
Abstract
Purpose:
The primary objective of this study is to determine if training on the Mimic dV-Trainer (MdVT) simulator results in improved ability on the da Vinci® surgical system (dVSS) using exercises with inanimate objects.
Materials and Methods:
Twelve trainees (MdVT group) and 10 residents and one fellow (dVSS group) were recruited for the study. Each participant in the MdVT group completed one session of five exercises on the dVSS that were scored for timing and accuracy, followed by four training sessions on the MdVT, and concluded with a final session on the dVSS in which the initial exercises were repeated. Improvement on the dVSS exercises was compared with dVSS group who completed four to six training sessions using the same exercises on the dVSS without any simulator training.
Results:
Both groups had similar significant improvements in the Letter Board and String Running exercises for both timing and accuracy. The MdVT group demonstrated significant improvement in the Pattern Cutting and Peg Board times. Only the dVSS group significantly improved in the Knot Tying time and the Peg Board accuracy.
Conclusion:
Training with the MdVT provided similar improvement on five exercises performed on the dVSS when compared with training on the dVSS alone. The use of this simulator in resident and student training may help bridge the gap between the safe acquisition of surgical skills and effective performance during live robot-assisted surgery.
Introduction
Virtual reality (VR) simulation may provide the surgeon with the adequate tools to train in a risk-free environment and may bridge the gap between the safe acquisition of surgical skills and effective performance during live robot-assisted surgery. 6 In a recently published study and another soon to be published study, Sethi and associates 7,8 demonstrated initial face, content, and construct validity of the Mimic dV-Trainer (MdVT). We present a prospective study in which we compare two groups of novices. One group trained with inanimate objects on the da Vinci® (Intuitive Surgical, Sunnyvale CA) Surgical System (dVSS) and the other group trained with the MdVT. The goal of this study was to determine if training on the MdVT provides the acquisition of skills on the dVSS.
Materials and Methods
The MdVT was developed by Mimic Technologies, Inc. (Seattle, WA) and was commissioned by the Departments of Urology at Indiana University and Mechanical Engineering at Purdue University. The simulator interface includes foot pedals, side pods, endowrists, and a high definition stereoscopic display that functions similarly to the console components found in the dVSS (Fig. 1). The MdVT simulation software allows the user to interface with a stereoscopic virtual environment that includes inanimate objects and virtual anatomy. Immediate performance feedback is available for the user or investigator after the completion of a virtual exercise (Fig. 2). 7,8

Console interface.
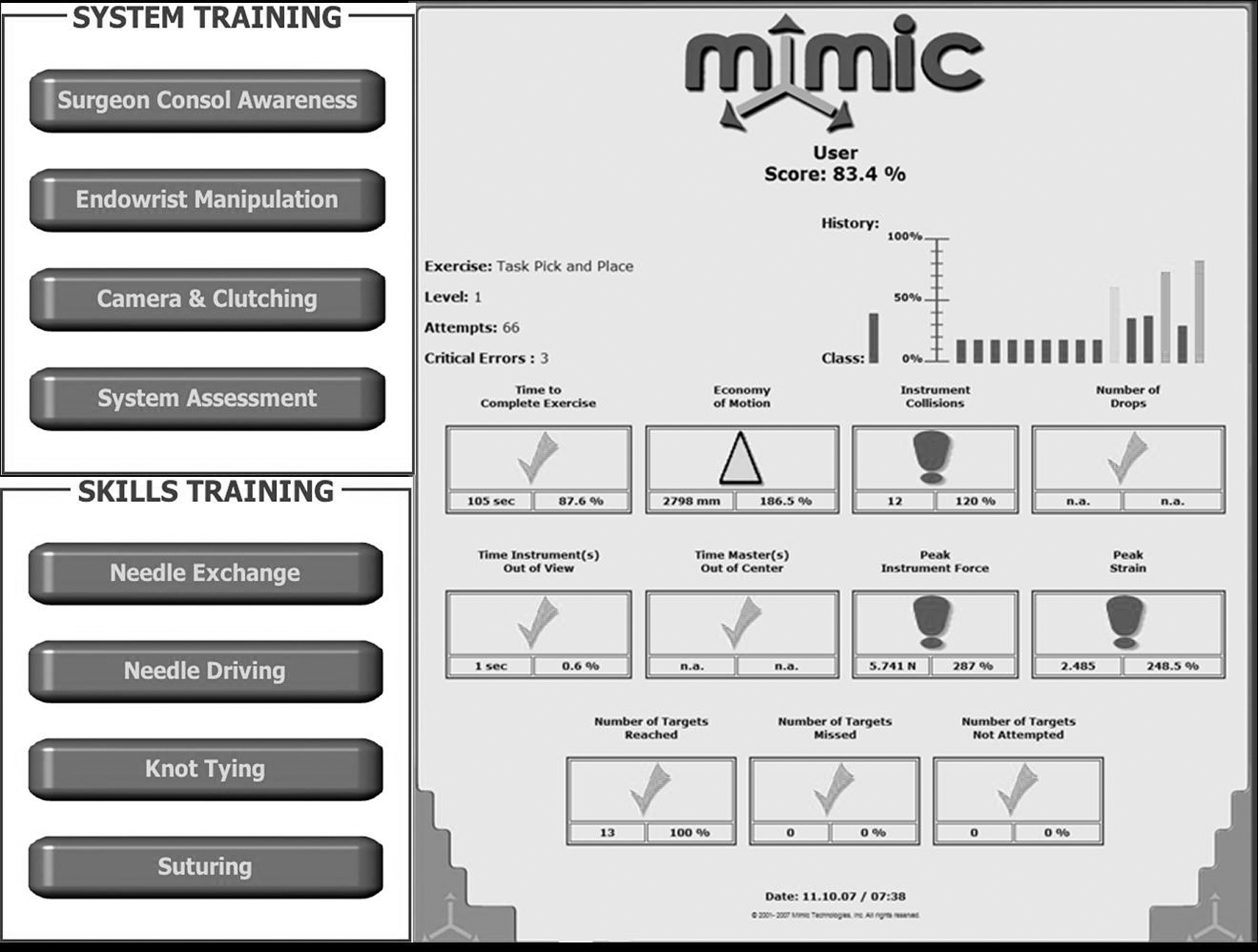
Performance metrics.
At our institution, we require the urology residents to practice five standardized training exercises on the dVSS using inanimate objects before working with patients in live surgery. These exercises were modified from Scott and colleagues 9 and are based on our laparoscopic pelvic trainer curriculum. The five exercises include 1) Peg Board—pegs are picked up from a peg board with the left hand, transferred to the right hand, and placed in a marked hole; 2) Pattern Cutting—Potts scissors are used to cut out a circle pattern on a Kendall Telfa® pad that is secured within a wooden frame; 3) Letter Board—wooden letters and numbers are placed on a board with the representative shadows of the numbers and letters using needle holders or graspers; 4) String Running—umbilical tape is grasped at marked sites using graspers and alternating hands; 5) Intracorporeal Knot Tying—two edges of a Penrose drain are approximated by using a surgeon's knot for the first throw followed by three additional single throws. The residents are required to complete six training sessions that are scheduled on the weekends. Each resident is allotted a 1 hour time slot in which to practice the five exercises. A surgical technician oversees the resident use of the robot and scores the times and accuracy of the residents on each exercise. We have had 11 residents complete four to six training sessions using the exercises described above on the dVSS.
We recruited a group of 12 participants consisting of medical students and interns with no previous robotic experience and asked them to complete a series of exercises using a combination of the MdVT simulator and the dVSS. Each participant in the MdVT group completed an initial training session on the dVSS consisting of the five standardized exercises (Letter Board, Peg Board, String Running, Pattern Cutting, Intracorporeal Knot Tying). After the initial training session on the dVSS, the participants completed four training sessions consisting of four exercises on the MdVT. These exercises were designed to mimic many of the same skills required on the dVSS exercises. The MdVT exercises consisted of 1) Letter Board—letters and numerals are placed on the perimeter of a 3 × 3 letter board and placed onto their corresponding positions; 2) Pick and Place—rings are picked up by a designated grasper and placed on alternating cones; 3) Ring Walk—a ring is guided along a virtual ureter; 4) Clutching Cavity—the graspers are moved across long distances in a virtual abdomen necessitating use of the clutch and camera pedals. Exercises on the MdVT were scored for timing, economy of motion, instrument collision, time instruments were out of view, peak instrument force, and the number of targets reached and missed. After completing the MdVT training exercises, the participants returned to the dVSS and were retested for timing and accuracy on the initial five exercises described by Scott and coworkers. 9
The introductory and final results for timing and accuracy were compared for individual exercises on the VR simulator and on the dVSS within the dVSS and MdVT groups. The baseline scores for timing and accuracy and the level of improvement for individual exercises were compared between the dVSS and the MdVT groups. The data were analyzed with paired t tests using the R statistical software. 10
Results
Twelve participants in the MdVT group completed an initial training session on the dVSS, four training sessions on the MdVT, and a final training session on the dVSS. One participant was unable to complete the final training session on the dVSS because of scheduling conflicts. Eleven participants in the dVSS group completed a minimum of four training sessions on the dVSS alone. The MdVT group consisted of eight medical students, 3 urology interns, and 1 urology fellow with no previous robotic experience. The dVSS group consisted of 10 urology residents and 1 urology fellow with minimal robotic experience before starting the sessions. The dVSS group was able to participate in live robotic and laparoscopic surgery as a part of their clinical duties in between training sessions. The MdVT group had virtually no participation in live robotic or laparoscopic surgery in between training sessions.
The mean baseline times on the dVSS were worse in the MdVT group on the Peg Board and Pattern Cutting exercises (P = 0.04 and P = 0.006, respectively). There were no significant differences in baseline times and accuracy observed between the two groups in the other standardized exercises on the dVSS. Table 1 shows the results of the five standardized exercises for both groups. Both groups demonstrated similar improvements in the Letter Board and String Running exercises for both timing and accuracy. The dVSS group showed statistically significant improvement in the Intracorporeal Knot Tying time and had increased accuracy placing the pegs in the designated holes on the Peg Board exercise. Only the MdVT group demonstrated statistically significant improvement in the Peg Board and Pattern Cutting times. While the MdVT group had improved mean times on the final Intracorporeal Knot Tying exercise, these times did not reach statistical significance.
dVSS = da Vinci Surgical System; MdVT = Mimic dV-Trainer; (s) denotes plural.
Table 2 shows the results of the VR simulator for the MdVT group. During the sessions on the MdVT, participants had significantly improved times on the Letter Board, Pick and Place, and Clutching Cavity exercises. The desired targets were hit with increasing frequency on the Ring Walk, Pick and Place, and Clutching Cavity activities. There was significantly improved economy of motion on the Letter Board and the Pick and Place exercises. Finally, there was a decreased peak instrument force on the Clutching Cavity exercise and decreased number of instrument collisions on the Pick and Place.
MdVT = Mimic dV-Trainer; N = Newton.
The differences in improvement between the introductory and final dVSS training exercises were compared between the two groups. The MdVT group had significantly greater improvement in the Peg Board times and Pattern Cutting times (P = 0.008 and P = 0.02, respectively). There were no statistically significant differences between the two groups in their levels of improvement for the remaining dVSS exercises (Table 3).
dVSS = da Vinci Surgical System; MdVT = Mimic dV-Trainer.
Discussion
As interest in robot-assisted surgery continues to expand, there remains a need to provide young surgeons with proficiency in robotic technology. The development of valid simulators that allow surgeons-in-training to master minimally invasive techniques in a controlled, pressure-free environment will assist in the safe acquisition of skills and help overcome the steep learning curve associated with new technologies. 11 –17 VR robotic simulators have the potential to address the training needs of inexperienced surgeons.
The MdVT performance metrics include time to completion of the exercise, number of instrument collisions, time instruments out of view, peak instrument force, peak instrument strain, economy of motion, number of targets reached, and number of targets missed. Although we did not share the results of the performance metrics with the participants in between MdVT exercises, these performance metrics may be used to provide immediate feedback to the participant and assist the surgeon-in-training in the rapid acquisition of skills on the dVSS.
The MdVT group consisted mostly of medical students and their exposure to surgery was minimal whereas the dVSS group consisted almost exclusively of urology residents with a broader surgical experience at baseline. The dVSS group had the additional advantage of day-to-day surgical experiences that included clinical coverage of live robot-assisted surgery and laparoscopic surgery in between training sessions. These differences explain the statistically significant difference in baseline timing scores between both groups on the Peg Board and the Pattern Cutting exercises.
Both groups exhibited similar improvements in performance times and accuracy between the initial training session and the final training session on the dVSS. The MdVT group demonstrated statistically significant improvement in all of the exercises except for the String Running and Intracorporeal Knot Tying. The mean times for both of these exercises in the final dVSS session were improved, albeit not statistically significant in this small sample size. At this point, suturing exercises are not fully developed on the MdVT and were not used during this study. The lack of an adequate suturing exercise and the surgical inexperience of the MdVT group may be responsible for their lack of improvement demonstrated on the Intracorporeal Knot Tying exercise. In the Peg Board and Pattern Cutting exercises, the MdVT group made significant improvements in the mean times whereas the dVSS group did not. These were the same exercises in which the MdVT group scored significantly worse at baseline compared with the dVSS group.
On the VR simulator, the Letter Board and the Pick and Place exercises are either identical or very similar to Letter Board and Peg Board exercises on the dVSS. Training that used both of these exercises clearly translated into improved performance on the final dVSS session. The Clutching Cavity exercise is designed to teach the participants how to use the camera and clutch foot pedals. Improved familiarity with the foot pedals results in decreased peak instrument force and decreased instrument collisions. Significant improvements in peak instrument force were demonstrated on the MdVT in the Clutching Cavity exercise. Improved familiarity and efficiency with the foot pedals would theoretically translate into improved timing on the five standardized dVSS exercises. Unfortunately, this study did not have a system in place to measure improved use of the foot pedals on the dVSS.
There was an overall trend toward improvement in many performance metrics on the VR simulator despite a lack of statistical significance. A larger number of participants and immediate feedback after completion of a VR exercise may have demonstrated statistical significance in more of the performance metrics. The VR simulator provided familiarity and comfort with the console controls that translated into a dramatic improvement on the dVSS for the MdVT group.
There are several limitations to this study. The differences in baseline surgical experiences and the responsibilities of day-to-day clinical duties gave the dVSS group a performance advantage compared with the MdVT group. Despite the additional advantages of the dVSS group, the MdVT group performed exceedingly well. This study can also be criticized for the small sample size in both cohorts.
Some of the software used for this study was custom developed for us to duplicate our robotics skills curriculum. The MdVT software development is working to introduce exercise sets that can be easily created by the user to suit his/her specific surgical specialty or surgery. Advanced task training for individual specialties with geometric exercises similar to anatomic structures (ie. urethrovesical anastomosis) and suturing suites that teach various suturing scenarios (ie. bleeding management) may be available in the future.
Mimic is continuing to make improvements on components of the MdVT that remain somewhat fragile. The grippers and gimbals require robust durability before the MdVT will be available for commercial distribution. The rate of novices adopting robot-assisted surgery into their practice remains low after completion of the training courses provided by Intuitive Surgical. The MdVT could play a role in improving retention rates of robotic surgical skills among low volume robotic surgeons. The use of the MdVT in the training of novices and future software developments in VR simulation may help bridge the gap between the safe acquisition of surgical skills and effective performance during live robot-assisted surgery.
Conclusions
Training on the MdVT improved performance on the dVSS when exercises with inanimate objects were used.
Footnotes
Disclosure Statement
No competing financial interests exist.