
Abstract
Introduction:
Laparoscopic nephroureterectomy (LNU) is a safe, minimally invasive approach for management of upper tract urothelial tumors. Controversy exists over the optimal technique for the distal ureter and bladder cuff (DUBC) excision. We examined the novel technique of using the LigaSure™ bipolar electrosurgical device in laboratory investigations and during clinical LNU to manage the DUBC.
Patients and Methods:
Initial investigations were undertaken in the porcine model. Areas of both normal porcine ureters and bladders, and ex vivo human ureters from radical nephrectomy specimens were sealed with the LigaSure and stained with nicotinamide adenine dinucleotide (NADH) and hematoxylin and eosin to examine the length of treatment effect and the viability of the ablated tissue. Clinically, we performed 22 LNU for proximal urothelial tumors using the LigaSure for the management of the DUBC. Intraoperative cystoscopy assessed cuff resection and bladder leakage. On postoperative day 10, a cystogram was performed.
Results:
In the porcine model, the technique sealed the bladder effectively with a mean burst pressure of 14 mm Hg. Cellular staining revealed no viable urothelial tissue in the seal area and an additional 2 mm outside this area. Eighteen patients had a successful seal/ablation intraoperatively. Cystoscopy revealed cautery artifact and blanching over the former position of the ureteral orifice.
Conclusion:
The LigaSure device ablates and seals urothelial tissue with no viable cells in the clamped and adjacent blanched tissue. Our technique is technically feasible, removes an adequate bladder cuff, typically maintains a closed urinary system, and adheres to sound oncological principles. This procedure could be performed in both laparoscopic and open nephroureterectomy for proximal upper tract transitional cell tumors.
Introduction
A novel method of approaching the DUBC was described by our group in 2005, using the LigaSure bipolar electrosurgical device (Valleylab, Inc., Boulder, CO). 4 Clinical development was unknowingly undertaken simultaneously by our group and Tsvian et al 5 from Israel (Dr. Herrell and Dr. Tsvian personal communication). We hypothesized that the LigaSure technique had the potential advantages of sealing the bladder effectively, destroying an adequate cuff of bladder tissue, maintaining a closed urinary system to avoid urine and tumor cell spillage, and adhering to oncological principles. We describe our initial laboratory experiences using the LigaSure device to assess bladder sealing and urothelial cell viability in a porcine model and human ureteral tissue, as well as our clinical experience using this technique during HAL and pure laparoscopic NU (LNU).
Patients and Methods
Animal model
In an institutionally approved International Animal Care and Use Committee study, 10 adult domestic pigs underwent laparoscopic sealing of the bladder with assessment of seal leakage pressure. A three-way Foley catheter was first inserted into the porcine bladder. Five pigs underwent laparoscopic dissection of the ureters down to the bladder using a standard three-port configuration. The 10-mm LigaSure Atlas was used to clamp, cauterize, and seal (cut) the bladder dome. The bladder was filled with methylene blue–stained saline, and intravesical pressures were recorded via pressure transducer. The pressure at which saline leaked through the ablated dome was recorded as the burst pressure. Two pigs were used as controls. The control animals did not have LigaSure-ablated areas. Instead, the bladder was filled until it ruptured, and the burst pressure was recorded. In the first three animals, there was an attempt to measure pressures by ablating the junction of the ureter with the bladder similar to the NU. However, due to porcine anatomy, an adequate amount of tissue to seal was unable to be obtained. Thus, we altered protocol and sealed the bladder dome as described instead. In addition, the 5- and 10-mm LigaSure Atlas™ were used to seal segments of isolated porcine ureter.
The treated segments were harvested and the animals were sacrificed. Urothelial cell viability of the ablated ureteral segments was assessed by histological evaluation with hematoxylin and eosin (H&E) and nicotinamide adenine dinucleotide (NADH) staining by a dedicated uropathologist. In addition, the length of the peripheral treatment effect area on each side of the LigaSure application was measured. Two sets of controls, untreated ureter and areas that were clamped by the device but not activated, were evaluated. All tissues were processed and stained in a similar fashion.
Human tissue study
Under Institutional Review Board approval, we obtained 10 human radical nephrectomy specimens, and the attached ureteral segment was treated with the LigaSure device in two areas. When the specimen was harvested, the pathologist stained the application and surrounding areas with H&E and NADH to evaluate for viable cells.
Clinical study
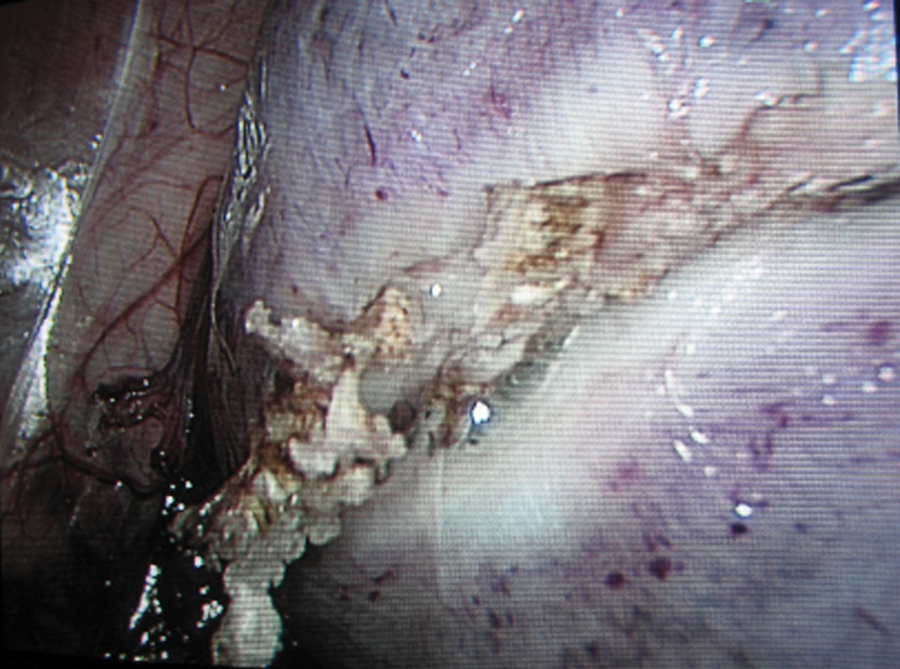
Since 2004, 22 patients with proximal urothelial tumors underwent HAL-NU or LNU with the LigaSure Atlas device used for management of the DUBC by a single surgeon (SDH). Choice of an LNU or HAL-NU was dependent on surgeon preference. Briefly, our technique was similar to previously described reports and included mobilization outside of Gerota's fascia and control of the renal hilum. 6,7 After identification of the ureter at the level of the pelvic brim, an additional 12-mm accessory working port was placed in the lower midline to aid in the ureteral dissection. The ureter was dissected into the pelvis and clipped proximally with two Hemolock™ clips (Weck Systems, Triangle Park, NC) to avoid potential urine spillage. The ureter was traced and mobilized to the detrusor hiatus. The distal ureter was dissected into Waldeyer's sheath posteriorly using hook electrocautery with or without LigaSure (Fig. 1). Gentle upward traction using an atraumatic grasper on the ureter aided in circumferential dissection into the bladder musculature. The dissection continued until the bladder mucosa at the ureterovesical junction was identified. The LigaSure was then used to seal and resect the DUBC en bloc with two sequential applications. Initially, the device was activated distally (caudally) across the elevated bladder mucosa and junction with the distal ureter. Next, the device was reapplied approximately 5- to 10-mm cranial and after sealing the cutting function was activated (Fig. 2). The device provided excellent dissection and hemostasis.
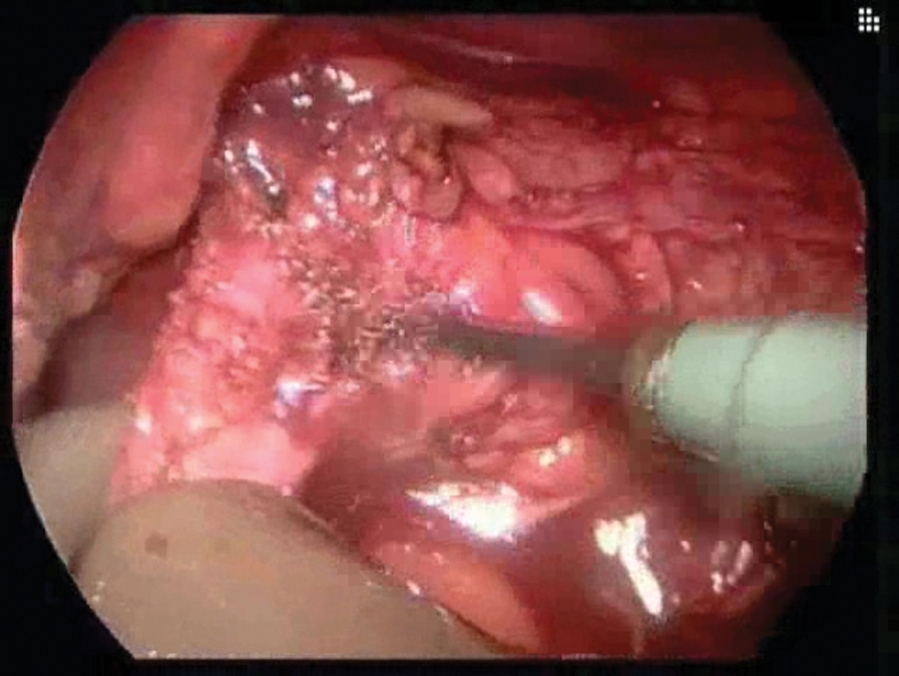
Electrocautery hook is used to dissect ureter into Waldeyer's sheath.
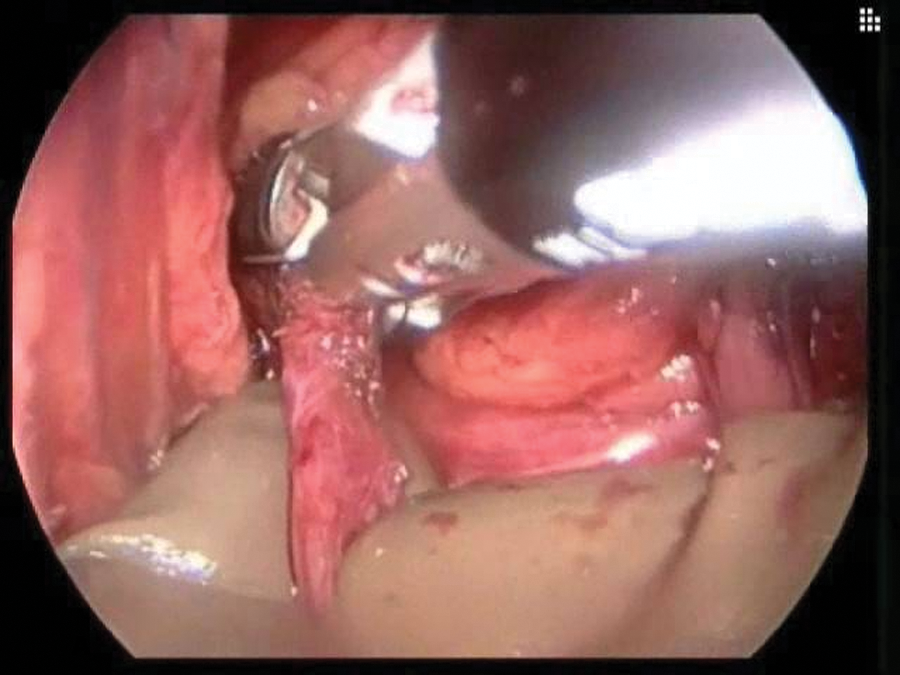
Ten-millimeter LigaSure device positioned across the junction of the distal ureter and bladder cuff. First of two sequential applications.
Flexible cystoscopy was performed intraoperatively to confirm resection of ipsilateral bladder cuff and ureteral orifice. Simultaneous transabdominal laparoscopic inspection of the sealed bladder area allowed identification of any urine leakage from the sealed bladder edge. A Foley catheter was left indwelling for 10–14 days postoperatively, at which point a cystogram was performed to confirm adequate bladder sealing. Follow-up surveillance was performed with cystoscopy and urine cytology every 3 months for the first 2 years in combination with appropriate upper tract imaging. Thereafter, patients were followed with a disease-appropriate surveillance protocol.
Results
Animal model
In the animal model, the urothelial tissue treated by the LigaSure device was without viable cells by both H&E and NADH staining. Twenty sealed/ablated areas of ureteral tissue were evaluated. In addition, the peripheral thermal effect zone represented by a blanched area extending beyond both edges of the application zone was evaluated for each seal. The peripheral thermal effect zone length was 2 mm in each direction from the clamped area for the 10-mm Atlas and 1.4 mm for the 5-mm Atlas (Fig. 3). Both sets of controls of nonclamped, nonablated segments and clamped but nonactivated segments of ureters demonstrated normal viable urothelial tissue. This confirmed that the LigaSure activation and not just the clamping of the tissue causes ablation. These animal studies confirm that the LigaSure device adequately ablates ureteral urothelial tissue.
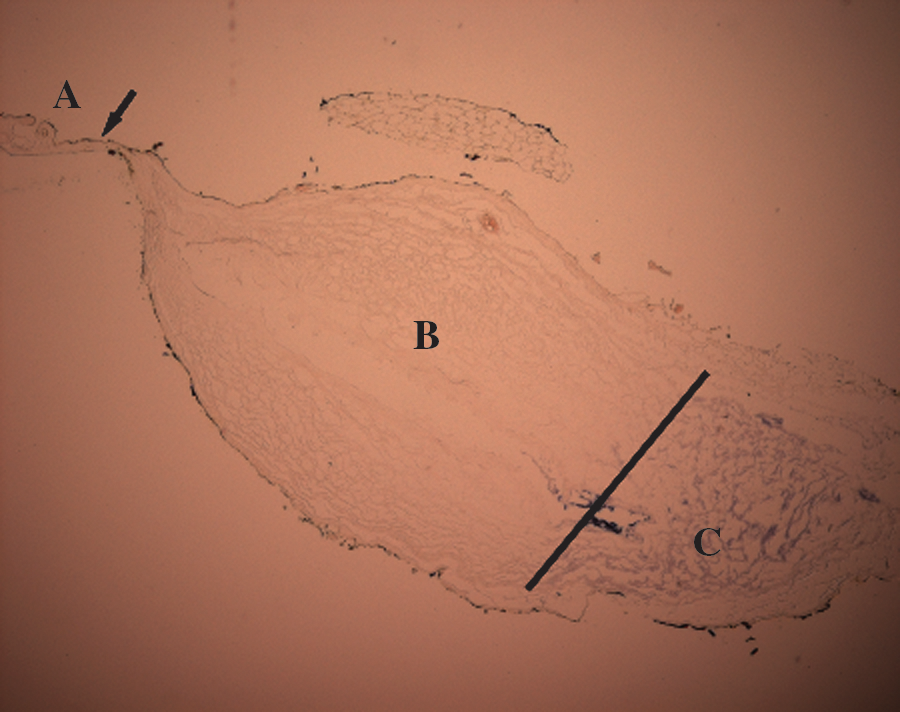
Nicotinamide adenine dinucleotide (NADH) stain: Peripheral thermal ablation zone lateral to the ureteral seal application area, approximately 2 mm of the ureter. Note the lack of staining in the seal/ablated area (A: left of arrow) and the adjacent peripherally thermally ablated tissue (B: left of the black line) and viable tissue (C: right of the black line).
The mean burst pressure was 14 mm Hg (range 10–17 mm Hg). Figure 4 demonstrates the porcine bladder filling without extravasation of fluid in the LigaSure-sealed area. Figure 5 shows the sealed area withstanding pressures well above the resting bladder pressure. The mean nonablated bladder burst pressure was 70 mm Hg. The mean estimated volume of saline instillation required for rupture for the ablated porcine bladder was between 150 and 200 cc, and for the nonablated bladder it was approximately 1100 cc.
The porcine bladder is distended as it is slowly filled, as the area sealed with the LigaSure shows no evidence of extravasation at this point.
The LigaSure-created seal of the bladder dome is close to its rupture point. The seal is able to withstand pressures well above the resting catheterized bladder pressure. The blanched areas adjacent to the sealed and ablated tissue are well demonstrated.
Human model
The human ureteral tissue studies in 20 ureteral seals mirrored the results of the animal model. Both H&E and NADH staining demonstrated no viable urothelial cells.
Clinical study
Twenty-two patients (14 men and 8 women) with suspected proximal urothelial carcinoma underwent HAL-NU or pure laparoscopic-NU. All patients presented with either renal pelvis or proximal ureteral lesions without the concomitant presence of a bladder tumor. There were no open conversions. Mean patient age was 65.6 years (38–84 years) and mean body mass index was 27.7 (20.2–35.8). Mean operative time was 227 minutes (96–300 minutes) and mean estimated blood loss was 158 cc (25–600 cc). Mean hospital length of stay was 3.5 days (1–13 days).
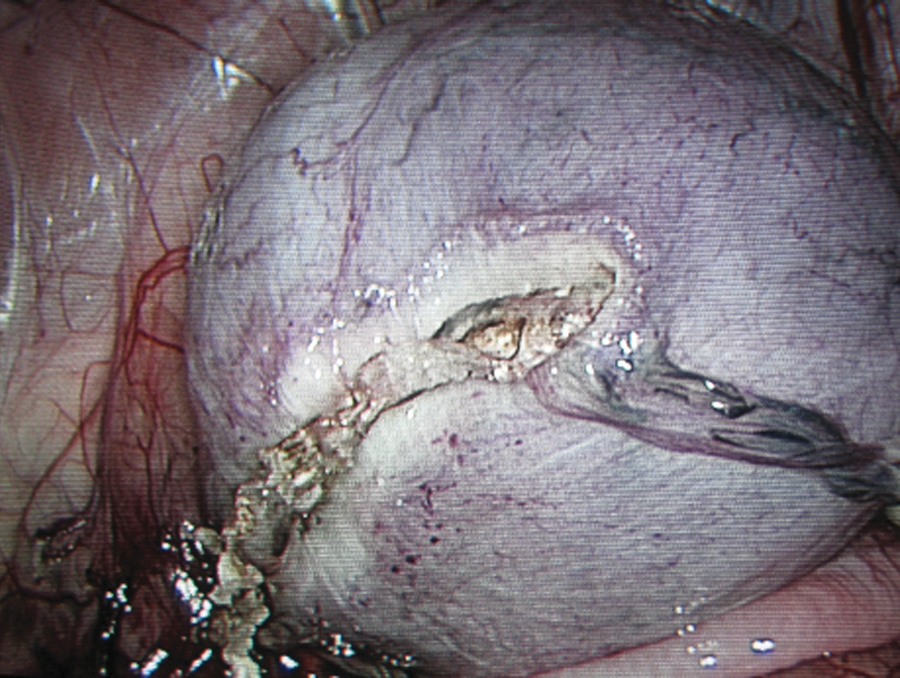
Eighteen patients had a successful seal/ablation. Figure 6 shows the cystoscopic view of the sealed DUBC. Intraoperatively, four patients required reinforcement of the bladder seromuscular layer with 2.0 Vicryl sutures when leakage from the bladder occurred with cystoscopic irrigation. Two of these patients had an indwelling ureteral stent in the affected ureter preoperatively with surrounding reactive periureteral inflammation at the time of HAL-NU. The other two patients were noted to have marked benign prostatic hyperplasia and bladder trabeculation.
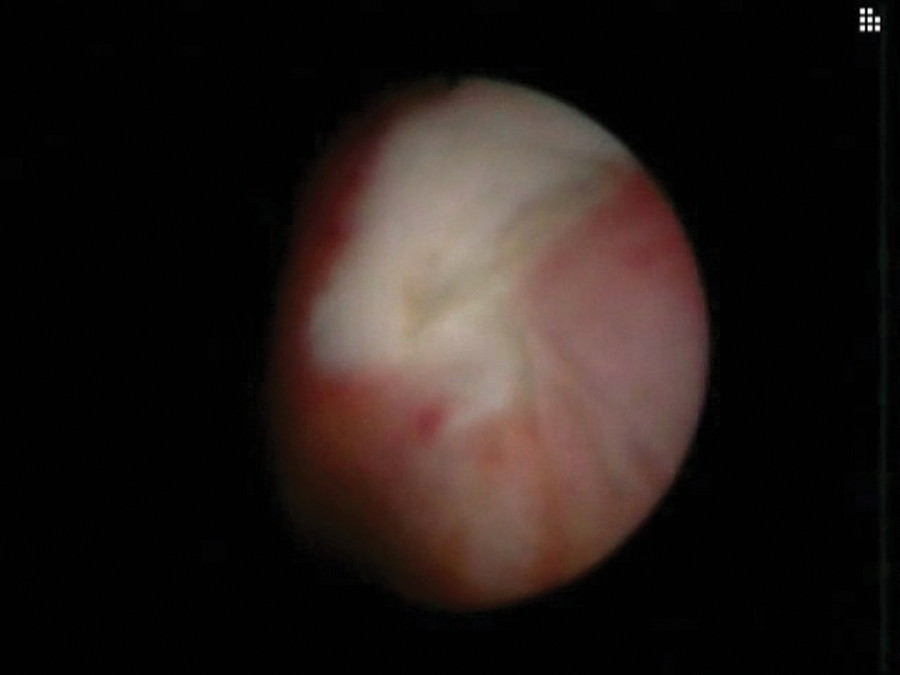
Cystoscopic view of the distal ureter/bladder cuff in a clinical case, demonstrating the LigaSure seal and peripheral treatment effect area of the bladder. The contralateral ureteral orifice was confirmed to be undamaged. Laparoscopic observation revealed no evidence of extravasation from the bladder.
Perioperative complications occurred in four patients. A vena cava injury occurred in one patient, who had dense reactive tissue from previous surgery. The cavotomy was over sewn with 5-0 vascular Prolene with no further sequelae. Another patient had a thermal injury to the small bowel upon entering the abdomen for placement of the hand assist device. This was noted at the time of surgery and was repaired without sequelae. The third patient had extravasation found at cystogram. This resolved with an additional week of catheterization. Additionally, the technique failed to remove the ipsilateral ureteral orifice completely in one patient. This was discovered postoperatively at the time of initial follow-up cystoscopy in the form of an approximately 2-mm distal hood of remaining orifice tissue. The patient subsequently underwent transurethral resection, with negative pathology, and has remained without evidence of disease. There was one death in the cohort. This patient had T4 disease and died from complications of renal failure and metastatic disease 3 months after the operation.
Final histopathology revealed urothelial carcinoma in 19 patients, renal cell carcinoma in 2 patients with central lesions and initial positive urine cytology, and no residual disease T0 in 1 patient with a history of upper tract transitional cell carcinoma treated endoscopically. Of the patients with urothelial carcinoma, 82% presented with renal pelvic tumors, 16.6% with multi-focal lesions, and 5.9% with a ureteral lesion. In patients with transitional-cell carcinoma, pathologic stages were pTa/Tis in 8 patients, pT1 in 4 patients, pT3 in 6 patients, and pT4 in 1 patient. All surgical margins were negative. Median follow-up period was 20 months (range 3–44 months), including cross-sectional computed tomography imaging in all patients. In three patients, superficial bladder recurrences were detected away from the bladder cuff scar. Two patients developed distant metastatic disease. No patient developed a retroperitoneal recurrence.
Discussion
Several series have shown laparoscopic or HAL-NU to have similar oncological outcomes to a number of open NU series. 2,8 Although enthusiasm for HAL-NU and pure LNU and its application have increased, the most controversial and challenging aspect of the operation remains the management of the DUBC. Data clearly demonstrate the importance of distal ureteral excision, as high recurrence rates exist in nonexcised stumps and the surrounding bladder mucosa. 9,10 Adherence to the basic tenets of oncologic surgery mandate the complete en-bloc excision of the kidney, ureter, and bladder cuff. Multiple techniques have been described in the literature as mentioned earlier. No single technique for the DUBC has become standard. 11
The open technique of DUBC excision during LNU parallels that of traditional open surgery. An extravesical or transvesical approach can be employed. An extravesical approach may maintain a closed urinary system; however, care must be taken to avoid inadvertent injury to the contralateral orifice. Alternatively, the anterior cystotomy transvesical approach permits aggressive, careful excision of the bladder cuff, but allows for urine leakage from the bladder during the dissection and possible tumor cell spillage. The transvesical approach remains our preferred technique of distal ureteral excision during LNU when treating patients with locally aggressive distal ureteral lesions.
The transvesical laparoscopic detachment and ligation technique pioneered by Gill et al 12 attempts to mimic the open approach by directly excising the DUBC via two transvesical laparoscopic ports. Briefly, an Endoloop™ (Ethicon, Cincinnati, OH) suture is placed around the ureteral orifice and used for retraction during the dissection of the DUBC. The transurethral resectoscope dissection is carried down through the full thickness of the bladder until extraperitoneal fat is seen, and the ureter is dissected laparoscopically. Suction through the transvesical ports minimizes extravasation of urine and irrigant. This technique permits complete excision of the DUBC under direct vision. Although the Endoloop ligates the ureteral lumen, there remains a risk of urine extravasation with potential tumor seeding. The group reported no differences in local bladder, retroperitoneal, or metastatic recurrences among 43 LNU compared with 35 open procedures. 13 The technique has a difficult learning curve and long operative times. 13
Shalhav and coworkers 14 described a technique of laparoscopic distal ureter stapling combined with cystoscopic unroofing and fulguration of the ureteral orifice and tunnel. The ureter is dissected laparoscopically into the detrusor muscle and stapled with an Endoscopic GIA stapler. Cystoscopically, the exposed ureteral and surrounding bladder mucosa are extensively fulgurated. There is a concern that viable urothelium may be left behind in the staple line. Viable cells have been confirmed between the staple lines in a porcine study. 15 There is an additional risk of staple migration, stone formation, 16 and potential extravasation. To date, there have been no reports of recurrences at the staple line. However, there was an increased incidence of positive surgical margins. 17
The pluck technique is the aggressive transurethral resection of the ureteral orifice to the perivesical fat before the mobilization of the kidney. 18 This method exposes the extravesical space to spillage of irrigant and urine during the procedure and potential tumor seeding with possible development of local tumor recurrences. 19,20 There have been several reports of local and retroperitoneal recurrences utilizing this technique. 19,20 Some advocates of this technique typically do not suture the defect closed; instead, they rely on the bladder to heal itself during a period of extended Foley catheter drainage for 10 to 14 days. 18 Wong and associates 21 recently reported their large series of utilizing the pluck technique without primary bladder closure during HAL-NU, and no cases of pelvic or peritoneal recurrences were noted. 22
Clayman et al 23 initially reported a ureteral intussusception technique for removal of the ureter during open NU without an additional incision. Modifications of the procedure have allowed for a laparoscopic application, but concerns over exposure of bladder and urethral mucosa to the entire intussuscepted ureteral mucosa make this modality less attractive. There is also uncertainty of complete ureteral resection.
The LigaSure device is routinely used in laparoscopic surgery for hemostasis. It is designed to seal vessels up to 7 mm in diameter through a computer-controlled bipolar diathermy system. 24 This system causes automatic discontinuation of energy delivered when the seal cycle is complete. The vessel fusion creates a permanent seal by melting the collagen and elastin in the vessel wall, but does not char the tissue. The LigaSure device effectively seals and cuts tissue, such as blood vessels, lymphatic tissue, and connective tissue, but its effects have not been fully studied on tissue in the urinary tract, such as the ureter and bladder. 25,26
Our hypothesis was that the sealant tissue effect of the device may allow for a simpler method of distal ureteral and cuff management with the potential for several advantages. First, minimal to no suturing is required. Laparoscopic suturing is difficult to perform a watertight closure. Second, this technique ensures destruction of any remaining cuff and/or ureteral urothelium, unlike the use of laparoscopic stapling devices. Further, the technique avoids the acute spilling of potentially tumor-laden urine during the procedure. This theoretically decreases the risk of local recurrence.
Our laboratory studies demonstrate that the device adequately seals and ablates both porcine and human urothelial tissue, without leaving any viable cells behind. We used both NADH stains and H&E stains to determine viability of tissue in this study. While the NADH stains demonstrated consistent and reliable cell death in both the ablated and peripheral treatment effect areas, the H&E stains were less consistent. Although H&E acutely shows some preservation of cell architecture, after some time it shows cell death more consistent with the acute NADH stain results. 27 –30 Therefore, the NADH stains have been generally accepted as the preferential technique to determine cell viability. The described technique (seal/ablation) adds a margin of oncologic safety relative to the endoscopic stapler, which may leave viable tissue. 15 In addition, the computer-controlled system limits the spread of the thermal energy to approximately 2 mm, decreasing the damage to surrounding structures.
The seal of the bladder mucosa ± detrusor created with the LigaSure is, of course, not as strong as normal bladder, as demonstrated in our porcine experiments. This may be especially true in the thin porcine bladder, but is also likely in the human mucosal seal resulting in low bursting pressures. However, it should be acknowledged that there are currently no studies investigating the strength and watertight status of a laparoscopic sutured closure in an LNU. Advocates of the pluck technique depend on the natural healing ability of the catheterized, decompressed bladder, whereas our technique, theoretically, at least provides some superior sealing ability and avoidance of urine spillage. We demonstrated that the seal is strong enough to withstand pressures above the resting pressure of the catheterized bladder. The majority of surgeons decompress the bladder with transurethral catheterization for 7+ days in most described techniques, including formal sutured closure. Thus, we have employed this device and technique for the management of the DUBC during HAL and LNU.
This technique is technically simple, and effective in the majority of cases. The LigaSure device reliably sealed the bladder acutely without urine leakage in 82% (18/22) of patients as demonstrated by intraoperatively filling the bladder and testing the closure. In 18/22 cases, there was no need for laparoscopic suturing in the pelvis, which can be challenging. A cystogram was performed on postoperative day 10 through the Foley catheter to confirm no extravasation; 21/22 patients had the catheter removed on postoperative day 10, with 1 patient demonstrating a small amount of leakage which resolved with an additional 7 days of catheterization. It is feasible that the bladder defect sealed itself by the nature of having a catheter in place for 10 days. However, it should be acknowledged that all patients were adequately closed by either LigaSure technique or suturing demonstrated intraoperatively.
In the cases that resulted in an intraoperative urine leak, all four patients were previously stented or had marked bladder changes consistent with bladder outlet obstruction. We hypothesize that the stents caused periureteral inflammation and mucosal edema preventing adequate tissue approximation, while the obstructive changes caused thinning of the wall or changes in structure at the cellular level, although this remains to be proven. Thus, not all patients represent ideal candidates for this dissection technique. Additionally, patients with bulky distal ureteral tumors are better managed by using the open transvesical approach.
A major advantage of the LNU LigaSure technique is that the specimen can be removed en bloc while maintaining a closed urinary system and avoiding urine spillage, which may contain malignant cells. Our early clinical experience and results with this method are encouraging, although in a small series with short-term follow-up. As with any new technique, additional larger series and potential modifications comparing long-term outcomes are necessary. Although comparative studies of the different techniques would be ideal, the relatively small number of cases even at high volume institutions likely precludes the goal of a randomized controlled study, unless a multi-institutional effort is organized. Given the limitations of the currently employed techniques of managing the DUBC in both open and LNU, this modality may be superior and thus translatable for both open and laparoscopic approaches.
Acknowledgment
The research was supported by an unrestricted educational grant from Valleylab, Inc.
Disclosure Statement
No competing financial interests exist.