
Abstract
Aim:
To investigate the accuracy of percutaneous cryoablation for kidney tumors performed under combined real-time ultrasonography (US) and three-dimensional (3D) CT scan navigation in a porcine model.
Materials and Methods:
After percutaneously injecting 2 to 6 tumor mimic lesions in 11 pigs, a CT scan was performed and digital data were saved into a navigation system (Real-Time Virtual Sonography® [RVS]) that allows 3D reconstruction and synchronization with real-time US images. The cryoprobe was guided percutaneously into the kidney tumor mimic, and ice ball formation was monitored continuously during cryoablation using the RVS system. Kidneys were harvested and sent for gross pathologic and histopathologic analysis at days 0, 15, and 30 postoperatively.
Results:
Thirty-five renal tumor mimics were created and treated by percutaneous cryotherapy; tumor mimic locations were as follows: 16 tumors (46%) in the lower pole, 14 (40%) in the central region, and 5 (14%) in the upper pole. Eleven tumor mimics (31%) were intraparenchymal, and 24 (69%) subcapsular. The synchronization between the CT scan 3D reconstructed images and real-time US was successful in all cases. The mean tumor size was 2 cm (range, 1.2–4 cm). Mean cryonecrosis size was 3.3, 3.7, and 2.8 cm at days 0, 15, and 30, respectively. Three (8.5%) positive margins were found on the macroscopic and microscopic analysis.
Conclusions:
RVS imaging system synchronizing real-time US with preoperative CT scan is a feasible and safe technique for percutaneous probe ablation of kidney tumors.
Introduction
Materials and Methods
After development of the percutaneous technique using the RVS in one pilot animal, the procedure was performed in 10 consecutive female farm pigs, weighing between 30 and 37 kg. The study protocol was approved by our Institutional Animal Care and Use Committee.
Surgical navigation
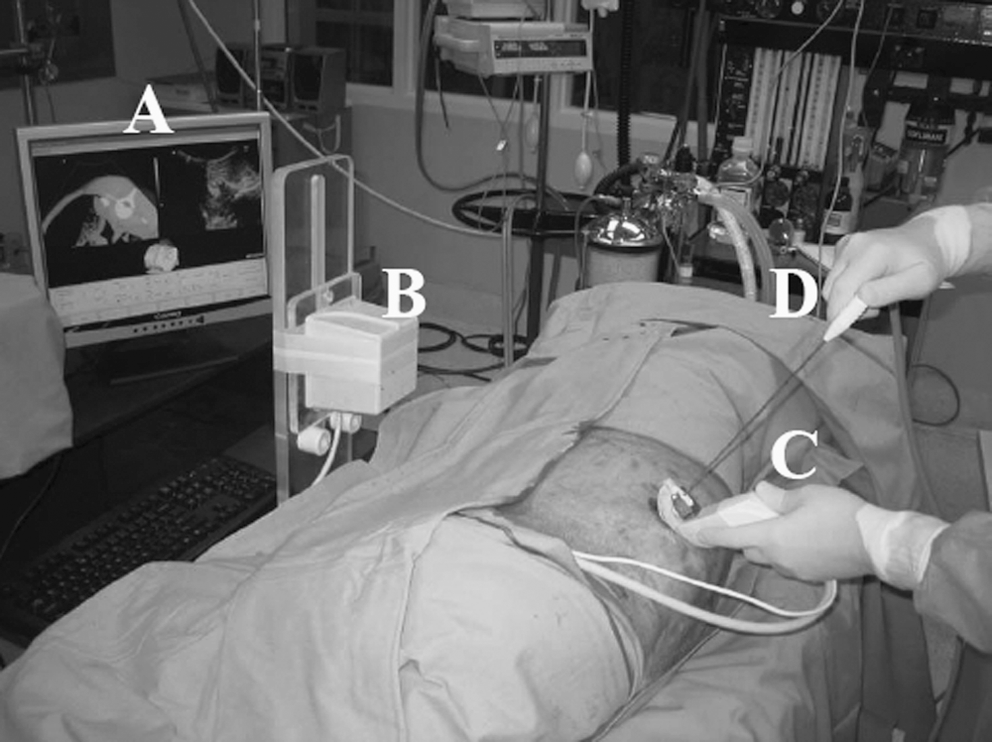
The RVS consists of a magnetic field generator placed beside the pig body, magnetic motion-tracking device on the US probe, standard US equipment, and image-processing workstation. A magnetic sensor fastened to the US probe registers and transmits to the workstation the 3D location and orientation of the probe within the generated magnetic field. The workstation then processes the preoperative helical CT volume data (Figs. 1 and 2). To correlate the US and CT images, three fiduciary markers are placed on the pig before CT scan. After the CT scan, the US probe with the magnetic sensor is sequentially placed on each of three fiduciary markers and correlated with the same fiduciary marker visible on the corresponding orthogonal CT slice. After calibration, the workstation reconstructs and displays the synchronized CT scan image with intraoperative real-time US image on a split screen display (Fig. 3).

(
(
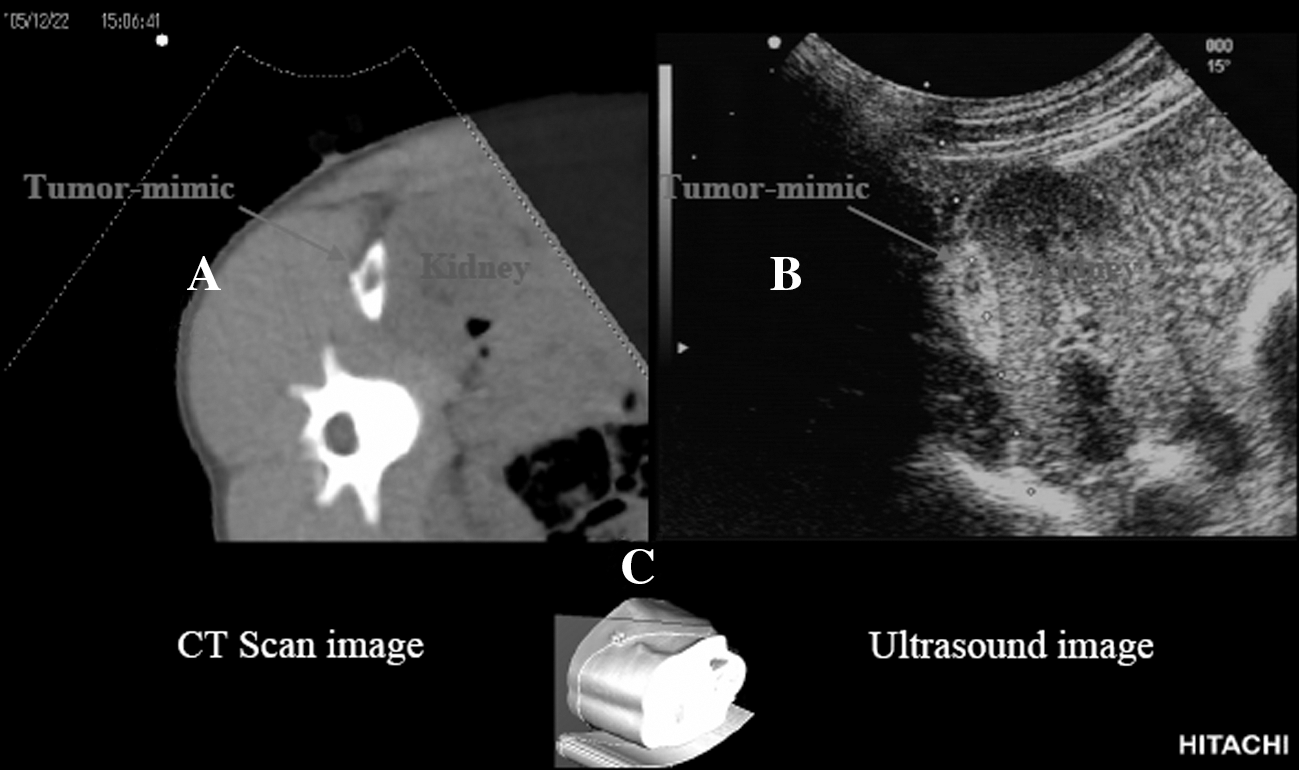
Screen display: the RVS system reconstructs and displays the synchronized (
Tumor target creation
Kidney tumor target was created by CT-guided percutaneous injection of a tumor mimic mixture designed for easy recognition on both US and CT scan. The mixture was prepared by combining 6 g of agarose, 12 g of natural fiber, 14 mL of glycerol, 3 mL of the contrast medium (76%), 2 mL of methylene blue and 40 mL of sterile water. The mixture was heated to just under its boiling point in a microwave oven and then cooled to 60°C before being injected slowly using a 20-gauge needle (Fig. 4). Three grams of iron sand was added to the mixture for greater hyperechogenicity. 7,8
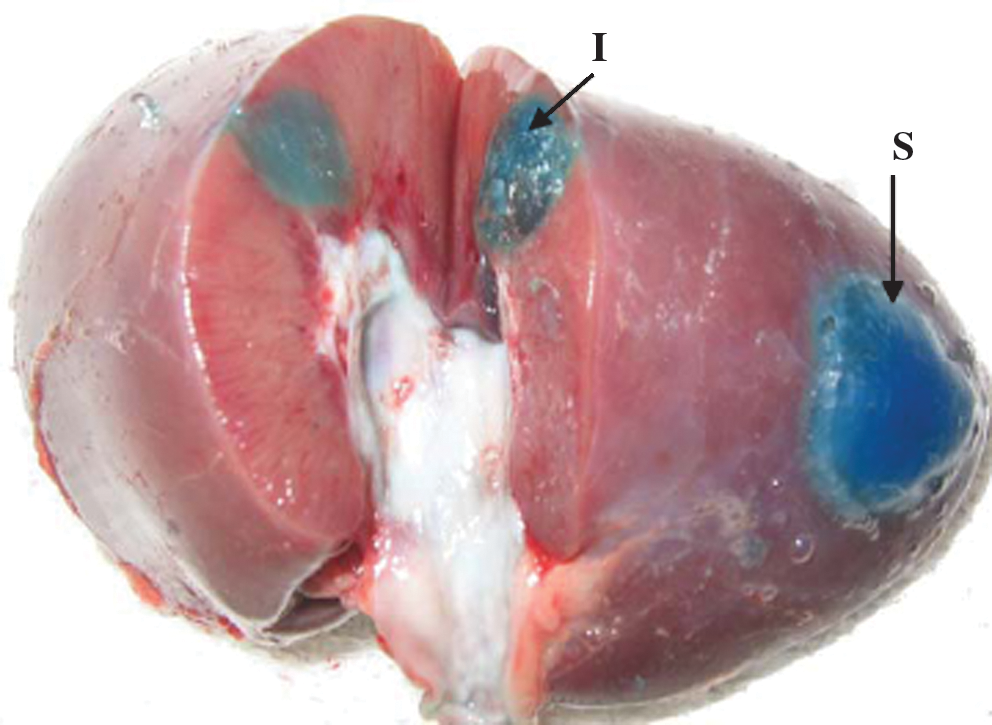
Intraparenchymal and subcapsular agar gel tumor mimic model injected percutaneously and used as a target for the cryoprobe placement. I = intraparenchymal; S = subcapsular.
Pilot group (one animal)
Two tumor mimic lesions were created in the right kidney of the pilot animal, and the kidney was then harvested without cryoablation to develop our technique of tumor mimic injection. Upper and lower poles of the pilot animal's left kidney were cryoablated without previous tumor mimic creation, to practice image calibration and synchronization.
Study group (10 animals)
After achieving two to six intraparenchymal and/or subcapsular tumor mimic lesions suitable for percutaneous cryoablation, we took CT images of each animal and transferred the data to the RVS. Under real-time US and 3D reconstruction CT scan, we guided the cryoprobe into each kidney tumor mimic, and cryoblated with two consecutive freeze–thaw cycles. Ice ball formation during cryoablation was monitored continuously. Tumors that were created in contact with bowel or vessels or those that had extravasated into the collecting system were not treated.
Two animals were euthanized at the conclusion of the procedure for technical validation; the remaining eight animals underwent laparoscopic right nephrectomy at day 15 and left nephrectomy on euthanasia at day 30. Kidneys were sent for gross pathologic and histopathologic analysis.
Percutaneous cryoablation
A single PERC-24, R2.4 CryoProbes™ (Endocare, Irvine, CA), was percutaneously placed with RVS system guidance into the previously created kidney tumor mimic. If the tumor size was >2 cm, two PERC-17, R1.4 CryoProbes were used. After the probe position was optimized and confirmed, real-time US monitoring was used during the development of ice ball formation and cryoablation process. At the completion of two freeze–thaw cycles, the probe was removed. Cryoablation was repeated in the same manner on the contralateral kidney.
Data collection
Data were collected prospectively as the study progressed. Created tumor mimics were categorized as hyperechoic (with iron sand), hypoechoic (without iron sand), intraparenchymal (endophytic on CT images), or subcapsular (exophytic on CT images). Ease of synchronization of US and CT scan images at various locations was noted. Ice ball diameter and ablated zone were correlated. Histopathology was reviewed for evidence of untreated tumor margins.
Results
Overall results
A total of 48 tumor mimic lesions were injected percutaneously. Two tumor mimics were injected in the first pilot animal to develop the technique of tumor creation and thus not cryoablated. Eleven tumor mimic lesions were excluded because of extravasation in the collecting system (n = 5) or location in contact with bowel or renal vessels (n = 6). Thus, 13 of 48 tumor mimic lesions were not cryoablated using the RVS system. The remaining 35 tumors were treated and thus included in the study.
Of the 35 tumor mimics, 22 (62.8%) were hyperechoic and 13 (37.2%) were hypoechoic on US (Table 1); 16 tumors (45.7%) were localized to the lower pole, 5 (14.3%) to the upper pole, and 14 (40%) to the central region. Eleven tumors (31.4%) were intraparenchymal and 24 (68.6%) were subcapsular. All lesions were identifiable on CT scan, US, macroscopic study, and pathology. The mean ablation diameter was 3 cm when performed on the kidney parenchyma, and 2.8 cm when performed on the tumor mimic (p > 0.99). The mean ice ball diameter was 3 cm. Synchronization between the CT image and real-time US was achieved over a mean time of 14.8 minutes (5–35 minutes). Time to synchronization was greater for hypoechoic tumors (27.7 minutes) compared with hyperechoic tumors (6.1 minutes; p < 0.0001). Time for synchronization decreased significantly with the learning curve (R 2 = 0.8; p < 0.0001) (Fig. 5). Two animals (5.7%) developed a retroperitoneal urinoma that was discovered at day 15, and one animal (2.8%) sustained a skin burn caused by ice ball extension at the time of cryoablation.
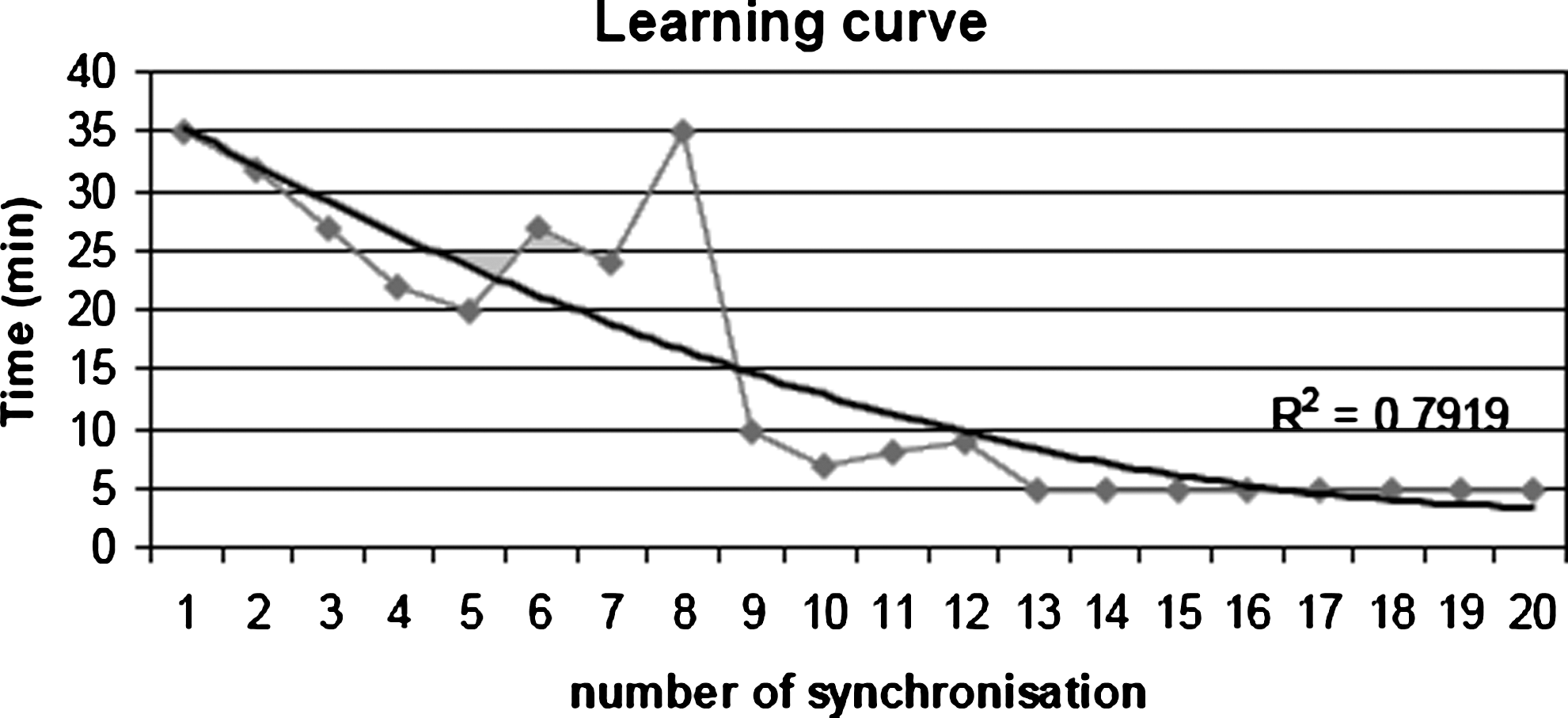
Learning curve of the time needed to acquire a synchronization between US and CT scan images.
Macro- and microscopic study
Mean cryonecrosis size was 3.3, 3.7, and 2.8 cm at days 0, 15, and 30, respectively. Three positive margins (8.5%) were observed on gross pathology and confirmed on histopathologic analysis (Figs. 6 –8). Two positive margins were observed in the group of 13 hypoechoic tumors and 1 in the group of 22 hyperechoic tumors (p = 0.28). We also observed 2 of 11 positive margins and 1 of 24 positive margins in the intraparenchymal tumor group and subcapsular tumor group, respectively (p = 0.17).

Acute group negative margin: renal parenchyma with vascular congestion (left). A 1 mm rim of renal tubules showing coagulative necrosis (arrow ↑) caused by cryoablation completely surrounds the gel (right) (H&E, 40 × ). g = gel; c = renal capsule; p = renal parenchyma; n = coagulative necrosis. H&E = hematoxylin and eosin.
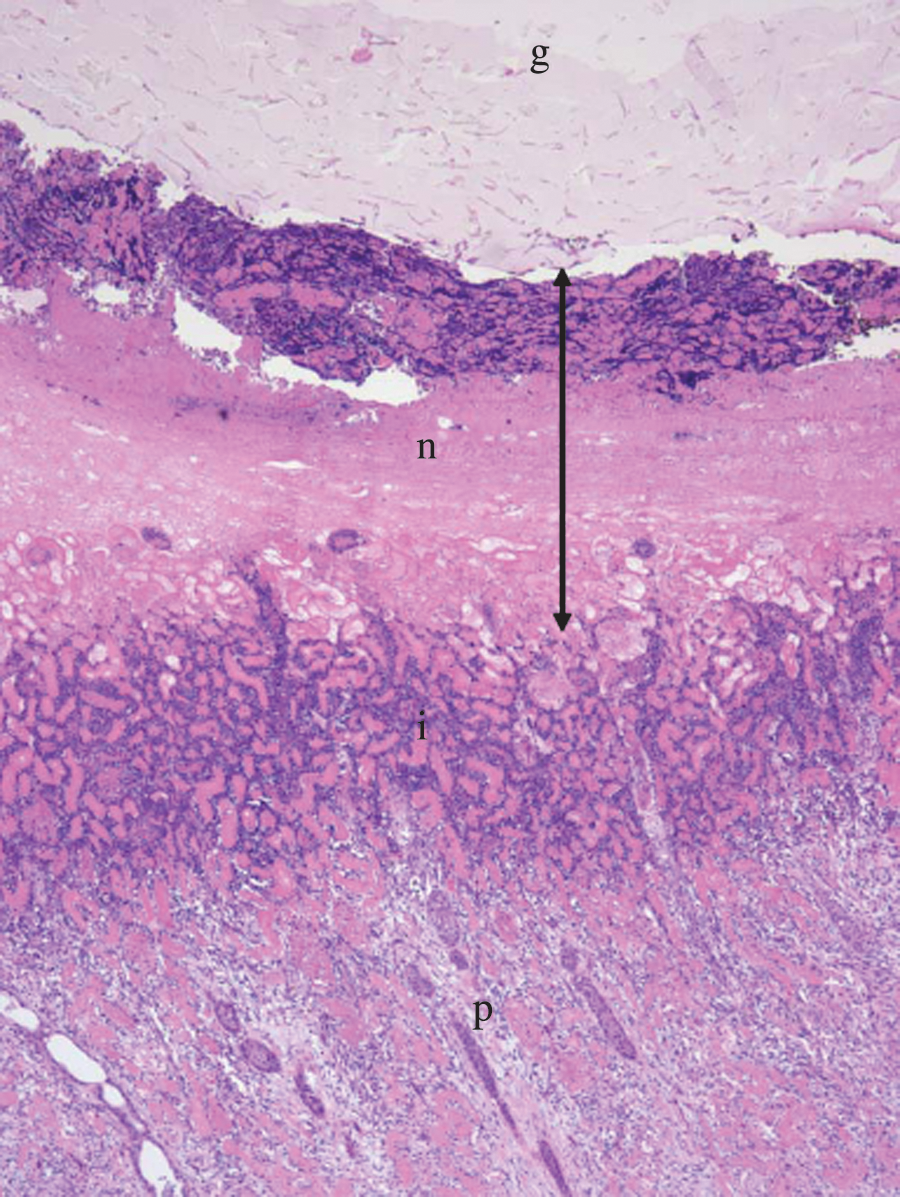
At 15 days the rim of coagulative necrosis is approximately 4 mm (arrow ↕). Beneath the necrosis, there is a rim of injured tubules (i) (H&E, 100 × ). g = gel; p = renal parenchyma; n = coagulative necrosis.
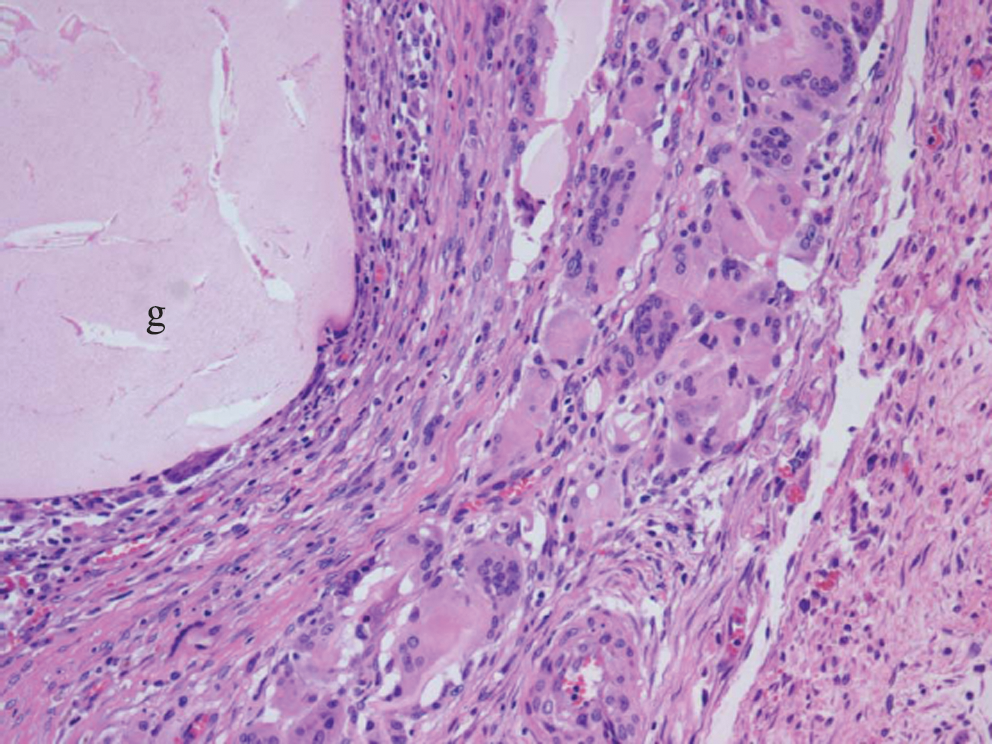
At 30 days the gel (g) is surrounded by a rim of fibroblasts and chronic inflammatory infiltrates, with a foreign body–type giant cell reaction (H&E, 200 ×).
Discussion
Percutaneous needle ablation is assuming an increasingly prominent role in the minimally invasive treatment of renal tumors. Precise needle placement is essential for successful ablation. Thus, good-quality and real-time images are needed. By combining CT scan data and real-time US images, RVS offers the potential for a precise needle placement while reducing radiation exposure.
Using RVS, synchronization was assessed by comparing the real-time US images with the detailed CT scan images at different section levels and angles. Synchronous overlapping of the real-time US and CT images allowed for maintenance of accurate orientation.
Several factors may influence the accuracy of tumor mimic targeting, as assessed in the present study. The distortion of the magnetic field caused by metallic operating table, CT scan suit, and probes required repetitive CT/US image fusion. The case of hypoechoic or upper pole tumor synchronization was more challenging because of difficulty of observation.
We took specific measures to improve repeatability and accuracy. CT acquisition should be performed in the same position as the procedure to avoid intraabdominal organ movement.
A more user-friendly synchronization process with a validation protocol will be reassuring before any needle placement.
A targeting needle guideline on the CT scan view and the ability of the system to dynamically adjust the CT images to kidney movements during needle placement would be of great benefit.
The two animals that developed a urinoma, a rare finding after percutaneous cryoablation, had been treated for lower pole intraparenchymal tumors. Both animals had a retroperitoneal urinoma with over 1 L of fluid discovered at day 15 during the nephrectomy without any sign of distress preoperatively. This finding could be explained by large area of cryonecrosis.
A randomized trial comparing the RVS system with standard CT-guided percutaneous cryoablation is needed to adequately evaluate this new approach.
RVS could be adapted to different types of renal percutaneous procedures, such as renal biopsy and percutaneous nephrostomy.
Further, MRI/US fusion technology could be applied for targeted biopsy and focal therapy of prostate cancer.
Conclusion
Percutaneous cryoablation of selected small kidney tumors under combined real-time US and 3D navigation is feasible and safe. It resulted in precise guidance for intrarenal cryoprobe positioning and real-time monitoring of the entire ice ball created. However, the RVS system required repetitive synchronization because of significant kidney movement.
Footnotes
Disclosure Statement
No competing financial interests exist.