
Abstract
Background and Purpose:
During laparoscopic partial nephrectomy, the importance of the initial suture placed under warm ischemic conditions cannot be underestimated. Inadequate hemostasis may lead to further surgical complications. Our goal was to determine which method of sutute ligation (running vs figure-8 interrupted) provides better initial hemostasis when performing partial nephrectomy in an ex-vivo porcine model.
Materials and Methods:
Deep partial nephrectomy defects were cut in the lateral aspect of six porcine kidneys. The renal artery was cannulated, and the kidneys were perfused from a water reservoir. The level (cm H2O) at which parenchymal leakage occurred was measured and recorded in three situations: No parenchymal suture; running suture along the base of the defect; and interrupted figure-8 sutures placed in parallel along the base of the defect.
Results:
Six kidneys were studied. Using interrupted figure-8 sutures, the mean leak pressure was 56.7 cm H2O (over baseline). Using a running suture, the mean leak pressure was 147.5 cm H2O (over baseline). Mean values were compared using two-tailed t test and found to be statistically significant (P = 0.05).
Conclusion:
In an ex-vivo porcine kidney model, use of a running suture along the base of a renal tumor defect (simulating that which is seen during partial nephrectomy) appears to allow for better initial hemostatic control, as compared with interrupted figure-8 sutures placed in parallel.
Introduction
Since the first reported laparoscopic partial nephrectomy (LPN) by Winfield and associates 3 in 1993, LPN has gained acceptance as a means of surgically removing the renal mass while at the same time preserving renal functioning units and minimizing patient morbidity. 4 Comparison between open partial nephrectomy and LPN appears to demonstrate similar outcomes. 5 –7 In addition, decreased morbidity, shorter hospital stay, and faster return to normal physical activity and work are well-documented advantages of LPN over open surgery. 8
LPN is a technically challenging procedure that requires that the surgeon be comfortable with intracorporeal suturing. The primary goals of LPN are: Adequate tumor removal, prompt hemostatic control, and collecting system closure. In this regard, a multitude of techniques have been described, and these descriptions vary as to renal cooling vs warm-ischemia time, tumor excision technique, renal vascular clamping technique, and techniques of hemostatic control. Regardless of whether clamping of the renal vasculature is performed, facile suturing to achieve initial hemostatic control of major vessels is an essential step in LPN.
Our technique is similar to that described by Gill and colleagues. 8 This involves characterizing tumor depth with intraoperative ultrasonography and performing tumor excision with cold scissors under warm ischema with both the renal artery and vein clamped using laparoscopic bulldog clamps. After placement of a running 2-0 polyglactin suture along the base of the defect, the bulldog clamps are released. Methylene blue is injected retrograde through a preplaced ureteral open-ended catheter to identify openings in the collecting system. Hemostatic figure-8 sutures are then placed to close the collecting system and to control any remaining open vessels. The importance of the initial suture placed under warm ischemic conditions cannot be underestimated. Inadequate hemostatic control may lead to further bleeding complications and may hinder complete collecting system closure. Reclamping of the renal vasculature may be necessary, leading to increased nephron damage secondary to repeated ischemia-reperfusion. Our goal was to determine which method (running suture vs figure-8 interrupted) provides better initial hemostasis when performing partial nephrectomy in an ex-vivo porcine model.
Materials and Methods
Porcine kidneys were obtained from Sierra Medical Research, Whittier, CA. The kidneys were warmed to room temperature, and a partial nephrectomy defect was cut in the lateral aspect of each kidney. All defects breached the deep parenchyma and the renal collecting system (Fig. 1). The renal artery was cannulated with a 14-gauge angiocatheter that was connected to a water reservoir via standard intravenous tubing (Fig. 2). Indigo carmine was injected into the water reservoir (1 ampule per liter) to allow for better identification of fluid extravasation.

Porcine kidney with partial nephrectomy defect. The renal artery is cannulated with an angiocatheter.
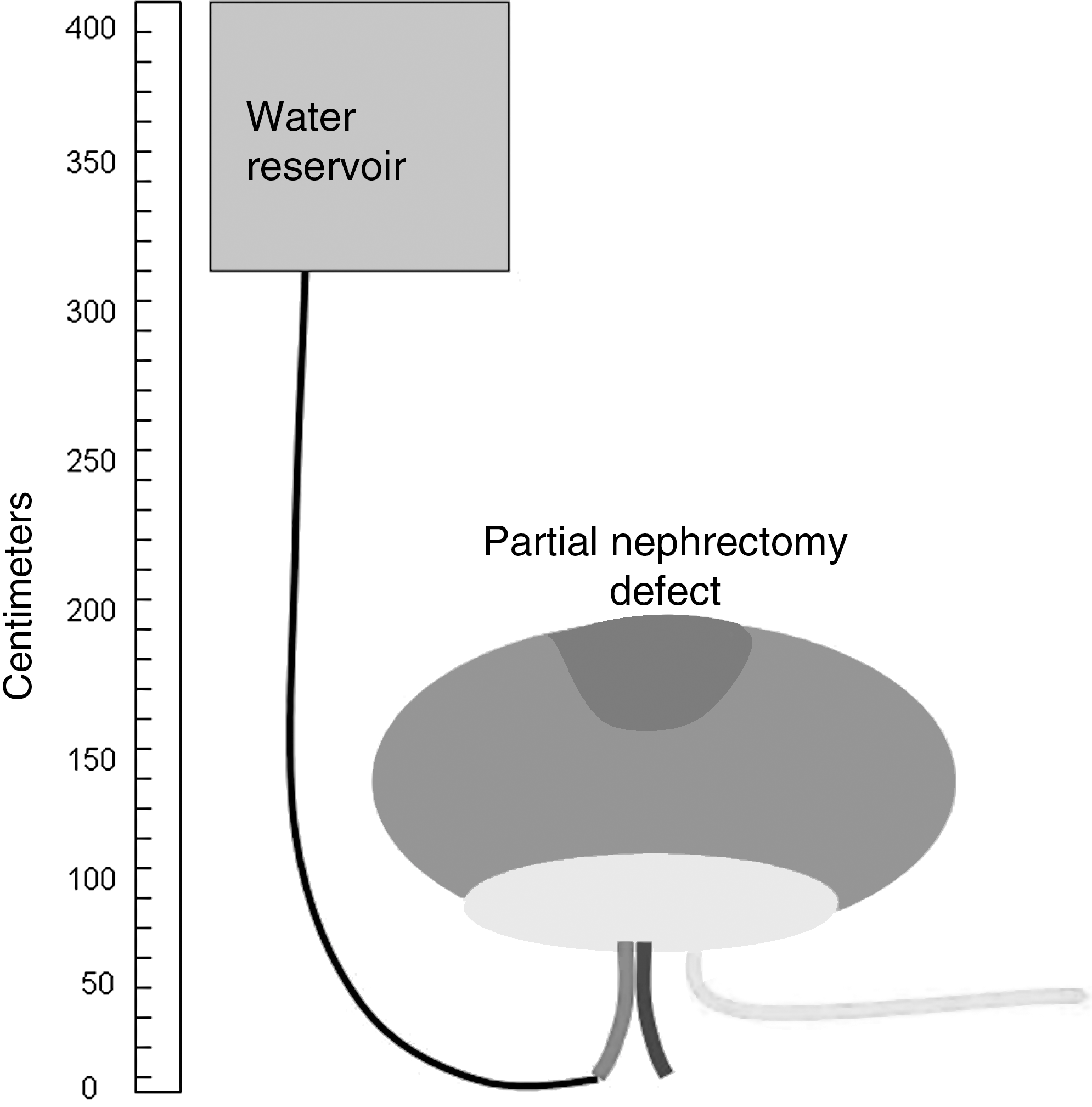
Diagram of experimental setup. The height of the water reservoir was measured above the level of the kidney in centimeters.
The water reservoir was then raised until simulated arterial bleeding was identified within the partial nephrectomy defect. Initially, this was performed for each kidney with no parenchymal suture in place, as a way to establish a baseline reading for each of the six kidneys. The height of the water reservoir was measured (in centimeters) above the level of the kidney. In kidneys 1, 3, and 5, a running 2-0 polyglactin suture/CT-2 needle was placed along the base of the parenchymal defect, and measurements (cm H2O pressure) were recorded. The running suture was then removed, and interrupted figure-8 sutures were placed in series in the same defect. For kidneys 2, 4, and 6, the series of interrupted figure-8 sutures were placed initially, and measurements were recorded. Those figure-8 sutures were removed completely before running the 2-0 polyglactin suture along the base of the defect. Leak pressure was again determined and recorded with the running suture in place. The leak pressure was defined as the point at which blue was seen within the parenchymal defect, representing significant leakage uncontrolled by the initial parenchymal suture placement. 2-0 Vicryl sutures were used throughout the studies, and all needles were size CT-2.
Results
Six kidneys were studied. Measured values for the leak pressure without suture ligation, with running suture ligation, and with interrupted figure-8 suture ligation are summarized in Table 1. Table 2 summarizes the results of the measured value of the leak pressure over the baseline leak pressure for each kidney. The mean leak pressure when interrupted figure-8 sutures were used as the initial method of hemostatic control was 56.7 cm H2O (over baseline). The mean leak pressure when a running suture was used as the initial method of hemostatic control was 147.5 cm H2O (over baseline). The two-tailed t test was used to determine that the difference between the two groups was statistically significant (P = 0.05).
Middle column = [running suture arterial leak pressure] − [leak pressure without suture].
Right column = [interrupted figure-8 suture arterial leak pressure] − [leak pressure without suture].
Discussion
Over the past 15 years, LPN techniques have been refined, and the procedure has been applied for increasingly larger and deeper parenchymal tumors. The major risks of LPN include intraoperative and postoperative hemorrhage and postoperative urinoma formation. Even at high-volume centers, the reported rate of postoperative hemorrhage is approximately 10%. 9 When tumor excision is performed under warm ischemic conditions, facile technique is needed to achieve hemostasis in a timely manner. Inadequate hemostasis when renal vascular clamps are removed can lead to complications, such as inadequate collecting system closure, reclamping of the renal vasculature, conversion to total laparoscopic nephrectomy, or open conversion to achieve hemostatic control.
Minimizing warm ischemia time is important to minimize renal unit damage at the cellular level. When warm ischemia is used during LPN, overall success is dependent on achieving maximal hemostasis of the larger cut vessels during the ischemic period. Pinpoint identification of smaller vessels that need further suture ligation is performed after the renal vascular clamps have been removed. Although we have been using a running suture technique along the base of the kidney defect, there is debate in regard to the best suture technique for best achieving hemostasis. For some surgeons who perform open partial nephrectomy, interrupted figure-8 sutures are used exclusively and are directed at visible open vessels and collecting system. Use of a running suture along the base of the defect became more commonly used when laparoscopic techniques were applied to the partial nephrectomy procedure.
Baumert and coworkers 10 compared two renal closure techniques in vivo during LPN and found that a technique that used a running suture (Baumert technique) did reduce the time needed under warm ischemia and reduced the number of complications. One could theorize that the running suture would be faster and easier to perform in the laparoscopic setting. If, however, our experiment showed that better initial hemostasis were achieved with interrupted figure-8 sutures, our feeling is that the extra warm ischemia time needed to place the interrupted sutures would be a worthwhile sacrifice to be more sure of hemostasis and thereby reduce the risk of having to perform additional maneuvers after removal of the renal vascular clamps.
In our experiment, we did not attempt to replicate the technique used by Baumert and associates, 10 but instead wanted to show an absolute numerical difference between two distinct closure techniques. In effect, each of the six kidneys in our experiment serves as its own control. We were able to demonstrate in an ex-vivo porcine model that use of a running suture along the base of the kidney defect allowed for better initial hemostasis compared with interrupted figure-8 sutures placed in parallel. Our results were statistically significant.
Conclusion
In an ex-vivo porcine kidney model, use of a running suture along the base of a renal tumor defect (simulating that seen during partial nephrectomy) appears to allow for better initial hemostatic control, compared with interrupted figure-8 sutures placed in parallel.
Footnotes
Disclosure Statement
No competing financial interests exist.