
Abstract
Introduction:
The daVinci Robot system has been widely lauded for its improved ergonomic characteristics when compared with the pure laparoscopic technique. Our goal in this study was to assess for the existence of guidelines to maximize the ergonomic benefits of the daVinci system. We also compared the surgeon's console with the recommendations of similar workstations.
Methods:
A literature review of seated ergonomics was performed to identify recommendations for work areas similar to the robotic system, where prolong seating is necessary. An upper body biomechanics and ergonomic expert was consulted to evaluate the daVinci system and aid in the formation of ergonomic positioning guidelines. Link-length proportions were used to evaluate size constraints of potential robot operators.
Results:
No published guidelines exist for proper positioning using the daVinci surgeon console. There are, however, several Occupational Safety and Health Administration workstation guidelines as well as microscope ergonomic guidelines. The use of link-length proportions showed that the surgeon console allows a comfortable posture for individuals with height between 64 and 73 inches. Review of the microscope ergonomics literature indicates that a neutral vertical seating position has been associated with decreased strain and musculoskeletal disorders.
Conclusions:
The body mechanics of the daVinci robot system best mimics that of microscopy. Future surgeon console modifications could emulate those reported in the microscope ergonomic literature, where a neutral vertical position has been recommended. This may help avoid potential musculoskeletal disorders similar to those previously seen with microscopy usage. Guidelines are suggested to optimize the surgeon's console position.
Introduction
The U.S. Department of Labor's Occupational Safety and Health Administration (OSHA) has extensive guidelines for good working positions at workstations. 8 Even more applicable, perhaps, is the body of work available on the ergonomics of microscopy. Commercial cytotechnologists frequently spend 6 to 8 hours a day looking into their microscope, with positions and physical movements that directly mimic the required upper body movements performed during robotic surgery. Good fit has been found critical with prolonged use of the microscope. 9 In a study with an average experience of 17 years, the subjects were found to have an increased risk of kyphosis attributed to a combination of chronically tense pectoral muscles, and bending over the scope for years. 10 When the risk of diagnosed occupational neck problems among various occupational groups was evaluated, microscopists were found to have a rate of 66%. 11,12 Another study found that 70.5% of surveyed cytotechnologists reported neck, shoulder, or upper back symptoms. 13 If we are to consider the microscope model as a plausible surrogate for robotic surgery ergonomics, the long-term fit between the robot and the operator becomes very important. In this study, we assess the ergonomic characteristics of the surgeon's console, and compared them with those of microscopy.
Materials and Methods
A thorough literature search was performed using PubMed and Medline searching keywords robotics, laparoscopy, microscopy, ergonomics, biomechanics, workstations, and daVinci. An upper body biomechanics and ergonomics team was consulted for evaluation of the workstation. The consultant team was allowed to watch several mock and actual operations by individuals of different heights, and was allowed to fully experiment with the workings of the daVinci system. The consult team was also able to discuss the system with surgeons experienced with the daVinci system.
To evaluate the ergonomics of the daVinci system, measurements were collected to assess the critical physical dimensions of the system. Although the preferred postures that individual surgeons utilize may vary, ideal posture was selected and assumed to represent most users. As shown in Figure 1, it was assumed that the user sits in a chair with his/her thighs parallel to the floor and the lower legs slightly outstretched to reach the foot-operated controls. Based on observation and experience with the system, it was assumed that an angle of 20° would be reasonable for the lower leg angle. For back flexion, the angle θ was treated as a variable and evaluated.
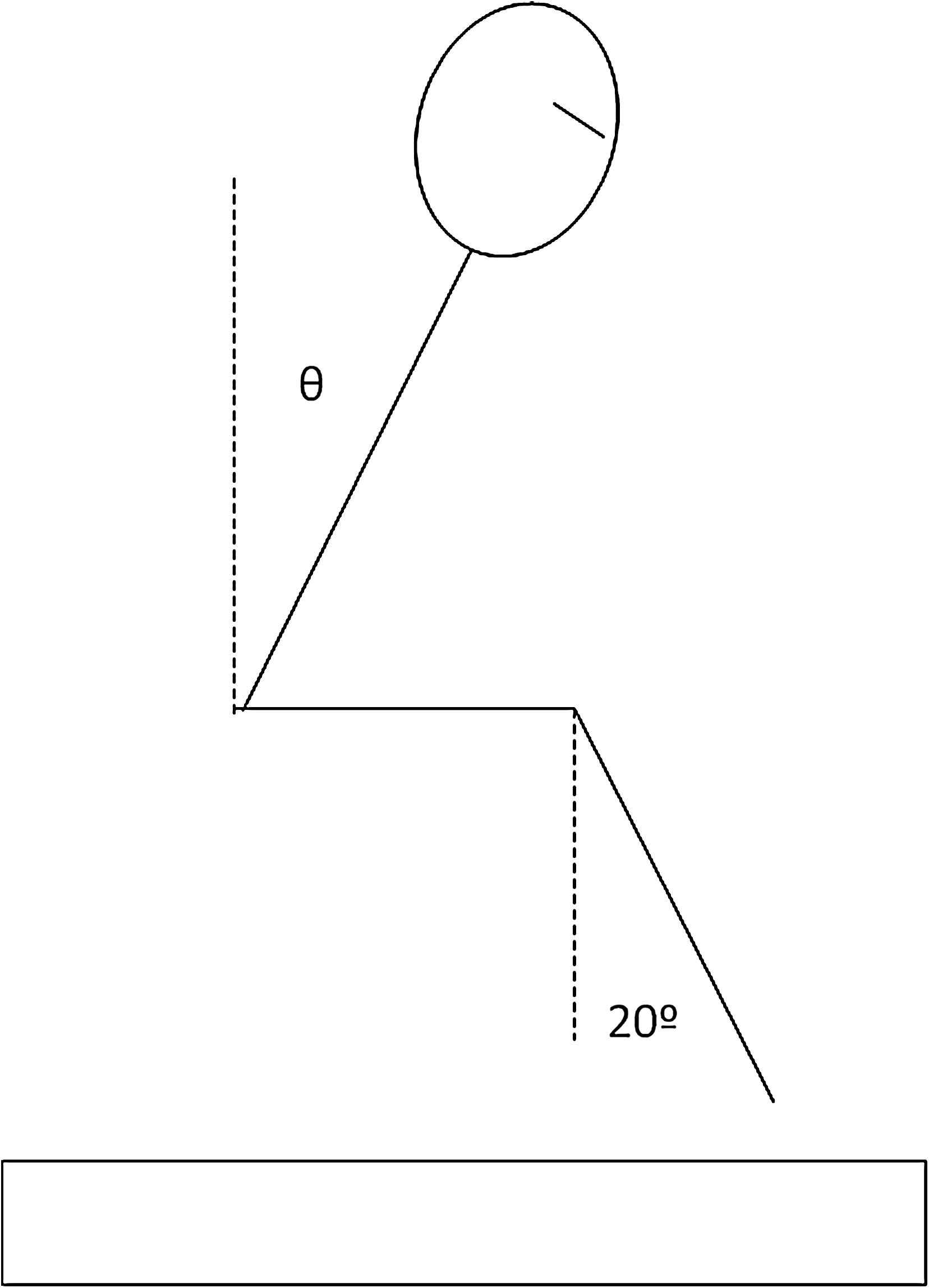
Assumed postures utilized in using the daVinci surgical system.
Based on the postures illustrated in Figure 1, and the link-length proportions identified by Drillis and Contini, 14 the vertical position of the user's eyes was determined for a wide variety of user statures. From Figure 1, the vertical positions of the eyes are simply a function of the angles of the back and leg. Since the user must place his/her foot on the foot pedals, it was assumed that the thickness of the controls was approximately 2 inches and that the chair would be positioned relative to the top of the foot controls, rather than the floor. As an example, for an individual 5′8″ in height, a leg angle of 20°, and a back angle of 15°, the eye location would be as follows: (Length of lower leg) × cosine(20°) + (Length of torso to eyes) × cosine(15°) + 2″.
Final recommendations were then compiled taking OSHA standards, the literature search, the above calculations, and expert consultant opinion into consideration.
Results
Evaluation of daVinci ergonomics
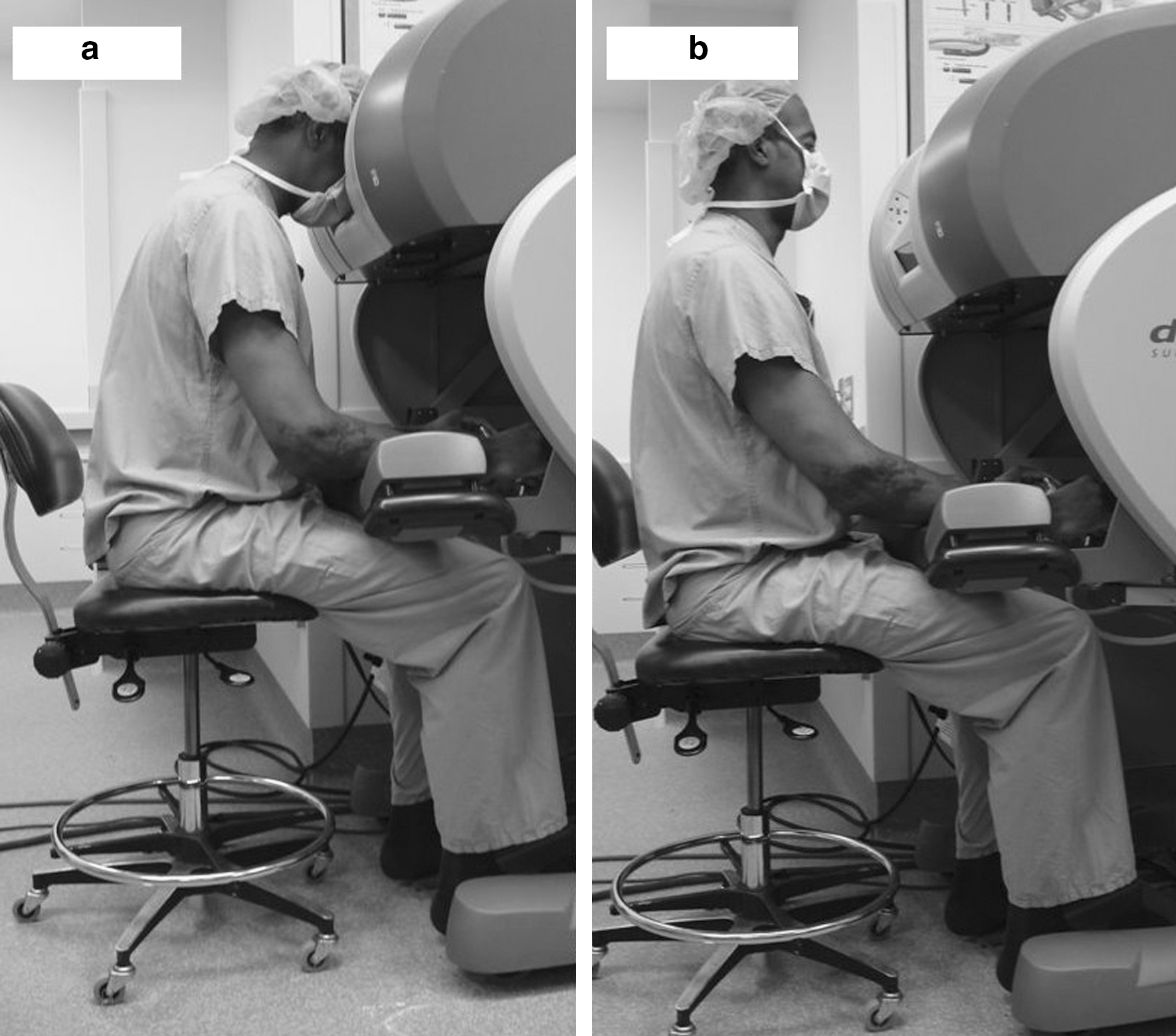
The eyepieces on the console were found to be adjustable between approximately 45 and 52 inches off the ground, with the pedal platform raised 2 inches above this. All subsequent stature analysis utilizes these figures. Assuming only a slight amount of back flexion (15°), the vertical location of the eyes for an individual 5′4″ in stature or shorter will fall below the lowest height adjustment of the eye piece (Fig. 2). In this situation, the operator must raise the seat and over-straighten their neck and spine to see into the eyepiece. In doing so, they will have difficulty reaching the pedals (Fig. 3a, b). As the angle of back flexion increases to 30°, individuals as tall as 5′7″ will be challenged to reach the eye piece. Similarly, individuals over 6′1″ will have to bend over greater than 30° for viewing (Fig. 4a, b).

Vertical eye position as a function of user stature. Each line represents a different level of back flexion angle.

(
(
Suggested guidelines to optimize the use of the surgeon's console
Surgeon's chair recommendations
Based on OSHA and formal prior microscopist work station evaluations, the chair should be on lockable castors for ease of mobility near the console workstation. The chair should have a readily adjustable height, lumbar support, and a tiltable seat angle, though generally parallel to the floor. The seat depth should be adjustable as well, to aid in utilization of the lumbar support.
Proper positioning
Chair and console height should be adjusted so that the view screens are at a comfortable position for viewing when the feet are resting on the ground in front of the pedals with knees at a 90° angle or greater. At this height, the upper arms are perpendicular to the floor with the elbows forming a 90° angle, and the forearms resting on the armrest (neutral position). Elbows should remain tucked close to the body and not flared. The ideal position should allow for the feet to easily reach the pedals, while the forearms can rest comfortably on the armrest, and allow observation through the view screens without undue arching and straightening of the back or neck to gain additional height or excessive bending of the neck and upper back to look downward. The position should be attained at the onset of the case, with periodic revaluation if discomfort occurs later. Although a headrest is available, avoid firmly pressing into the headrest, as this can result in undue forehead pain and neck strain.
The most frequent cause of malpositioning occurs when the arms are brought out of neutral position. When the hands are located toward the far edge of the work envelope, the user tends to raiser his/her arms off of the arm rest. This can be alleviated by frequent clutching to bring the arms back into a neutral position.
When symptoms suggesting fatigue presents, implement intermittent stretching during scope changes, instrument changes, or suture swaps. Reconsider chair and console height adjustments to reduce excessive back and neck arching or bending.
Discussion
The first known discussion of the ergonomics of the microscope occurred in the 1830s when Sir David Brewster noted in his Treatise on Optics that, “The best position for microscopic observations is when the observer is lying horizontally on his back. … The worst of all positions is that in which we look downward vertically.” Despite this early treatise, the ergonomics of microscope design went relatively ignored until the mid to late 1990s. By this time, several reports showed large numbers of work-related musculoskeletal disorders for workers sitting at their microscopes 6 to 8 hours a day for several years. About 70.5% to 75% of experienced microscopists have been found to have neck, shoulder, or upper back symptoms, 10,13 far exceeding that of the general population. When broken down into actual problem areas, 50% to 57% experience neck problems, 66% to 75% shoulder, 49% to 66% lower back, and 39% experience upper back problems. 9,10
As a result of these known musculoskeletal disorders, several intervention studies sought to determine the greatest static forces at play. Around the years 2000 to 2003, these studies resulted in modifications to microscope design that are reflected in the current daVinci system, such as a comfortable headrest, adjustable ocular height, and armrests. 10,15 One design that was not incorporated into the daVinci system, however, was a change in the ocular angle. As alluded to by Sir David Brewster in 1830 in his Treatise on Optics, looking downward is the worst angle for strain of the neck and shoulders. This age-old wisdom has been verified by modern studies by Chaffin and Anderson 16 and Putz-Anderson, 17 who both independently concluded that even slight head declinations such as 30° from vertical for the head and back can produce significant static muscle contraction, fatigue, and pain. These two studies caused microscope design to alter dramatically, resulting in a new generation of ergonomic microscopes with a changed ocular angle such that the modern microscopes can be viewed from an upright seated position looking straight forward. These recommendations were then verified with electromyographic (studies that revealed significantly lower muscle activity on both sides of the neck, deltoids, and trapezius muscles). 10 Moreover, it was found that the old style, downward looking angle exceeded the upper limit of Jonsson (must not exceed) for static and medium loads in the neck. 10 The results of surveys using the new microscope design revealed that participants were significantly more comfortable in the neck and shoulder regions (p < 0.05), and experienced less mid back discomfort. 15
When we consider that robotic surgery has been found to be more comfortable than laparoscopic in every aspect but discomfort in the neck and trunk, 7 these findings on the viewing angles of microscopes become even more enlightening. This suggests that future evolution of the daVinci surgeon console may benefit from a directly forward looking design to reduce neck, shoulder, and upper back strain. The results in the daVinci console are likely to be even more profound than the findings of microscopy, since a microscopist's head is forced to remain relatively rigid to maintain the view of the small lenses on the microscope. This forced rigidity is one of the proposed causes of neck strain. With the daVinci system, however, large view screens for each eye allow for small movements both horizontally and vertically while maintaining appropriate vision, and hence likely to reduce neck strain.
To further minimize static loading of the shoulders and upper back, it is important that the arms remain at least partially resting on the arm rest near neutral position. When working with the arms outstretched and unsupported for prolonged periods, the static loading of the deltoid and trapezius muscles can be significant and may lead to discomfort and soreness in those affected regions. This can be accomplished by forcing oneself to constantly clutch the system to maintain the forearms on the armrests.
Although the daVinci system fits most surgeons well, its range of adjustment is inadequate for men with height below the 5th and above the 95th percentile (Fig. 2), and ever more inadequate for short-statured women. In order for a small-statured individual to see through the eye pieces, he or she has to raise the chair to reach the eye pieces. In this setting, they experience difficulty reaching the foot controls (Fig. 3a, b). As such, it is likely that with the chair raised, the user will need to sit forward toward the edge of the seat with their upper leg outstretched to reach the foot controls. Therefore, it is advisable for individuals approaching 64 inches or less to consider placing the pedals on the docking rail used for transport instead of the floor. If this is still insufficient, consider an additional small platform to raise the foot controls so that the user is able to position the height of the chair to enable easy access to the eye piece and still reach the pedals. It should be noted that whatever method is used to raise the foot pedals, these needs to be stable and fully supported to avoid the possibility of the foot controls slipping while the system is in use.
Although most of the recommendations put forth in the results under Surgeon's chair recommendations and Proper positioning sections are for the most part common sense, following these is essential to maintain a comfortable operative experience.
Conclusion
Utilization of the suggested guidelines and potential modifications to the daVinci system has the potential to reduce static muscular skeletal strain during operating, resulting in a more comfortable operative experience with decreased long-term sequelae. A comfortable surgeon is a less fatigued surgeon with a better outcome for all involved.
Footnotes
Disclosure Statement
No competing financial interests exist.