
Abstract
Background and Purpose:
Renal artery-only (AO) occlusion, as opposed to artery and vein (AV) occlusion, has demonstrated some benefit in reducing renal insufficiency during warm ischemia. In this pilot study, we used digital light projection hyperspectral imaging (HSI) to construct a “real time” tissue oxygenation “map” to determine whether there are differences in renal tissue oxygenation during vascular occlusion with AO vs AV.
Materials and Methods:
Renal vascular occlusion with either AO or AV was performed for 60 minutes in seven porcine renal units. Using HSI, the percentage of oxyhemoglobin (%HbO2) in the renal cortex was determined at 4-minute increments throughout the ischemic period and for 30 minutes after reperfusion.
Results:
Average baseline %HbO2 in all animals was approximately 70%. After vascular occlusion in both cohorts, %HbO2 decreased by one third within 2 to 5 minutes, with a gradual decline in %HbO2 over the remaining 55 minutes. Oxyhemoglobin profiles for AO and AV occlusion diverged significantly between 16 and 24 minutes after vascular occlusion (P = 0.0001 and 0.036, respectively), with a merging of the two curves occurring after approximately 36 minutes (P = 0.093). During reperfusion, average %HbO2 improved to 72.4% after 25 to 30 minutes.
Conclusion:
In this pilot study, we demonstrate that renal tissue oxygenation drops rapidly after occlusion of the renal vasculature and returns to near baseline 30 minutes after reperfusion. In the porcine model, the %HbO2 differs significantly between AO and AV occlusion for up to 35 minutes after ischemia onset, indicating a possible “ischemic window” in which AO occlusion may provide benefit over AV occlusion.
Introduction
Animal studies from the 1950s and 1960s showed that there is an increased tolerance to ischemia if blood flow is interrupted using artery only (AO) clamping, versus clamping of the artery and vein (AV) together. 7 –9 In 2008, Gong and colleagues 10 confirmed improved postoperative renal function in patients who were undergoing laparoscopic partial nephrectomy during warm ischemia with AO occlusion compared with AV occlusion. Although venous backflow is postulated to be the primary mechanism of renal protection in these patients, improved oxygenation and perfusion has not been confirmed as the mechanism for better tolerance to warm ischemia with AO occlusion.
Hyperspectral imaging (HSI) is a novel technology that uses a highly sensitive camera to measure the visible reflection of light from various tissues. By setting the hyperspectral imager to detect known wavelengths of oxyhemoglobin and deoxyhemoglobin, it is possible to generate a “real-time” map of tissue oxygenation. 11 –13 Previously, this technology has been used to measure tissue oxygen levels in extremities during various types of stress. 12 In addition, a similar technology has been used to demonstrate real-time ischemia during donor nephrectomy. 14 In this pilot study, we used HSI in a porcine model to determine whether differences in renal oxygen delivery during warm ischemia may account for the clinical differences between AO and AV occlusion.
Materials and Methods
After approval by the University of Texas Southwestern Medical Center Institutional Animal Care and Use Committee, four female Yorkshire pigs, weighing between 60 and 80 kg, underwent AO or AV occlusion of each kidney. One renal unit was used at the beginning of the study as a pilot to develop our investigational technique and, therefore, was not included in the analysis.
After induction of anesthesia, the right kidney was approached through an open midline incision, and the peritoneum was mobilized from the anterior surface of the kidney. After exposing the kidney surface, the hilum was dissected free in all animals. Each renal unit was then randomly assigned a clamping technique (AV or AO occlusion), after which each animal received 0.25 mg/kg of mannitol 30 minutes before vascular occlusion. Vascular occlusion was performed using a curved Satinsky clamp for a duration of 1 hour based on previous animal studies demonstrating that ischemic insult to the kidney is universal in porcine kidneys at 60 minutes. 15 After image acquisition and warm ischemia of the right kidney, the identical procedure was carried out on the left kidney (using the opposite occlusion technique). During the procedure, rectal temperature was maintained between 37°C and 39°C, and hemoglobin saturation (as measured by pulse oximeter) was kept between 98% and 100%.
The digital light projection (DLP®, Texas Instruments, Dallas, TX) HSI system uses variable band-passes and center wavelengths to illuminate the kidney with known spectra of light over a wavelength range that incorporates the reflectance spectra of oxyhemoglobin and deoxyhemoglobin (520 nm to 645 nm). Spectrascopic images reflected from the kidney surface are captured by a charge-coupled device (CCD) focal plane array, and the data are formatted into a three-dimensional HSI cube, consisting of two spatial dimensions forming an image and one spectral dimension containing wavelength information. Once the imaging cubes are captured, the data are deconvoluted for percentage of oxyhemoglobin (%HbO2) as the result of a two-step process, which has been described previously. 16
Briefly, the relative percent contribution of each component (oxyhemoglobin and deoxyhemoglobin) is determined at each detector pixel of the CCD by use of a multivariate least squares regression. 1 The resulting chemically relevant visualizations are color-encoded at each image pixel, with various colors representing the relative %HbO2 (Fig. 1).
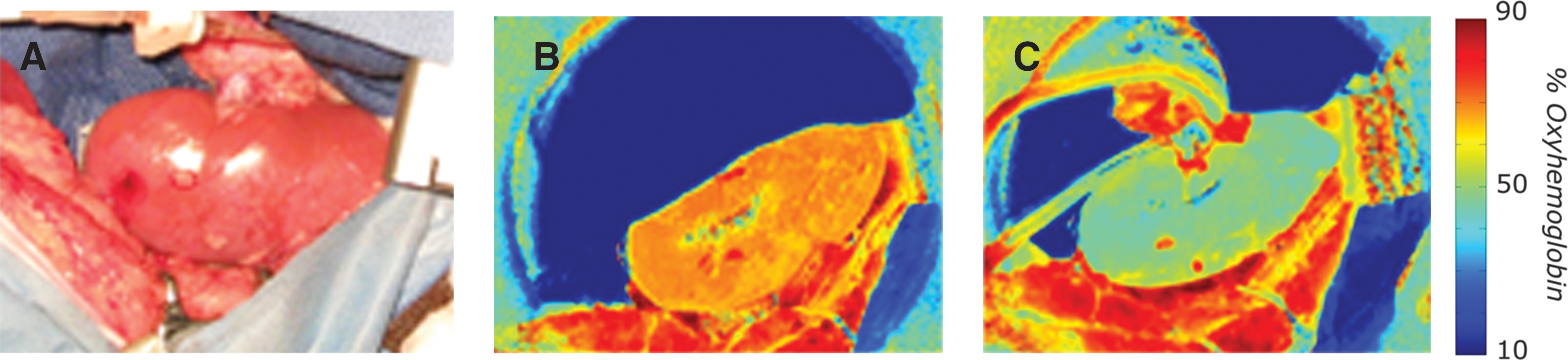
Hyperspectral images (HSI) demonstrate real-time renal tissue oxygenation. (
Statistical analysis was performed postoperatively by a statistician unfamiliar with the hypothesis of the study. The %HbO2 was measured over an 81 pixel area (9 × 9 square pixel region), which was chosen from a uniform surface site in the middle of each kidney, at each time point during the study (“optical biopsy”). An average of the pixels for each region was determined along with a standard deviation for each image cube. Images from each time frame were then grouped as a single data set to determine differences between AV and AO clamping conditions at each of the six periods. Once individual levels were calculated, a regression model was fitted using SAS statistical software (SAS Institute, Cary, NC) to ascertain whether there was a statistically significant difference between clamping methods with regard to renal oxygenation.
Results
Three renal units underwent AO (two right kidneys, one left) and four units underwent AV (two right kidneys, two left kidneys). HSI was performed at 4-minute intervals during vascular occlusion as well as during the reperfusion phase. Acquired images were color coded for %HbO2 at each detector pixel (Fig. 1). As expected, in all cases, baseline (preclamp) images indicated high renal tissue oxygenation as signified by orange-red pixels. After either AO or AV clamping, the real-time visual map of tissue oxygenation demonstrated substantial changes in %HbO2, as indicated by green and yellow pixels.
Before vascular occlusion, the average %HbO2 in all animals was approximately 70% (baseline %HbO2). After vascular occlusion, in both cohorts, %HbO2 dropped rapidly (33%) within 2 to 5 minutes, with a continuous but less severe decline in %HbO2 over the remaining 55 minutes (Fig. 2). While both cohorts (AO and AV) started and ended with similar %HbO2 levels, the techniques diverged significantly between 16 and 24 minutes after vascular occlusion (P = 0.0001 and 0.036, respectively), with a remerging of the two curves occurring at approximately 36 minutes (P = 0.093). After release of vascular occlusion, average %HbO2 improved to 54% after 2 minutes and 72.4% after 25 to 30 minutes.
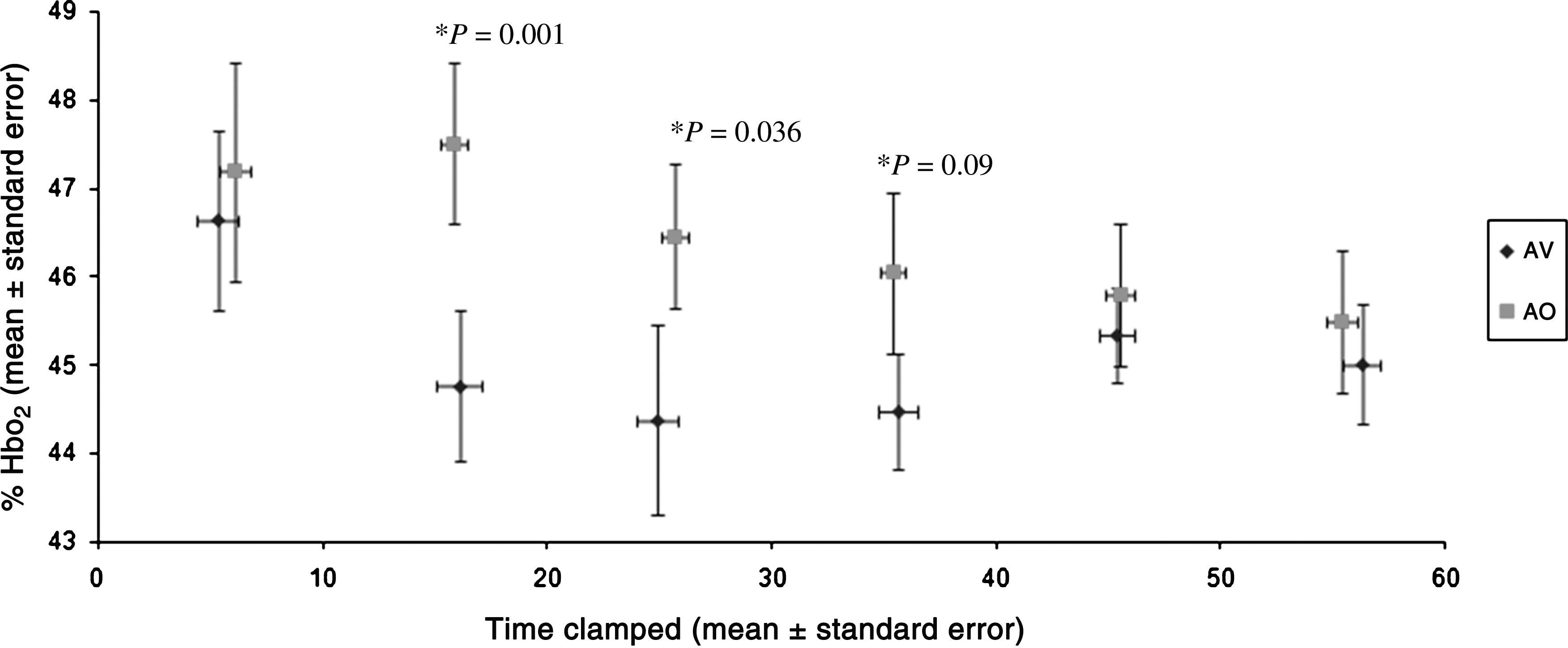
Percentage of oxyhemoglobin (%HbO2) during 60 minutes of vascular occlusion of either the artery and vein together (AV) or the artery alone (AO) in seven porcine kidneys.
Currently available HSI systems rely on liquid crystal tunable filter (LCTF) technology, which needs 40 seconds or more to capture and project an individual specimen. 12,14 By coupling a DLP imaging system with current technology, we were able to decrease image acquisition and processing to less than 30 seconds using 126 successive band-passes of light. Further shortening of the image acquisition to 3 spectral illumination images (“3 shot mode”) allowed us to shorten processing to a near video rate (3–4 frames per second), allowing real-time visualization of ischemic changes.
Discussion
Preservation of the remnant kidney is one of the primary goals during partial nephrectomy. In 1958, Birkeland and associates 8 published the first report on the effect of AO vs AV occlusion and renal cooling on preservation of renal function in a solitary kidney canine model. Using survival as an end point, animals that underwent AO occlusion under hypothermic conditions were able to tolerate ischemia times approximately 60% longer than animals undergoing AV occlusion under similar conditions. Subsequent animal studies during warm ischemia demonstrated improved renal blood flow after 1 hour of AO occlusion compared with AV or vein only occlusion. 7
Recent work by Orvieto and colleagues 17 in a solitary kidney porcine model confirmed renal preservation, as measured by postoperative creatinine level, in animals that were undergoing AO compared with AV occlusion during open warm ischemia, but not in animals that underwent laparoscopic warm ischemia. Although the authors postulated that the difference in outcomes between the open and laparoscopic approaches was a consequence of venous compression from the pneumoperitoneum, a follow-up study that compared occlusion methods during laparoscopic partial nephrectomy in human subjects again revealed that patients who were undergoing AO occlusion had a significantly smaller elevation in postoperative creatinine level than those who were undergoing AV occlusion. 10
Although studies to date have been nonrandomized or performed in animal models, there appears to be a consistent benefit with regard to postoperative renal function in patients who are undergoing AO compared with AV occlusion. The explanation for renal preservation with AO occlusion is unknown, but likely occurs as a result of venous backflow from the unoccluded renal vein, which may allow for: (1) decreased build-up of toxic metabolites and free radicals that develop from ischemic insult; (2) decreased capillary thrombosis because of continuous circulation during the procedure; (3) increased availability of substrate for efficient energy metabolism; and/or (4) improved renal oxygenation from a persistent supply of venous blood.
While several factors may play a role in renal preservation with AO occlusion, tissue oxygen delivery appears to be an essential component. In a canine study that evaluated occlusion methods, Schirmer and colleagues 9 demonstrated that cortical oxygen consumption decreased by 50% at 1 hour with both AO and AV occlusion. While consumption plateaued for up to 5 hours during AO, however, levels continued to decrease to near zero during AV occlusion. Although these results indicate improved oxygen consumption at 1 hour and beyond, they do not indicate whether there are differences in renal oxygen delivery or how tissue is affected during shorter ischemia times that are more typical of contemporary partial nephrectomy.
Using HSI to measure real-time tissue %HbO2 with AO vs AV occlusion, we were able to confirm the results of Schirmer and associates, 9 demonstrating that after 1 hour, tissue oxygenation dropped by approximately 50%. Moreover, although kidneys that were subjected to AO and AV occlusion showed similar absolute declines in %HbO2 after 1 hour of ischemia, there was a significant difference in tissue oxygenation between the two techniques that occurs after the initial 15 minutes and up to 30 to 35 minutes after induction of warm ischemia.
Although the clinical significance of the difference shown in the current study is unknown, it occurs near the typical clinical cutoff point for warm ischemia. 3 Our finding may explain the clinical benefit with regard to postoperative renal function that has been observed in the patients reported by Gong and coworkers 10 when warm ischemia time averaged 33 minutes.
There are several limitations of our study that deserve mention. Studies in a porcine model have demonstrated that permanent renal damage, as measured by decreased glomerular filtration rte (GFR), does not occur until 120 minutes. 18 We chose to use 1 hour of ischemia time as a cutoff for measuring tissue oxygenation, however, based on the fact that all animals undergoing 60 minutes of warm ischemia demonstrate a temporary renal insult. 15 While longer ischemia times may have allowed us to determine an absolute %HbO2 at which renal damage becomes irreversible, our purpose was to demonstrate that there are differences in oxygenation that occur early in the ischemic process (less than 60 minutes) that may be more clinically relevant.
Use of a solitary kidney model and measurement of postoperative serum creatinine may have allowed us to determine whether tissue oxygenation correlates with postoperative renal function. While these data may have added additional information, previous studies in a porcine model have demonstrated consistent renal damage across all animals with both AV and AO occlusion at 1 hour, as measured by a 25% decrease in GFR. 15 Because of the consistent nature of these findings, we did not find it necessary to repeat this portion of the analysis. Furthermore, porcine kidneys have been shown to have a higher tolerance to ischemic insult than human kidneys, 10 so that renal functional declines seen in the porcine model would likely not translate into differences found in humans.
HSI currently relies on illuminating the tissue with very precise spectroscopic light and then processing the light reflected from the tissue surface to determine the relative percentage of oxyhemoglobin perfusing the tissue. While the technology is able to provide a noninvasive optical biopsy of the tissue, the absolute percentage value of oxyhemoglobin represents tissue oxygenation from the microvasculature up to approximately 1 mm within the tissue. Because these values are referenced to oxyhemoglobin and deoxyhemoglobin in an ex vivo model and measure both arterial and venous blood, the absolute value of a given percentage is not equivalent to the oxygen saturation that would be measured by pulse oximeter. While current values do allow for comparison of data in a given experiment, future work with this technology will focus on calibrating the percent of oxyhemoglobin to a more “clinical” reference, such as oxygen saturation. In addition, improvements in near-infrared technology will allow imaging of the tissue at depths of 1 cm or more, as has been seen with the near-infrared LCTF hyperspectral imager. 18
As the complexity of partial nephrectomy and its application to a broader range of patients continues to increase, it is essential for physicians to continue to search for ways to reliably preserve the remnant portion of the kidney. While hypothermia has been used successfully in open surgery, the lack of an efficient method for inducing hypothermia during laparoscopy dictates that an alternative method for reducing renal insult must be sought, including changes in surgical technique and investigation into new pharmacotherapies. AO occlusion has shown a preliminary benefit to improving postoperative GFR after warm ischemia during laparoscopic partial nephrectomy. While the precise mechanism of renal preservation is unknown, it appears that preservation of renal tissue oxygenation may play a primary role. Further use of HSI, which allows for real-time noninvasive monitoring of renal tissue oxygenation, may allow investigators to determine whether there is a perfusion or oxygenation level at which tissue can be preserved and may allow surgeons to further tailor their technique to improve the postoperative function of the remnant kidney.
Conclusion
HSI represents a novel method for noninvasive measurement of renal tissue oxygenation. As demonstrated in this pilot study, renal tissue oxygenation drops rapidly after occlusion of the renal vasculature and returns to baseline 30 minutes after reperfusion. In the porcine model, purported benefits of AO clamping over AV clamping may be because of differences in renal oxygenation during the first 30 to 35 minutes of renal ischemia.
Footnotes
Acknowledgments
The authors are grateful for the help of Stephanie Shaffer for her expertise in the handling and care of the animals used for this study.
Disclosure Statement
Dr. Zuzak holds a patent on the hyperspectral imaging device. The other authors have no competing financial interests.