical margin. In this patient, the surgery was converted to a radical nephrectomy. Reclamping of the renal artery is avoided at our institution because of the concern for reperfusion injury.
Hb = hemoglobin; Cr = creatinine; SD = standard deviation.
A total of four complications occurred: One patient in group 1 and three patients in group 2. All were urine leaks. These patients were treated initially using a Foley catheter and ureteral stent. In all four cases, the urine leak persisted after 2 weeks. Thus, percutaneous nephrostomy (PCN) tubes were placed and ureteral stents were removed. The urine leak resolved in all patients with a mean time of 6 weeks after surgery (4 weeks after PCN placement). Mean preoperative and postopoperative hemoglobin and creatinine levels were not significantly different between the two groups. There was no meaningful difference in the average hospital stay length (2 vs 2.5 days)
In the nonclamped group, the pathologic findings were renal-cell carcinoma (RCC) in two patients; the final diagnosis in the remaining nine patients was angiomyolipoma in three, oncocytoma in four, benign cyst in one, and lymphoma (Table 3). In the clamped group, all were RCC except one (oncocytoma). The stages of all malignancies were T1a except for one case of T1b (4.2 cm) in group 1. The overall rates of carcinoma were 18% and 90% in groups 1 and 2, respectively.
RCC = renal-cell carcinoma.
Discussion
Multiple investigators have reported the benefits of clamping the renal hilar vessels in LPN. 5,10 These advantages include decreased blood loss and lower incidence of positive surgical margins. Thus, many have argued for the routine clamping of the renal hilum during LPN.
Despite the apparent benefits of renal hilar control during LPN, there are few obvious drawbacks. First, isolation and gaining complete control of the renal hilar vessels are technically challenging. As a result, the learning curve of LPN using this technique may be too steep for many surgeons. Second, after cross-clamping the renal hilum, the surgeon has a finite length of time to resect and obtain adequate hemostasis. The usual recommended maximal warm ischemic time during LPN is 30 minutes, based on reports by Desai and associates. 11 Finally, the long-term effect of clamping the renal artery is uncertain.
Based on these disadvantages of cross-clamping the renal hilar vessels, some have argued that LPN can be performed safely in some patients without hilar control. Andonian and colleagues 12 suggested that the “no hilar clamping” technique may be applicable for small exophytic renal masses that are less than 1 cm from the surface. Stolzenburg and Liatsikos 13 performed LPN without clamping the hilum for exophytic tumors that were no larger than 2 cm. In the present study, we report that LPN can be safely completed without clamping the renal vessels if the depth of invasion is less than 50% of the renal parenchyma.
The obvious advantage of the nonclamp technique is that warm ischemia is avoided. It has been reported that irreversible renal damages start occurring during partial nephrectomy when the warm ischemia time is longer than 30 minutes. 14 More recently, warm ischemia time cutoff of 40 minutes has been suggested. 15 Regardless, it is intuitive that longer ischemic time will correlate with poor renal function. Thus, it is our institution philosophy to avoid renal clamping if possible.
Because of the perceived risks of warm ischemia, many urologists at various institutions have studied and developed various surgical techniques that permit partial nephrectomy without hilar clamping. Specifically, Gruschwitz and coworkers 16 from Germany reported on the safety and efficacy of laser-supported partial nephrectomy in five patients while Andonian and associates 17 published the initial experience with the Habib laparoscopic bipolar radiofrequency device in three patients. In addition, the safety of the TissueLink device was reported in 11 patients. 18
A careful inspection of the results demonstrated that the operative time for the nonclamped group was significantly shorter by ∼1 hour. This increased operative time in the cross-clamped group is likely for two reasons. First, when cross-clamping iss necessary, a more meticulous dissection of the renal hilum was carried out. This part of the surgery is routinely performed by resident urologists and takes 30 minutes on average. Second, in the cross-clamped group, additional time is necessary for reconstruction/repair of the renal defect. This is reflected in the average cross-clamp time (warm ischemia time) of 28.9 minutes.
A comparison of the pathology reports between the two groups revealed surprising findings. Specifically, the incidence of carcinoma was significantly less in patients who did not need clamping of renal hilum (18% vs 90% in clamped group). This observation is consistent with that reported by Venkatesh and colleagues 19 in which the incidence of malignancy increased with deeper depth of invasion in small renal masses. Nevertheless, additional studies are necessary for confirmation of this concept.
Although the complication rates in both groups were comparable and no transfusion was necessary in both groups, there was a slightly higher incidence of urine leak in the clamped group (three vs one in the nonclamped group). Compared with published reports, the overall urine leak rate of 19% seen in the current report is significantly higher. Indeed, Breda and coworkers 20 recently reported urine leak rates after LPN in the literature to be 1.4% to 2.0%. The reason underlying the much higher urine leak rate in our series is unclear. Based on the analysis of the results, however, it is likely that the urine leak rate after LPN will vary from series to series, depending on the proportion of endophytic tumors.
Consistent with this concept, Meeks and colleagues 21 reported in their series of 127 patients that the overall urine leak rate was 13.3%. A more detailed breakdown of this series showed that the urine leak rate was higher in patients who needed open partial nephrectomy than in those undergoing LPN (18.5% and 10.5%, respectively). Because open partial nephrectomy is usually performed for deeper and larger renal tumors, the higher urine leak rate after open partial nephrectomy likely represents the higher complexity of the tumors.
When urine leaks develop after partial nephrectomy, it usually necessitates an extended period of urine drainage. Indeed, in an analysis of 21 patients with urine leak after partial nephrectomy, the mean duration was 53 days (range 5–240 d). In the current study, the mean duration of urine leak was 6 weeks. All urine leaks were initially managed with ureteral stent and Foley catheter. Urine leak persisted more than 2 weeks in all cases with this management strategy, however. Subsequently, a nephrostomy tube was placed, and the ureteral stent and Foley catheter were removed. In all patients, the urine leak resolved within 4 weeks following the placement of PCN. Based on this experience, we recommend an early placement of a nephrostomy tube in patients with urine leak after partial nephrectomy. At our institution, we now place PCN in patients with urine leak that lasts longer than 1 week.
The estimated blood loss was not significantly different between the two groups. Published reports have suggested that cross-clamping the renal hilum results in lower blood loss. Thus, the apparent inconsistency between the literature and the current manuscript is likely threefold. First, when cross-clamping, only the renal artery was controlled; the renal vein was left un-clamped. This may result in significant backflow of blood. Indeed, it has been reported that clamping the artery only, as opposed to controlling both the artery and vein, resulted in increased blood loss while providing better renal function during LPN. 22 Second, more complex and deeper tumors were in the cross-clamp group. More recently, we have started cross-clamping both the renal artery and renal vein. A detailed analysis after a sufficient surgical volume will likely prove or disprove the impact of artery-only clamping on blood loss. Third, the incidence of benign tumor in the nonclamped group was 64% in our series. Because benign renal tumors, as opposed to RCC, may have decreased vascularity, the relatively lower blood loss in the nonclamped group may be a mere reflection of the high incidence of benign tumors in the current series. Additional studies are necessary to verify this concept.
Conclusion
LPN can be performed safely without hilar control in selected patients. Depth of tumor invasion may correlate with incidence of malignancies in patients with small renal tumors.
Footnotes
Disclosure Statement
No competing financial interests exist.