
Abstract
Purpose:
To evaluate the usefulness of laparoscopic surgery in the management of urachal remnants with recurrent infection in infants.
Patients and Methods:
Eight infants (mean age 9.6 months, range 2–16 months) underwent laparoscopic excision of urachal remnants with recurrent infection between June 2006 and December 2008. During the same period, 10 infants (mean age 13.2, range 4–17 months) underwent open surgery for the same condition. The laparoscopic surgery was performed transperitoneally by using three ports. The urachal remnant was dissected from the umbilicus to the bladder dome and then removed completely.
Results:
Immediate complications did not develop in any patient. Blood loss, hospital stay, and operative time with laparoscopic surgery were less than those with open surgery. Recurrence did not develop in any patient who underwent laparoscopic surgery, while it did develop in one patient who underwent open surgery.
Conclusion:
The laparoscopic approach appears to be a safe and effective alternative to open surgery in the management of urachal remnants with recurrent infection in infants.
Introduction
Traditionally, standard surgical management involves the radical excision of the umbilicus along with the urachus and the ventral bladder cuff via an infraumbilical incision, for which a considerably large incision is necessary. Inevitably, the surgery results in a prominent scar, causing considerable disfigurement. On the other hand, laparoscopic surgery is an alternative approach to the complete excision of urachal remnants. This technique is simple and feasible, enabling both sufficient ligation of the urachus and thorough excision of the infected cyst.
Although several studies on the use of the laparoscopic approach for urachal abnormalities have been reported, few of these reports pertain to infants. Here, we report our experience with the laparoscopic approach in the management of urachal remnants with recurrent infection in infants.
Patients and Methods
Patients
Eighteen infants with urachal remnants were referred to our hospital between June 2006 and December 2008. All patients had a history of urachal abscess, and treatment with infraumbilical incision and drainage had failed in all cases. On ultrasonography, a urachal sinus was detected in these patients. Eight infants (mean age 9.6 months, range 2–16 months) underwent laparoscopic surgery, while 10 infants (mean age 13.2, range 4–17 months) underwent open surgery. The surgical approach was selected randomly by doctors. Informed consent was obtained from the subjects' parents, and the study was approved by the Ethics Committee of Shanghai Jiao Tong University.
Laparoscopic procedure
Patients were placed in the supine position, and general endotracheal anesthesia was administered. A nasogastric tube and Foley catheter were placed.
Three trocars were inserted into the peritoneal cavity: A 5-mm trocar at the right midclavicular line at the level of umbilicus was used as an optiview trocar; two other 5-mm trocars inserted in the right upper and the lower quadrant of the abdomen were used as working ports (Fig. 1). Under direct visualization after CO2 insufflation, the urachal remnant was easily identified below the level of the umbilicus. Peritoneal and preperitoneal cysts were resected free of the transversalis fascia using diathermy scissors along with a clamp. Dissection was continued retrogressively along the umbilical ligament to the umbilicus, and excision was performed with retention of the umbilicus. Cystotomy was not deemed necessary in any of the cases with atresia of the portion of the urachal remnant adjacent to the bladder, which was confirmed during the surgical process.
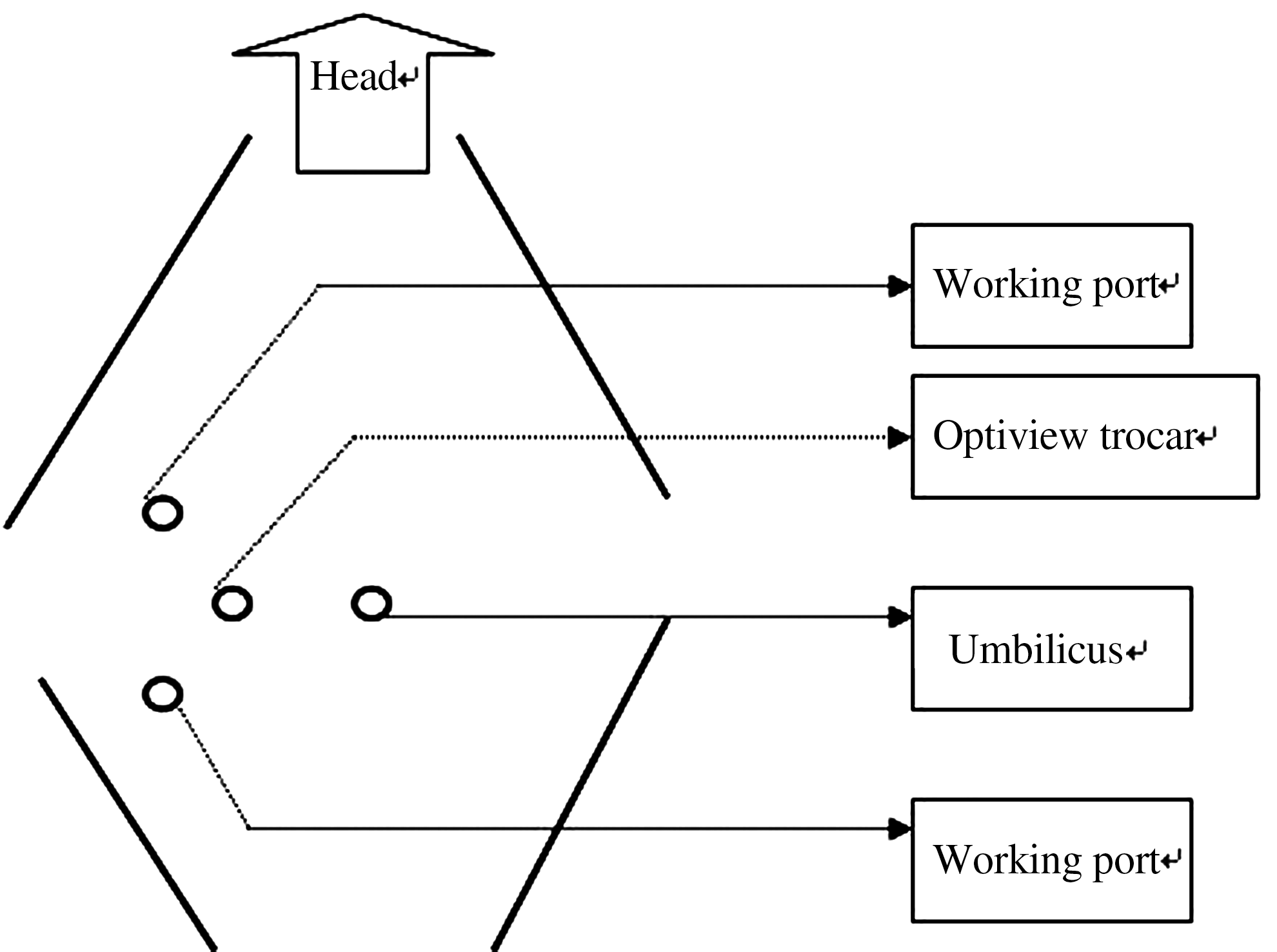
Trocar positions in the process of laparoscopic excision of urachal remnants in infants.
Open surgery
The operation was performed via a suprapubic midline incision. A urachal cyst and the umbilical ligament attached to the umbilicus were resected away from the abdominal wall simultaneously. In most cases, this resection was not necessary. In three patients with a patent urachus, however, excision of the dome of the bladder was necessary. The opening of the bladder was then closed in a running fashion with two layers of sutures (polyglycolic acid 3-0).
Statistical analysis
All data were expressed as mean ± the standard deviation and analyzed with statistical package SPSS 10.0 for Windows. One-way analysis of variance was used to determine statistically significant differences between the groups. P < 0.05 was considered statistically significant.
Results
The mean operative time in the laparoscopic approach was 120 minutes, and there were no cases of intraoperative complications. Recovery in all patients was uneventful, and the patients were discharged on the third day after surgery. The diagnosis was confirmed on pathologic examination.
We compared various aspects of laparoscopic surgery and open surgery. No statistically significant difference was seen between the two approaches with respect to operative time, blood loss, and hospital stay (Table 1, P > 0.05). We have also reviewed recent studies, and a comparison of these findings is provided in Table 2. No contraindications of laparoscopic excision of urachal remnants have been reported.
SD = standard deviation.
NR = not reported.
Discussion
The urachus is a cordlike structure between the bladder and the umbilicus that represents the embryologic remnant of the allantois. The urachal remnant is a rare congenital anomaly, with an incidence of 2 in 300,000 infants and 1 in 5000 adults. 1,2 Various types of remnants have been described, including cyst, sinus, diverticulum, and patent urachus. Infection is the common complication of urachal remnants, particularly in babies. Our experience suggests that acute infections of urachal cysts can be treated mostly by antibiotic therapy and drainage. Blichert-Toft and Nielsen, 4 however, reported a recurrence in 31% of infected cysts that were not excised. The risk of malignant degeneration in the urachus is another indication for surgical management. 3,5
With the introduction of ultrasonography, urachal remnants can be easily diagnosed, thus enabling the administration of early treatment. 6 Surgical treatment of urachal remnants involves the complete excision of the remnant, inclusive of the preperitoneal and peritoneal tissue, with or without the excision of the bladder cuff. 4
The traditional surgical approach for excision of the urachal remnant necessitates a transverse or midline infraumbilical incision. Radical excision necessitates the removal of all structures within the umbilicovesical fascia, including the urachus and the medial umbilical ligament, as well as the associated peritoneum extending from the umbilicus to the bladder dome. 7 Incomplete resection entails the possibility of adenocarcinoma, 8 while excessive resection may unnecessarily result in unfavorable sequelae.
To minimize the morbidity from surgery, postoperative pain, and length of convalescence, the laparoscopic approach was considered for the removal of urachal remnants. All relevant studies have reported the feasibility and effectiveness of the laparoscopic technique for the management of urachal diseases. 9 –13 The largest case series reported on the laparoscopic management of urachal cysts was a retrospective study by Kavoussi and associates. 11 On the basis of these findings, it can be considered that the laparoscopic approach is safe and effective and can be offered as the first-line therapeutic option for patients with urachal remnants.
In our study, this minimally invasive procedure was used in the treatment of pediatric patients. To our knowledge, very few series have been conducted on the use of laparoscopic procedures in young patients. Yamzon and colleagues 14 proposed the use of robot-assisted laparoscopic excision of urachal cysts in pediatric patients. They reported that this approach is a safe and effective option for the minimally invasive management of urachal cysts in children. Instruments for robot-assisted procedures, however, are quite expensive and may not be available in numerous hospitals of developing countries. Reports on traditional laparoscopic techniques in pediatric patients may therefore be useful to many clinicians.
A comparison of laparoscopic procedures and open surgery did not report any significant difference between the two. 15 If complete excision of the cyst can be achieved, recurrence of symptoms can be avoided in all patients, as shown in our series. As the accuracy of diagnosis, we suggest early surgical intervention in patients with a urachal cyst. We believe that the establishment of pneumoperitoneum during the procedure does not have any substantial effect on the movement of the digestive tubes, and neither did the procedure impair the succession of bowel. 10 Early feeding proved to be safe and effective. 16 Without pain and starvation, it seemed that the babies recovered to normal activity very soon. In addition, because the trauma from the operation was minor, parents could easily reassure the babies.
To avoid the advancement of the laparoscope too close to the lesion, trocars were inserted from the right part of the abdomen, instead of at an infraumbilical site. During the procedure, the cyst was excised completely, starting in the reverse direction from the beginning of the bladder upward. This technique seems to be suitable in cases with considerable adhesion. 17 Some authors have recommended the injection of methylene blue into the sinus to clearly identify the boundaries of the cavity. 17 In addition, another obvious advantage of the laparoscopic procedure is that it causes minimal cosmetic disfigurement. With the technologic advances in endoscopic surgical instrumentation and improvement in technical skills, we expect that laparoscopic surgery can be applied increasingly in urachal disease.
Footnotes
Acknowledgments
Some data in the report were collected from Comer Children's Hospital affiliated with Chicago University and Shanghai First People's Hospital. We greatly appreciate their help.
Disclosure Statement
No competing financial interests exist.