
Abstract
Objectives:
Radiofrequency ablation (RFA)–assisted laparoscopic partial nephrectomy (LPN) may allow for improved hemostasis without need for renal hilar vessel clamping and elimination of warm ischemia to the kidney. We compare outcomes in patients undergoing radiofrequency ablation-assisted robotic clampless partial nephrectomy (RF-RCPN) and LPN.
Methods:
Thirty-six patients and 42 patients underwent LPN and RF-RCPN, respectively. In the RF-RCPN group, the Habib 4× RFA device was used to coagulate a margin of normal parenchyma around the renal mass to allow excision of the mass within a bloodless plane. Unlike in the LPN group, renal hilar vascular occlusion was not performed in the RF-RCPN group.
Results:
Tumors treated in the RF-RCPN group tended to be larger (2.8 vs. 2.0 cm) and more often endophytic (52.6% vs. 16.1%). Collecting system reconstruction occurred more often in the RF-RCPN group (78.6% vs. 30.6%). Operative duration was longer in the RF-RCPN group (373 vs. 250 minutes), but this included time for cystoscopy, ureteral stenting, and repositioning of the patient. Blood loss, transfusion rates, renal function, and complication rates did not differ between the two groups. No patients required renal hilar vessel clamping or nephrectomy to control bleeding in the RF-RCPN group.
Conclusions:
The use of RFA-assistance during robotic partial nephrectomy allows excision of renal tumors without hilar vascular clamping, thus eliminating renal warm ischemia. Larger and more centrally located tumors were excised with RF-RCPN. No differences in blood loss, complication rate, postoperative bleeding, renal function, or recurrence rate were noted compared with LPN.
Introduction
Patients and Methods
From October 2002 to May 2007, 36 consecutive patients underwent LPN with renal hilar vessel clamping and cold sharp excision of renal tumors. Between June 2007 to February 2009, 42 consecutive patients underwent RF-RCPN. We did not discriminate based on tumor size or location to which patients we offered RF-RCPN. Starting from June 2007, only the RF-RCPN technique was utilized for partial nephrectomy in this study. All patients had surgery performed by one of three surgeons (R.B.N., N.D.S., or K.T.P.). Patient information was collected prospectively in a centralized database with Institutional Review Board approval. Patient characteristics and perioperative outcomes were compared. Proportion of endophytic tumors were defined as tumors with >50% of tumor volume within normal kidney outline or tumor impinging on the collecting system seen on preoperative imaging. 18
t-Test and chi-squared test were performed with Microsoft Excel 2007 (Redmond, WA). Multivariate analysis (linear or logistic regression models) was done using SAS 9.2 (SAS Institute, Cary, NC). p-Values <0.05 were considered statistically significant.
Our RF-RCPN technique has been modified since its initial description. 26 We now place a 7F externalized ureteral stent instead of a 5F externalized catheter for retrograde injection of methylene blue intraoperatively and to improve urinary drainage after repair. Ports are placed in a “W” configuration with patients in lateral decubitus position (Fig. 1). Renal hilar vessels are not clamped after exposure with a transperitoneal approach. The tumor is localized with laparoscopic ultrasound and then exposed. The da Vinci robot (Intuitive Surgical, Sunnyvale, CA) is then docked. A margin of coagulated normal parenchyma is made around the tumor with a bipolar RFA laparoscopic device, the Habib 4 × (AngioDynamics, Queensbury, NY) coupled to a Rita 1500 × (software version 8.41) generator to create the coagulated plane around renal tumors before excision (Fig. 2). All bleeding encountered during the coagulation process is controlled by repuncturing and treating the affected area. The tumor is resected with robotic scissors in the coagulated margin. Collecting system violations are closed with running absorbable suture. We then place Surgicel bolsters (Ethicon Endo-Surgery, Cincinnati, OH) and FloSeal™ (Fusion Medical Technologies, Mountain View, CA) in the tumor bed and perform the sliding-clip renorrhaphy as described by Benway. 27 Once frozen section tumor bed biopsies and margins are confirmed negative for tumor, a closed suction drain is placed before closure.
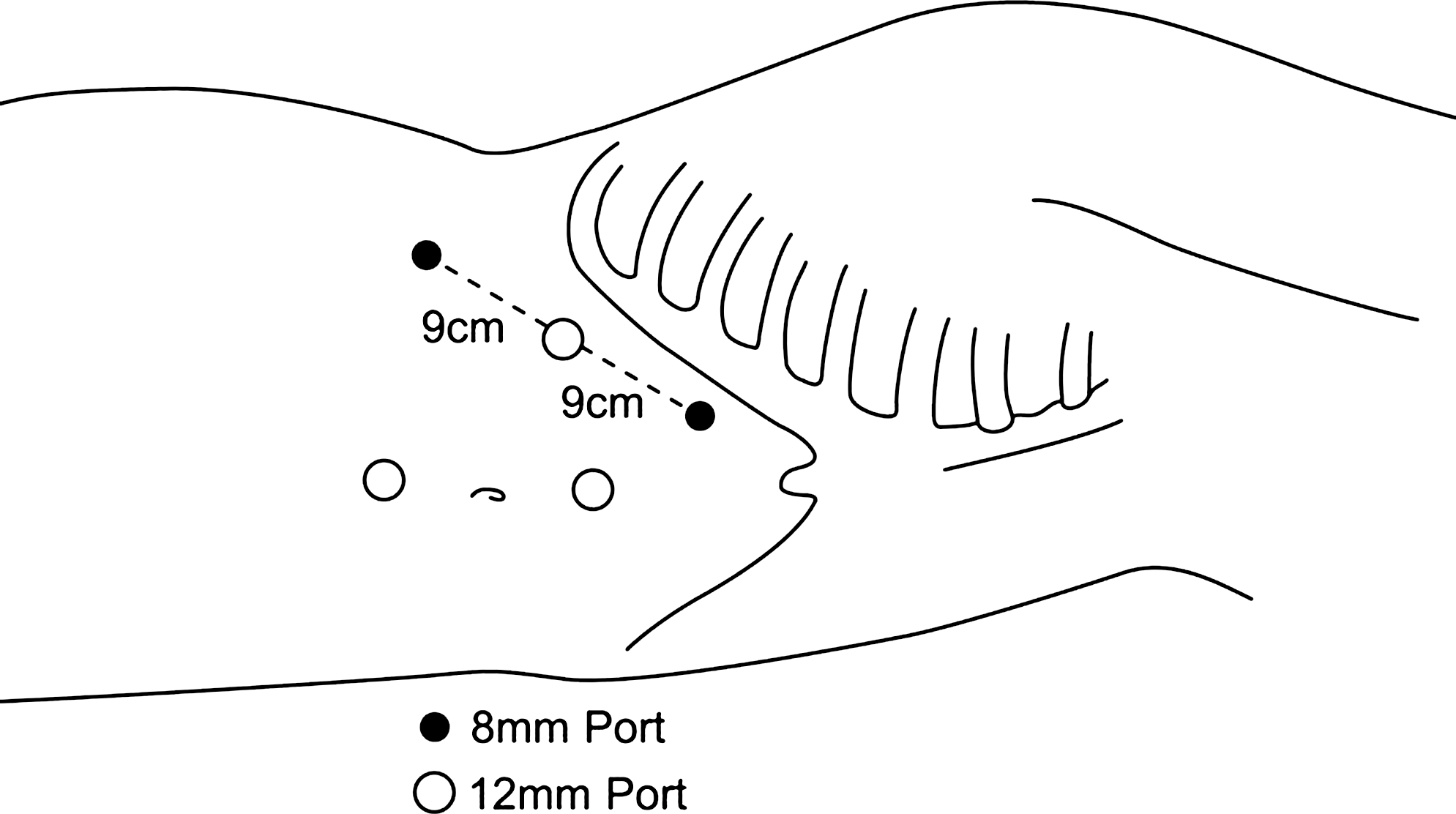
Radiofrequency-assisted robotic clampless partial nephrectomy: port configuration. Patient repositioned in lateral decubitus position. Ports placed in W-configuration.
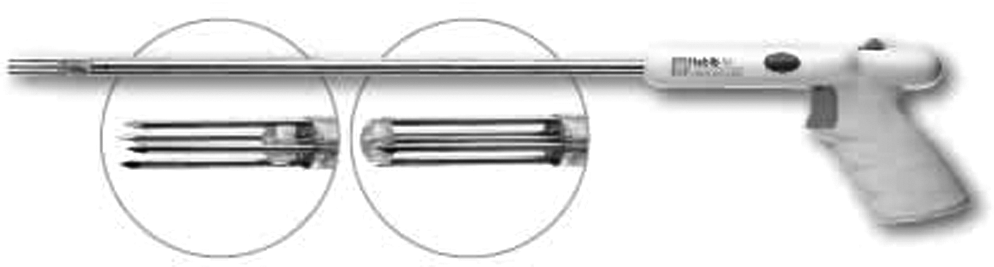
Clampless partial nephrectomy technique. Bipolar radiofrequency ablation probe (RITA Habib 4× laparoscopic with 1500 × generator; AngioDynamics) maneuvered 1 cm from tumor margin in normal parenchyma to create band of coagulation necrosis.
We perform LPN similarly to previously described techniques. 28 We do not place an externalized ureteral stent before LPN. Therefore, collecting system violations after tumor resection are observed by urinary extravasation after intravenous administration of indigo carmine and mannitol (given before clamping).
Results
Preoperative patient characteristics did not differ between groups except in those patients undergoing RF-RCPN who had larger mean radiographic tumor size (2.0 and 2.7 cm, p ≤ 0.007) and more tumors ≥4 cm (2.8 and 16.7%, p = 0.044) (Table 1). Additionally, tumors in the RF-RCPN group were more often endophytic (26 [52.6%] vs. 5 [16.1%], p = 0.0017) and larger on mean pathologic tumor size (2.8 cm [range 0.9–12] vs. 2.0 cm [range 0.5–3.5 cm], p = 0.022). Mean warm ischemia time during LPN was 31.1 minutes (range 0–52). Vascular clamping was never performed in the RF-RCPN group. Mean operative time was longer for the RF-RCPN group (373 and 293 minutes, p ≤ 0.00006) because it included time for cystoscopy, stent placement, and patient repositioning. Mean estimated blood loss did not differ statistically between groups (LPN: 250 cc [range 100–800]; RF-RCPN: 337 cc [range 50–3500]). More RF-RCPN patients required collecting system reconstruction (78.6 and 30.6%, p = 0.00002). No cases in either group required conversion to total or OPN. Mean hospital stay after LPN and RF-RCPN was similar (2.0 and 2.8 days, p = 0.21). Multivariate linear regression models showed technique and tumor size to be predictive of operative time (RF-RCPN, p = 0.0009; tumor size, p ≤ 0.0001). Patient age predicted length of hospital stay (p = 0.0199) (Table 2).
LPN = laparoscopic partial nephrectomy; RF-RCPN = radiofrequency-assisted robotic clampless partial nephrectomy; EBL = estimated blood loss.
BMI = body mass index.
LPN and RF-RCPN group patients had similar rates of complications (overall, urological, and nonurological) (Tables 1 and 3). Urine leak occurred in two patients who underwent LPN (5.6%) and in seven patients in the RF-RCPN group (16.8%, p = 0.12). Urine leaks in the LPN group resolved with prolonged closed suction drainage (5 and 14 days). Of the seven patients in the RF-RCPN group, three patients were managed similarly (5, 6, and 19 days). The remaining four patients required additional procedures to treat urine leaks: ureteral stent only (1) or ureteral stent and percutaneous drain (3). Three patients' leaks resolved at 5, 5, and 10 months. One patient continues to leak 2 months after surgery. Multivariate analysis showed that age was a significant predictor of nonurologic complications (Table 4).
Excludes bleeding complications.
N/Y = no/yes.
Postoperative renal function did not differ with technique (Table 1). Mean length of follow-up (i.e., time from day of surgery to last radiographic follow-up with axial imaging) was significantly longer in the LPN group (25.8 mo vs. 7.8 mo). One patient in the LPN group had a positive margin. One patient in the RF-RCPN group had disease recurrence in his lungs and ribs 1 year after surgery as seen on CT and confirmed with biopsy. This patient is a 63-year-old man who underwent RF-RCPN for a 5.5 cm grade 2 cystic clear cell renal cell carcinoma with negative margins.
Discussion
Our technique of RF-RCPN does not require renal hilar vessel clamping during tumor excision and eliminates the risk of ischemic damage to the kidney. Renal hypothermic techniques for LPN have been developed to minimize renal ischemic insult during hilar clamping, but they are not necessarily widely used or easily achieved. 29 –32 Even warm ischemia time in excess of 20 minutes is associated with a higher incidence of acute and chronic renal failure, increase in serum creatinine >0.5 mg/dL, and need for permanent dialysis. 8 This may limit the type of mass considered appropriate for LPN to small exophytic lesions, especially for inexperienced surgeons. Indeed, initial case series of clampless RFA-assisted LPN primarily treated small polar exophytic lesions, reserving larger, more endophytic or interpolar lesions for resection after vascular occlusion (Table 5). 17,18,22,25 We did not discriminate, based on tumor size or location, which patients should undergo RF-RCPN. Over half of patients in this group had endophytic or interpolar tumors, showing that more complex tumors may be safely resected with our technique. Although renal function did not differ with technique, follow-up was shorter for the RF-RCPN group and more time may be needed to detect an advantage in renal function preservation.
This series combined open and LPN in their results.
This is the current series being described.
N = no; Y = yes.
Both animal and clinical RF-assisted clampless partial nephrectomy series have reported successful hemostasis during tumor excision 17 –22,25,33,34 utilizing monopolar RF devices in conjunction with LPN (Table 4). Bipolar RF devices have been evaluated in animals 33 –35 and OPN in humans 36 but not with laparoscopic/robotic partial nephrectomy. We have found the Habib 4 × device capable of sealing any arterial or venous branch encountered during tumor resection. Intraoperative hemorrhage, however, remains a real concern. We have not converted any cases to open surgery or nephrectomy for bleeding, but two cases in the RF-RCPN group had relatively high estimated blood loss (1.5 L for a 2.3 cm tumor, and 3.5 L for 3.5 cm tumor). Both had posterior left-sided centrally located tumors. In these cases, longer treatment times were required to achieve hemostasis. This may be caused by a heat-sink effect, which causes heat loss from the tissue during RF treatment by thermal conduction/convection (i.e., increased heat loss caused by larger vasculature or proximity to collecting system). 24 This may limit the efficacy of the RF device, whose effect depends on heating the targeted tissue because of ionic friction, resulting in cell death by coagulative necrosis. 34 Indeed, vascular clamping increases the RF lesion size by limiting heat-sink effect. 24
Overall, bleeding complication rates did not differ with technique. The higher complexity of cases in our RF-RCPN group may explain the higher transfusion rate relative to other reported RF-assisted clampless LPN series. 17,18,20 –22,25 Of the two patients who experienced postoperative hemorrhage with RF-RCPN, neither required transfusions for reasons directly attributable to use of the Habib 4× RFA device. One had oozing from a pinpoint hole in the renal vein sustained during dissection, remote from the partial nephrectomy site. The second patient received one unit of packed red blood cells for dizziness upon standing despite stable hemoglobin and hemodynamics. Four patients in the LPN had postoperative hemorrhage. Two required transfusions only for retroperitoneal hematomas. Two patients had persistent arterial tumor bed bleeding necessitating interventional radiology (IR) embolization in one and exploration in the other for hemodynamic instability.
The use of the da Vinci robot facilitates intracorporeal suturing compared with pure laparoscopic techniques. 37 The greater number of urine leaks in the RF-RCPN groups was not completely unexpected because collecting system repair was needed more often as more tumors were endophytic. All repairs were water tight. Although not statistically different, the higher rate of urine leak in the RF-RCPN group (16.8%) is concerning and is relatively high compared with rates in OPN (2.3–17%) 3,38 and LPN series (2.1–6.4%). 3,39 –41 Monopolar RF-assisted LPN porcine models demonstrated that RF energy does not seal collecting system violations. 42 Histologic evaluation of RF-treated kidneys shows that a zone of necrosis in the parenchyma ranging from 3 to 9.6 mm may be induced around the active tine of the RF device during coagulation. 24,33,34 This suggests thermal injury to the collecting system resulting in delayed tissue slough and repair breakdown as an etiology for leaks observed in the RF-RCPN group. Further, the presence of ablated and subsequent necrotic tissue in the area of resection may delay closure of the collecting system. The leaks seen in three patients in the RF-RCPN group that required prolonged ureteral stenting may have resulted from a combination of the aforementioned delayed tissue slough as well as unrecognized collecting system violations and patient comorbidities that may have affected wound healing (e.g., two of the three patients had diabetes mellitus).
Regarding oncologic efficacy, no positive margins occurred in the RF-RCPN group. Because hilar clamping is not done, the surgeon and pathologist can grossly and microscopically examine the specimen to ensure complete tumor extirpation with further resection as necessary. No local and one distant recurrence occurred with RF-RCPN, which is consistent with published laparoscopic radical nephrectomy (LRN) series. 3 Follow-up is relatively short, however, as in other published RF-assisted LPN series. 17 –25
Weaknesses of our study include the nonrandomized and uncontrolled nature of our groups. We may have been more selective, thus introducing bias, when treating patients with LPN because of concerns over warm ischemia time and difficulty of intracorporeal suturing. Further, we began utilizing RF-RCPN later in our collective experience at which point we may have been more comfortable in attempting resection of larger and more complex tumors. The da Vinci robot and the Habib 4× device are expensive technologies that may limit its availability. Finally, long-term renal function and oncologic efficacy data are not available for RF-RCPN.
Conclusions
RF-RCPN appears to be equivalent to LPN with regard to complication rate, postoperative renal function, and oncologic efficacy, with limited follow-up. Longer operative times in the RF-RCPN group are a result of cystoscopy, stent placement, repositioning, and early surgeon experience. RF-RCPN allows intraoperative evaluation of surgical margins and resection of larger centrally located tumors without time constraints of renal ischemia. Evaluation of this promising technique with randomized controlled study is warranted.
Footnotes
Disclosure Statement
Robert B. Nadler is a speaker for Angio Dynamics and Intuitive Surgical.