
Abstract
Purpose:
We assess the safety, efficacy, and cost of the novel long-term indwelling thermo-expandable Memokath ureteral stent for the management of malignant and benign ureteral strictures.
Materials and Methods:
Since October 2004, we treated 73 patients (34 men), ages 23 to 84 years (mean 57.7) with 86 ureteral strictures (13 bilateral) with the Memokath™ 051 stent. The causes of the strictures were benign in 55 cases and malignant in 31 cases. Follow-up included radiography, renal ultrasonography, and renography if needed after 2 weeks, 3 months, and then every 6 months.
Results:
The mean operative time was 23 minutes, while the mean hospital stay was 1.5 days. The average indwelling time of an individual Memokath was 11.2 months. After a mean follow-up period of 17.1 months, there were 68 stents in situ. In 12 cases, spontaneous resolution of the ureteral stricture was revealed after a mean indwelling time of 9 months. The remainding six cases were treatment failures. In 15 cases, because of late complications, a Memokath exchange took place after a mean period of 18 months. A total of 26 complications were revealed after the insertion of 102 Memokath stents. These included six cases of urinary tract infections; 15 stent manipulations were needed because of stent dislodgement, and 5 stents were removed because of encrustration and blockage. In the long term, the overall costs for the Memokath treatment and follow-up were considerably less than with the conventional Double-J stent.
Conclusions:
The ureteral Memokath stent is a promising, safe, and efficient treatment option for the minimally invasive management of both benign and malignant ureteral strictures.
Introduction
In this study, we assess the safety and efficacy of a novel long-term indwelling thermo-expandable ureteral stent for the management of malignant and benign ureteral strictures and present relevant technical tips.
Materials and Methods
The ureteral Memokath stent
The Memokath™ 051 stent (Pnn Medical A/S, Kvistgaard, Denmark) is a thermo-expandable nickel-titanium alloy spiral ureteral stent. 2 The structure of one of these components is floppy, while the other one is rigid, resulting in a thermosensitive “shape memory” (ie, a deformed piece of alloy is restored to its original shape by increased temperatures). The Memokath softens at temperatures below 7° to 13°C and returns to a preformed shape when warmed to a temperature above 55°C. When the Memokath is inserted in the desired location, it is flushed with heated sterile water at 55° to 65°C, which causes it to expand and anchor on the top of the stricture. The Memokath has a shaft diameter of 10.5F and its fluted proximal end expands to 20F. Available lengths are 30, 60, 100, 150, and 200 mm (the length of the double-fluted–ended stent is 200 mm).
The Memokath has a tight spiral structure that prevents urothelial in-growth between the coils. Its spiral construction allows adaption to the natural curves of the ureter, and the resulting lack of outward pressure lessens the risk of secondary ischemic injury to the ureteral wall. Furthermore, the titanium component resists corrosion in the urinary tract. 2 These characteristics allow easy insertion and removal of the Memokath.
Insertion technique and technical tips
The Memokath is inserted after the exact length and position of the ureteral stricture are assessed by retrograde and/or anterograde contrast studies. Traditionally, the upper and lower ends of the stricture are marked and measured between two metal markers on the skin of the patient's abdomen. 2 Initially, a dilator-insertion sheath is inserted over a guidewire previously passed through the stricture. The guidewire and the inner dilator are removed so the Memokath can be inserted into the sheath, which remains just above the proximal end of the stricture. The sheath is then retracted so that the entire stent is exposed in the stricture. Once the position of the stent has been adjusted, the inner mandrel is removed and up to 20 mL of 60°C of sterile water is infused until full expansion of the proximal end is achieved. The proximal end opens to a funnel shape, which then rests on the stricture, anchoring the stent.
Contrast studies can confirm correct position and decompression of the upper urinary tract. Also, an anterograde version of the Memokath is available for insertion through a nephrostomy tract, and it is mounted in reverse order to enable identical positioning. 3
We have modified the technique of measuring the length of the stricture after experiencing cases of pelvic cancer in which the deviated ureter was incorrectly measured with the needle markers. Obesity can also render the measurement incorrect. We suggest using a ureteral catheter that is marked with sterile adhesive tape (ie, Steri-strip) when placed in the proximal end of the stricture and when withdrawn to the distal end. Another challenging issue is that when a previously inserted Double-J-stent is removed, it may be impossible to readvance a guidewire because of complete obstruction (usually in malignant strictures). We suggest performing contrast studies and stricture measurement with the help of a double-lumen ureteral catheter over a safety wire.
In cases of proximal strictures with hydronephrosis, the expansion of the proximal end of the Memokath can be insufficient because of dilution of the heated water. We suggest emptying the dilated system through the Memokath assembly set and, if needed, infusing warm water via a ureteral catheter that is positioned in the proximal end of the Memokath.
Removal technique and technical tips
The ease of removing the Memokath is one of the advantages in comparison with mesh metallic stents that allow tissue in-growth (eg, Wallstent). 4 An ureteroscope is inserted to the base of the Memokath, and up to 50 mL of water below 10°C is infused in parallel with cold irrigation. The base of the stent can be grasped with biopsy grasping forceps or with a Dormia basket. 5 The Memokath will uncoil and can be removed easily.
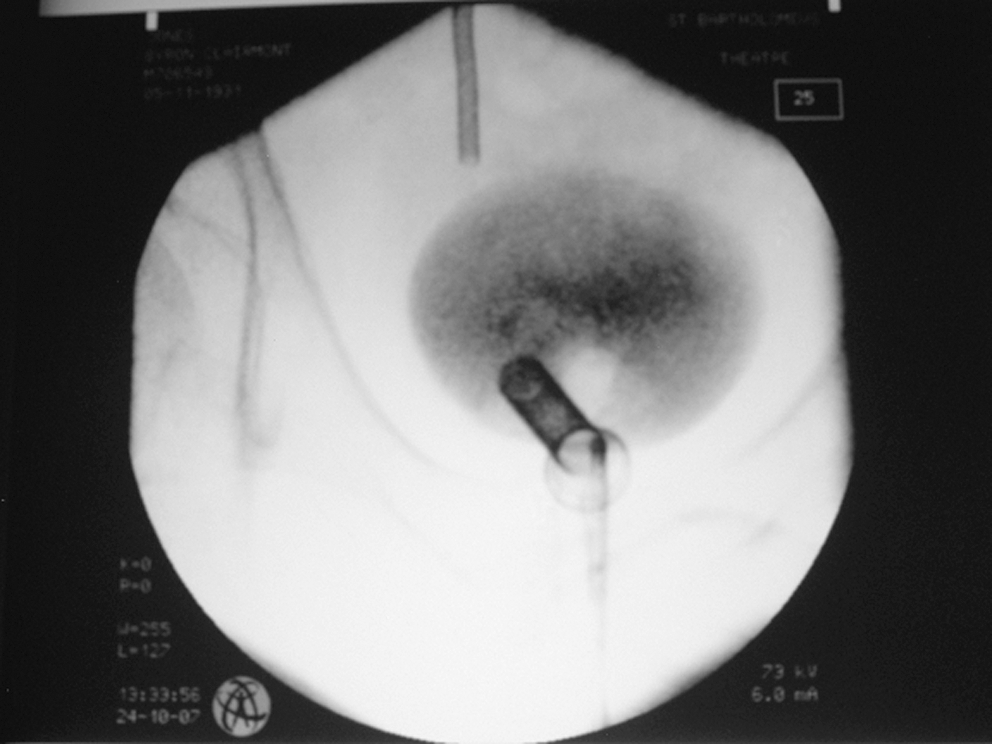
We have modified the removal technique, because we have experienced difficulties in grasping the base of the Memokath with the forceps and the Dormia basket, especially when using a flexible ureteroscope for a migrated Memokath in the kidney. 6 We advance a hydrophilic guidewire through the lumen of the Memokath and insert a balloon dilation ureteral catheter halfway into the Memokath (Fig. 1). The balloon is then carefully manually inflated until it grasps the stent. After cold water (below 10°C) is injected, the stent softens and uncoils, and it is removed as an atraumatic wire.

Removal of the ureteral Memokath stent with a balloon catheter. The black dots represent radio-markers at both ends of the inflated balloon.
Patients
After Institutional Review Board approval, we prospectively studied patients with ureteral strictures who underwent insertion of a Memokath from April 2004 to March 2009. We treated 73 patients (34 men), ages 23 to 84 years (mean 57.7) with 86 ureteral strictures. Thirteen patients underwent insertion of bilateral Memokath stents (Fig. 2). The causes of the strictures were benign in 55 cases and malignant in 31 cases (Table 1).

Bilateral ureteral Memokath stents in a patient with retroperitoneal fibrosis.
CA = cancer.
In all cases, we used a retrograde technique as described above. In one patient with a Double-J stent in situ, we managed to insert the ureteral Memokath through a preexisting prostatic Memokath (Fig. 3). 7 All patients received intravenous antibiotics at induction, followed by a week of oral antibiotics. Our follow-up protocol includes clinical examination, serum urea, creatinine, electrolytes levels, radiography of the kidneys, ureters, and bladder (KUB) and ultrasonography (US) of the kidneys at 2 weeks, 3 months, and every 6 months thereafter. If inconclusive, intravenous urography and/or renal isotope studies were used in single cases. To assess the cost-effectiveness of the ureteral Memokath, we developed a cost-comparison model between the Memokath insertion and conventional Double-J stent insertion and exchange, including costs of material, hospital services, recovery, and follow-up. 8
Memokath 051 inserted into the right distal ureter through an existing prostate Memokath 022 in a patient with prostate cancer, bladder outflow obstruction, and right distal ureter obstruction.
Results
Memokath stents could be inserted in all patients as planned. Mean operative time was 23 minutes (range 17–52 min). No perioperative or immediate postoperative complications were recorded, while the average hospital stay was 1.5 days (range 1–5 d). The average indwelling time of a Memokath was 11.2 months (range 1–39 mos). After a mean follow-up period of 17.1 months (range 1–55 mos), there were 68 (79%) stents in situ. In 12 (14%) cases, spontaneous resolution of the stricture was revealed after a mean indwelling time of 9 months. Six (7%) cases were treatment failures (four cases because of encrustation and two cases because of progressive malignant obstruction), which were managed with reinsertion of Double-J stents and/or open reconstructive surgery. Thus, the overall success rate was 93%.
Fifteen (15%) Memokaths were exchanged after a mean indwelling time of 18 months. Urinary tract infections (UTIs) developed in six (7%) patients, who needed short hospitalization and intravenous antibiotics. In 15 (17%) cases, stent manipulation was necessary because of stent dislodgment and/or blockage. Stent dislodgment was retrograde in 2 cases and anterograde in 11 cases. The Memokaths that migrated in the kidney were removed with flexible ureteroscopy, while the stents that migrated anterogradely were cystoscopically removed and/or exchanged.
In the four cases of Memokath blockage because of encrustration (after a mean period of 6 months), three patients were known stone formers, while the fourth case involved a transplant anastomotic stricture. The encrusted Memokath was removed with ureteroscopy after stone fragmentation with the Lithoclast. In one case in which we used the holmium laser, the Memokath fragmented; hence, the use of a laser is contraindicated because the Memokath is thermosensitive. The transplant patient passed the encrusted stent in the bladder as the stricture spontaneously resolved.
Regarding the 12 cases of spontaneous stricture resolution, the Memokath was expulsed into the bladder in 11 patients (including 2 transplant patients), while in 1 patient, it was passed out unnoticed. Half of these patients reported LUTS. Stricture resolution was confirmed with retrograde contrast studies and did not recur during the regular follow-up. Furthermore, our cases include five patients with anastomotic strictures in transplanted kidneys. One patient went into renal failure because of a blocked stent, necessitating surgical revision, two stents were working fine, and two stents have been passed spontaneously with the stricture resolved.
We have calculated that in the National Health System, a Double-J stent insertion costs 2540 € ($3717). Assuming 6-monthly stent changes and two outpatient follow-ups with radiography of the KUB per year, the total costs to manage a ureteral stricture with Double-J stents is 5512 € ($8180)/year. The insertion of a Memokath necessitates the same infrastructure with the Double-J stent. Additional costs arise from the price of the stent itself and the insertion procedure costs 4762 € ($7067). Together with three follow-up visits in the first year with radiography of the KUB, the total cost in the first year is 5283 € ($7841). Therefore, in the first year, the Memokath can be regarded as cost neutral. Whereas the costs for Double-J stent insertion are repeated at 5512€ ($8180) annually, Memokath patients will only require two yearly follow-up visits with radiography of the KUB at 432 € ($641). Therefore, from the second year, the annual savings with the Memokath are roughly 5080 € ($7539).
Discussion
The successful use of metal stents in the vascular system led researchers to investigate their use in the urinary tract. 9 Four types of ureteral metallic stents have been mainly studied: self- or balloon-expandable, externally coated, and thermo-expandable, such as the Memokath. 9
General experience
Literature on ureteral Memokaths is scarce, and our present series is the largest. 10 –13 Three studies comparable to ours have looked at its use in both malignant and benign strictures. 5,12,13 A total of 148 stents were inserted in 117 patients, of whom 73 (62%) patients had malignant strictures. The mean follow-up ranged from 14 to 20 months. After that period, 40% to 75% of stents were in situ and working, whereas 25% to 60% had to be removed because of failure or complications. Patient data, indications, stricture etiology, and complication type and rates are similar to our own data. This establishes the method and its clinical outcome as reproducible. Strictures close to the pelviureteral junction and long strictures seem to be more prone to stent migration, a clinical observation that we confirm.
Recently, Agrawal and associates 5 compared the cost of the Memokath insertion with the cost of inserting a Double-J stent and reported that these costs are offset if the Memokath stent remains in situ for more than 8 to 12 months. Also, Kulkarni 14 reviewed relevant literature on ureteral metallic stents and concluded that the success of the Memokath is good, in contrast with just fair success of the Wallstent.
Malignant and benign strictures
Memokath stents are of benefit in the treatment of cancer patients with a ureteral stricture who need chemotherapy or as an aid in end-of-life care. Most cancer patients die with the Memokath in situ and without Double-J–related LUTS. In these patients, there is an increasing argument for primary stent placement with the Memokath stent. 15 Data concerning the use of Memokath in benign strictures are rare, and a few studies have reported 67 Memokaths in 61 patients. 16 –18 The stents were placed over 3 to 9 years, with a follow-up of 1.5 to 4.5 years. After this period, 42% to 70% of stents were in situ and working, while 27% to 36% had to be removed because of complications. In contrast to one report that linked malignant strictures with an increased risk of stent obstruction and migration, we did not find any significant differences in benign and malignant strictures in terms of clinical outcome and complications. 17 We concur with other researchers that encrustation is more likely in recurrent stone formers. 16
Transplant anastomotic strictures
Eleven cases have been reported with a mean follow-up of 20 months that comprised determination of creatinine levels and renal transplant US. 3,18,19 Each stent migrated (after 10 days), encrusted (at 13 months), and needed replacement because of UTI (at 14 months). Anterograde insertion and insertion under local anesthesia have been recommended. 3,18
We have inserted Memokaths in five patients with transplants with good results matching those in the relevant literature. With patients under regional anesthesia, we insert a guidewire percutaneously through the transplanted kidney into the bladder; the guidewire will act as our guide to retrograde stent insertion. We do this because we believe that retrograde insertion is less traumatic for the transplanted kidney than percutaneous insertion.
Ureteroileal strictures
In one study, three Memokath stents were inserted for ureteroileal strictures that were refractory to other interventions. 20 Nephrostomy insertion was recommended for anterograde access before inserting the Memokath stent because a retrograde approach may be challenging. 21
Dual-expansion Memokath
Modifications to prevent proximal Memokath migration resulted in a prototype dual-expansion version. Satisfactory results were reported after insertion of such a Memokath in three patients with recurrent benign stricture. 22 Our initial experience after insertion of double-ended full-length Memokaths (Fig. 4) in five patients was encouraging. 11 Patients did not have a higher complication rate than with shorter one-ended stents, and we did not observe any cases of encrustation.

Double-ended full-length 200 mm ureteral Memokath on the left and a 100 mm Memokath on the right in a patient with bilateral ureteral obstruction after radiation of lymph nodes related to gastric cancer.
Conclusions
The Memokath ureteral stent is an attractive long-term and cost-effective minimally invasive management option for both benign and malignant ureteral strictures. It has the advantage of immediate decompression and relief of obstructive uropathy. It bears no risk for bladder irritation, reflux, and flank pain, in contrast to conventional Double-J stents. Also, there is no need for frequent replacement, such as with the Double-J stents, resulting in improvement of quality of life. All patients need long-term regular monitoring, however, because of potential complications.
Several technical tricks of the trade have been developed, making the Memokath insertion, removal, or exchange safe, quick and efficient. In cases of spontaneous stricture resolution, there is no need for reinsertion, provided that patients are closely followed. We discourage the insertion of the Memokath in recurrent stone formers as well as the use of a holmium laser to manage encrustation within the stent. The ureteral Memokath stent is a useful tool in minimally invasive surgery; however, relevant long-term randomized studies are encouraged and warranted.
Footnotes
Disclosure Statement
No competing financial interests exist.