
Abstract
Introduction:
The use of surgical clips as suture anchors has made laparoscopic partial nephrectomy (LPN) technically simpler by eliminating the need for intracorporeal knot tying. However, the holding strength of these clips has not been analyzed in the human kidney. Therefore, the safety of utilizing suture anchors is unknown as the potential for clip slippage or renal capsular tears during LPN could result in postoperative complications including hemorrhage and urinoma formation. With the above in mind, we sought to compare the ability of Lapra-Ty clips and Hem-o-lok clips to function as suture anchors on human renal capsule.
Methods:
Fresh human cadaveric kidneys with intact renal capsules were obtained. A Lapra-Ty clip (Ethicon, Cincinnati, OH) or a Hem-o-lok clip (Weck, Raleigh, NC) was secured to a no. 1 Vicryl suture (Ethicon) with and without a knot, as is typically utilized during the performance of LPN. The suture was then placed through the renal capsule and parenchyma and attached to an Imada Mechanical Force Tester (Imada, Northbrook, IL). The amount of force required both to violate the renal capsule and to dislodge the clip was recorded separately.
Results:
Six Lapra-Ty clips and six Hem-o-lok clips were tested. The mean force in newtons required to violate the renal capsule for the Lapra-Ty group was 7.33 N and for the Hem-o-lok group was 22.08 N (p < 0.001). The mean force required to dislodge the clip from the suture for the Lapra-Ty group was 9.0 N and for the Hem-o-lok group was 3.4 N (p < 0.001). When two Hem-o-lok clips were placed on the suture in series, the mean force required to dislodge the clips was 10.6 N.
Conclusion:
When compared with Lapra-Ty clips, using two Hem-o-lok clips may provide a more secure and cost-effective method to anchor sutures on human renal capsule when performing LPN.
Introduction
Because of the above technical challenges, surgical clips have been used in laparoscopic surgery as suture anchors. 1,2 These are the devices that are substitutes for knots, and by placing a clip on the distal end of the suture and one on the proximal end, the need for knot tying is obviated. In doing so, suture anchors can make LPN technically simpler by eliminating the need for intracorporeal knot tying. 3
Suture anchors can fail, however, and in the context of a LPN can lead to significant complications including hemorrhage or urinary extravasation. Suture anchor failure generally occurs in two situations: (1) insufficient holding strength causes the anchor to slip on the suture or (2) anchors placed at the renal capsule to hold the suture can tear through the capsule and into renal parenchyma.
The holding strength of surgical clips has not been described when used on human kidneys with intact renal capsules. Therefore, we sought to compare the performance of two commonly used laparoscopic suture anchors (Fig. 1) and determine the type and combination of clips that yielded the optimal result.
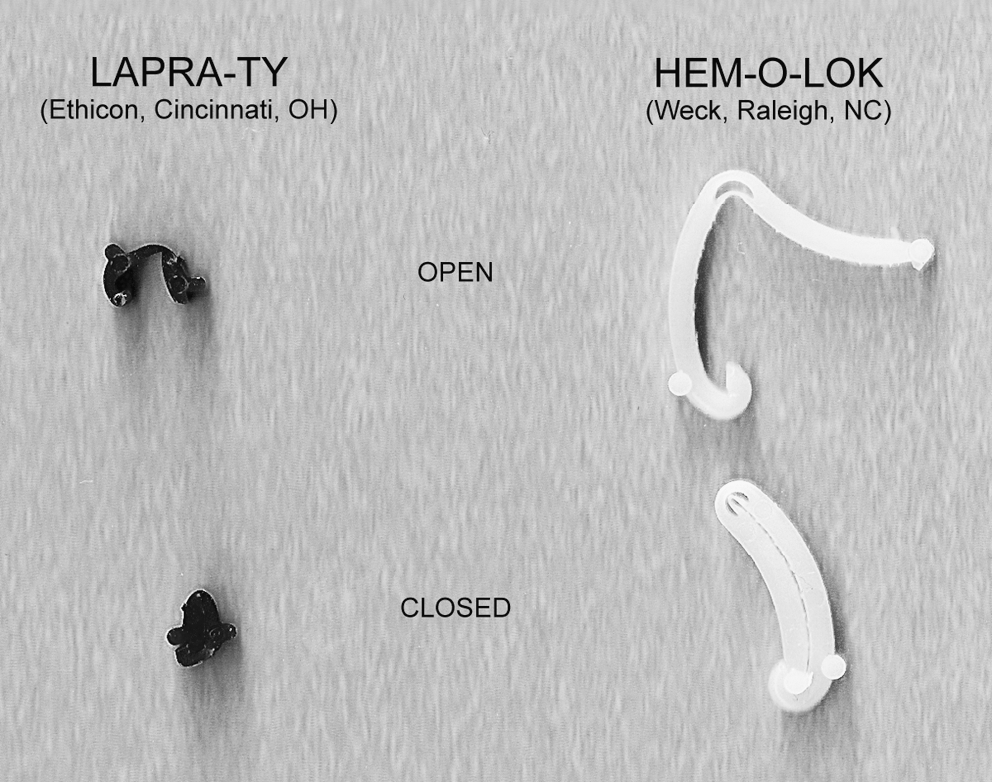
Lapra-Ty and Hem-o-lok clips in the open and closed position.
Methods
Fresh, nonfixed, human cadaveric kidneys with intact renal capsules were acquired from autopsies after appropriate consent was obtained. The kidneys were sectioned coronally into halves. A single knot was placed on the end of a no. 1 polyglactin (Vicryl) suture (Ethicon, Cincinnati, OH), and a Lapra-Ty clip (Ethicon) or a large Hem-o-lok clip (Weck, Raleigh, NC) was secured to the suture abutting the knot. The suture was then drawn through the renal capsule and parenchyma, until the suture anchor rested against the renal capsule. A loop was tied into the suture at 14 cm of length and attached to an Imada Mechanical Force Tester (Imada, Northbrook, IL). The kidney was then secured in a stationary frame. The force tester was pulled by hand, and the amount of force required for the anchor to violate the renal capsule was recorded (Fig. 2). Each type of clip was tested for a total of six times.
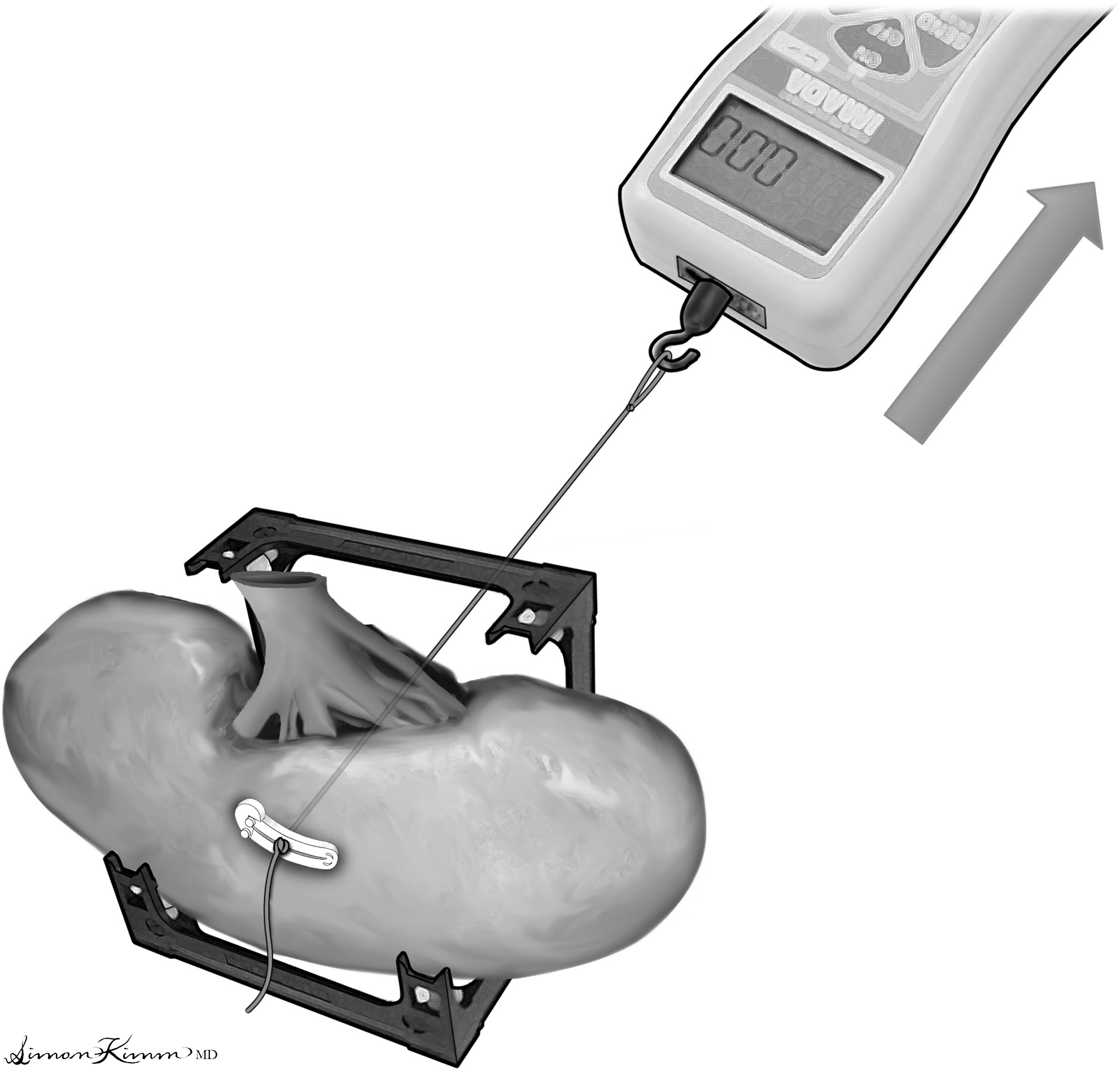
A hand-held force tester was used to measure the point at which the suture anchor violated the renal capsule.
Next a suture anchor was applied to a no. 1 Vicryl suture, without a knot, and placed in a frame to stabilize the suture anchor. The force required to displace the clip from its applied position, or holding strength, was measured. Trials were performed with both Lapra-Ty and Hem-o-lok clips. This process was repeated with two clips in series for each of the clips. Ultimately, the force required to dislodge a single Lapra-Ty clip, a single Hem-o-lok clip, and two Hem-o-lok clips was measured. The mean values were calculated and compared using a paired t-test.
Results
The Hem-o-lok clip required a mean force of 22.1 N (standard deviation [SD] 7.02), and the Lapra-Ty clip required a mean force of 7.3 N (SD 2.16) to violate the renal capsule. The data were analyzed using a t-test, and the difference was found to be statistically significant at p < 0.001 (Fig. 3).
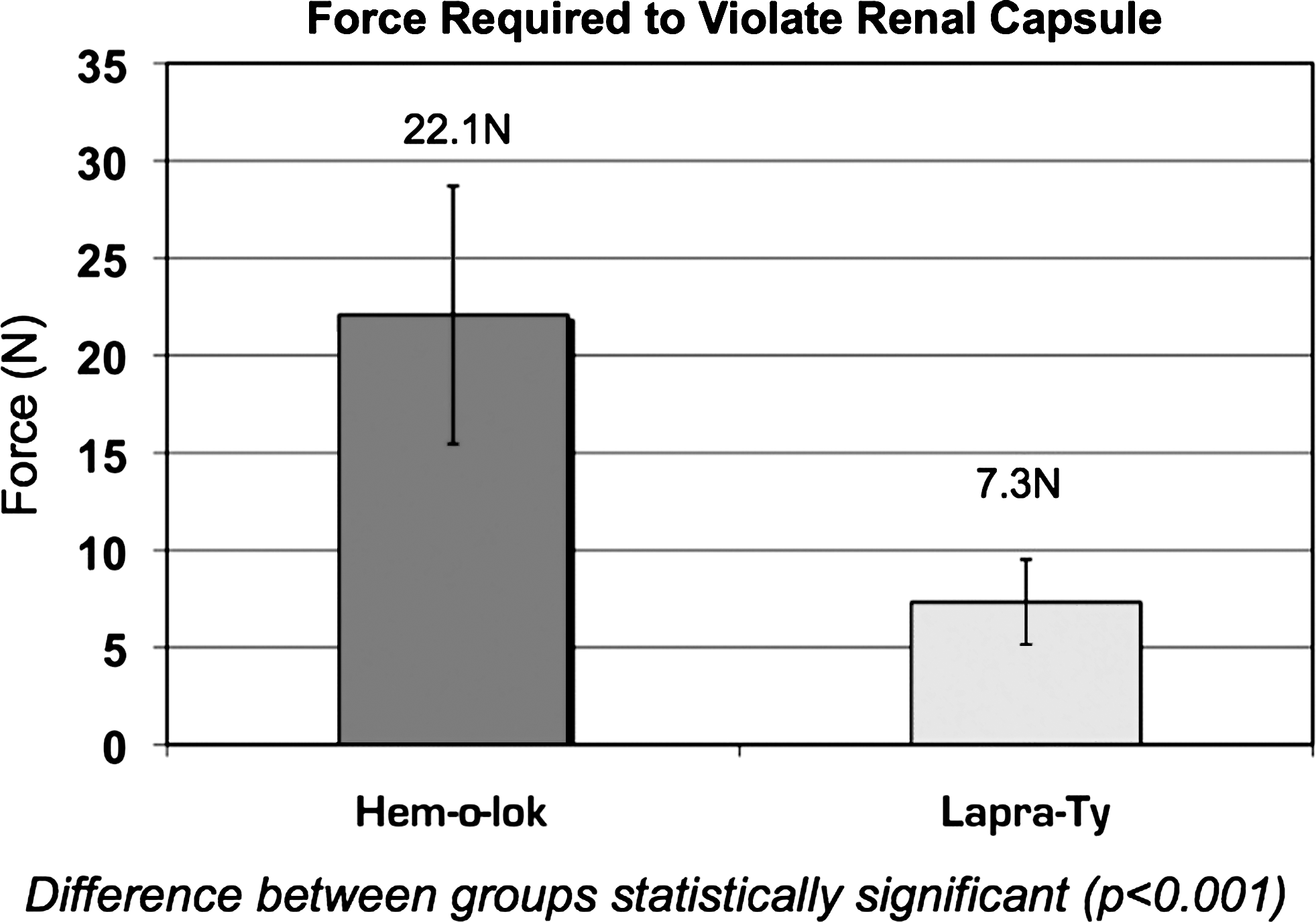
Force required to violate the renal capsule by the Hem-o-lok and the Lapra-Ty clip. The data were analyzed using a t-test, and the difference was found to be statistically significant at p < 0.001.
The holding strengths, or force required to dislodge the clips from the suture, are summarized in Figure 4. A single Hem-o-lok clip required a mean force of 3.4 N (SD 1.30) to be dislodged from its applied position on the suture. A single Lapra-Ty clip required a mean force of 9.0 N (SD 2.91). When two Hem-o-lok clips were placed immediately in series on the suture, the mean force required to dislodge them from the suture increased to 10.6 N (SD 3.02).
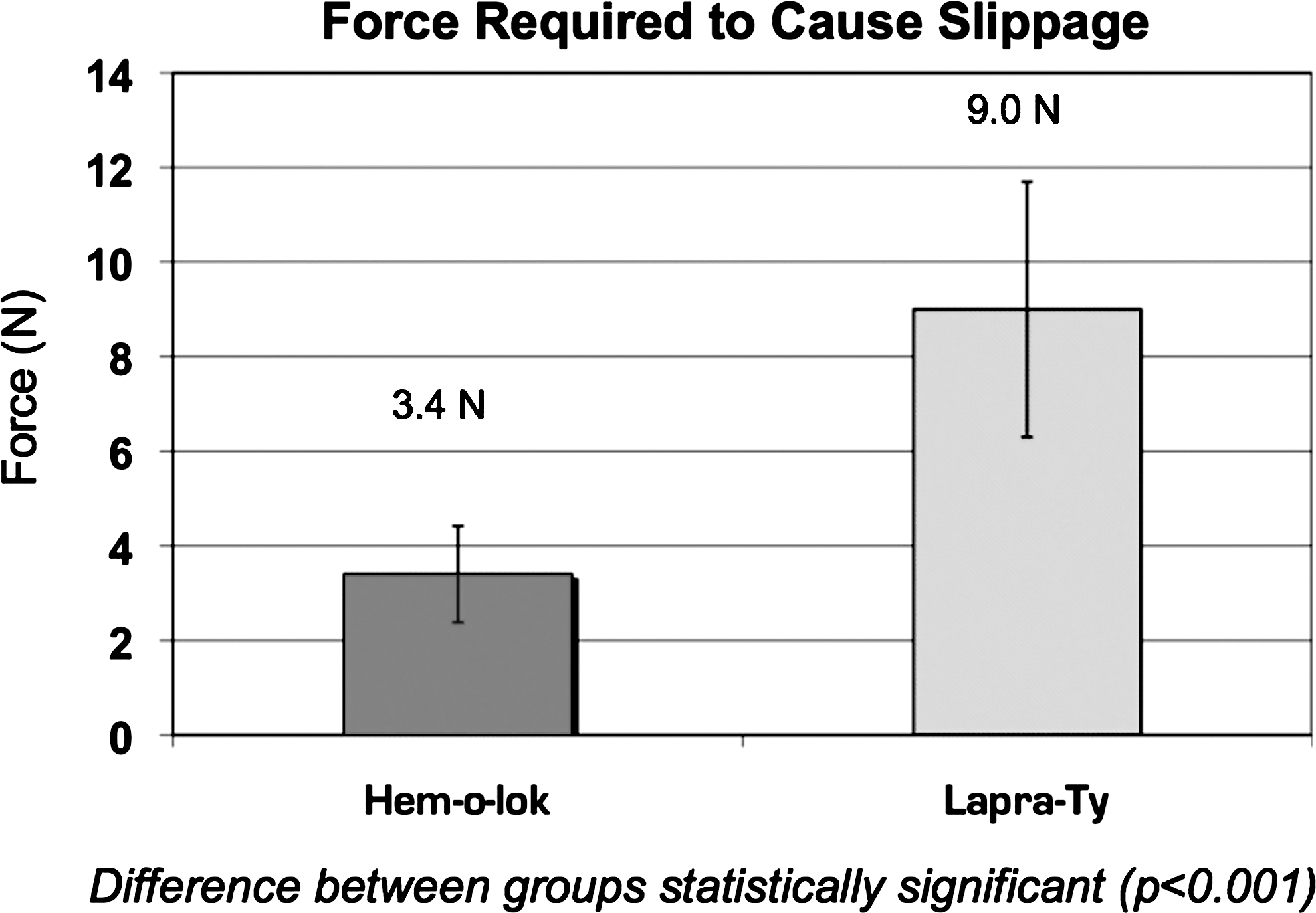
The force required to dislodge a single Hem-o-lok or Lapra-Ty clip from its applied position on the suture. This is a measure of the clip's holding strength.
A single Hem-o-lok clip required significantly less force to be displaced when compared with a Lapra-Ty clip (p < 0.05). Placing two Hem-o-lok clips in series on the suture greatly increased the overall holding strength to 10.6 N. When compared, the force that displaced two Hem-o-lok clips was not significantly different to that required to dislodge a single Lapra-Ty clip, shown in Figure 5 (p > 0.05). Figure 6 summarizes the clips used as suture anchors and the forces they can hold.
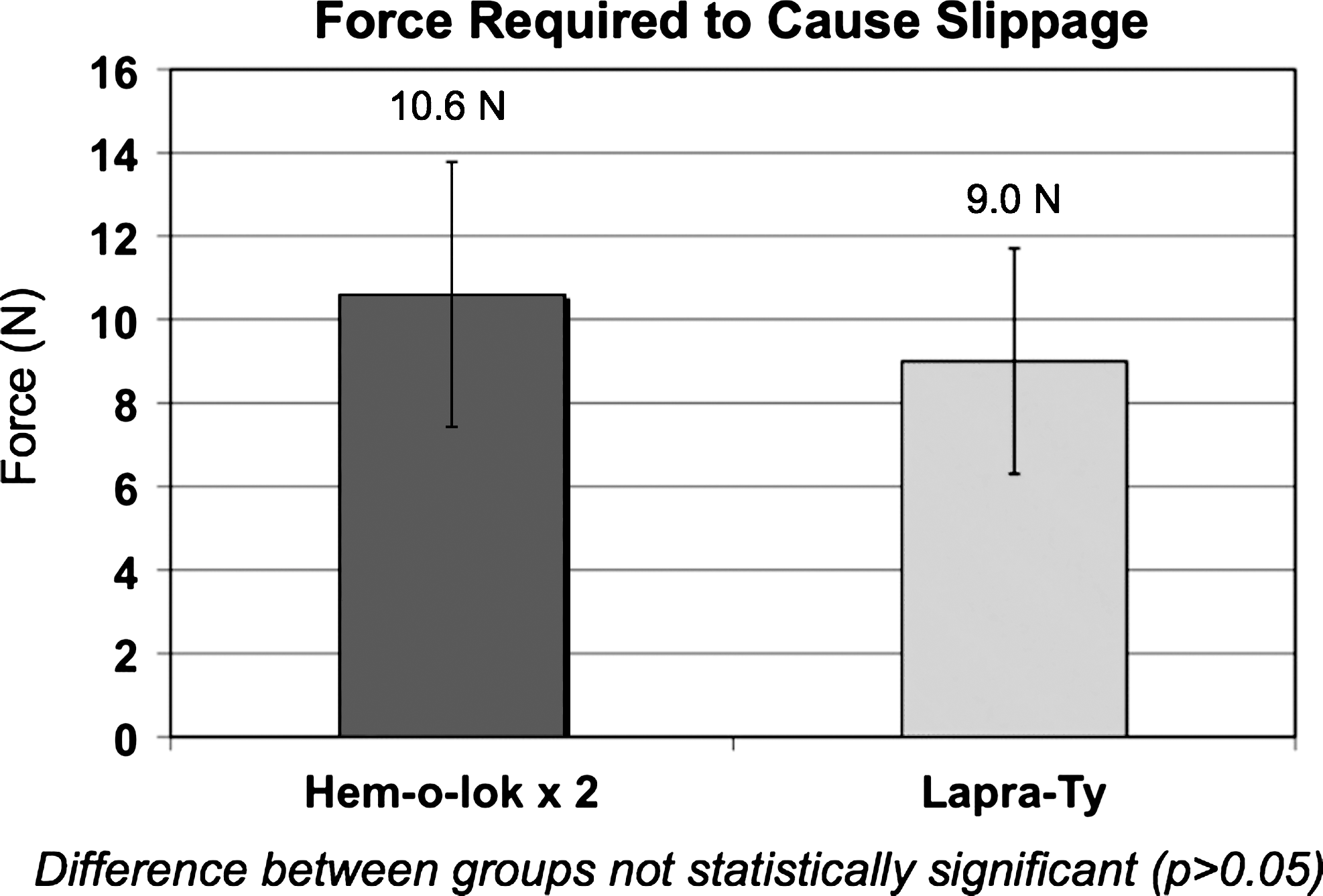
The force required to dislodge a single Lapra-Ty clip or two Hem-o-lok clips from its applied position on the suture. The two Hem-o-lok clips are applied immediately adjacent to one another, increasing the overall holding strength.
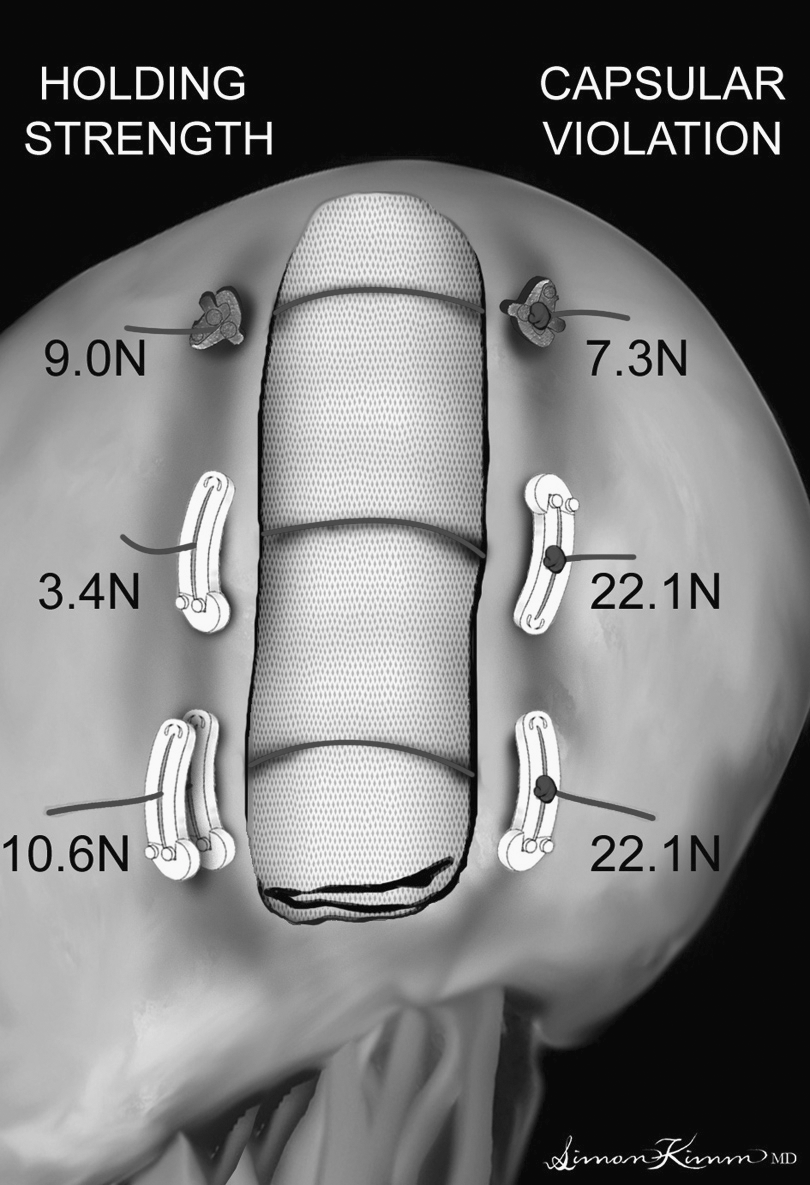
Securing a bolster after partial nephrectomy using either Lapra-Ty clips (dark) or Hem-o-lok clips (white). The force required to violate the renal capsule is displayed on the knotted side of the suture (right), and the force required to cause slippage is displayed on the unknotted side (left). The use of a single Hem-o-lok clip on the knotted side and double Hem-o-lok clips on the unknotted side resulted in the most secure anchor.
Discussion
Suture anchors are devices that, if used properly, can safely and effectively minimize the need for intracorporeal knot tying. 1 Several types of suture anchors exist, and this study focuses on two clips that are in common use today. The Lapra-Ty clip is a locking absorbable polydioxanone clip that can be used for either single suture placement or running sutures. They hold their strength for 14 days, are totally absorbed by 13 weeks, and are designed to anchor a single strand of polyglactin suture. 4 The Hem-o-lok clip is made from a nonabsorbable polymer and comes in four sizes (medium, medium-large, large, and extra-large). They are designed primarily to ligate small vessels, but can serve to anchor sutures, with the large size most often utilized for this purpose. The Hem-o-lok clip also features a locking mechanism, to prevent inadvertent clip opening after being engaged.
Failure of these devices can occur either through inadequate holding strength or tearing of the tissue by suture and anchor. In the two devices we tested, the Lapra-Ty clip had a greater tendency to violate the renal capsule than the large Hem-o-lok clip. Suture holding strengths are not an issue here, as the clips were placed against a knot that prevents sliding; however, a much greater force was necessary for the Hem-o-lok clip to tear the renal capsule. The reason for this is attributable to the Hem-o-lok clip's larger physical profile, as potentially lacerating forces are distributed across a larger surface area. Also the Hem-o-lok clip features flat surfaces, which are less likely to tear into the capsule. In contrast, the Lapra-Ty clip has a smaller profile, which does not dissipate forces as widely, and has sharp edges that can cut into the capsule, leading to capsular violation. The phenomenon of capsular violation is not a common occurrence during the performance of LPN. However, should it occur, it could have serious consequences. When capsular tearing occurs during the clip placement, it causes additional bleeding and an increase in warm ischemia time as the failed clip and suture need to be removed and a new one placed in a slightly different location. Our data suggest that the use of Hem-o-lok clips will minimize this possibility.
When suture holding strengths were compared, the Hem-o-lok clip was inferior to the Lapra-Ty clip. The forces we measured were comparable to the findings in previous studies. 5 Because the Hem-o-lok clip is designed primarily as a vascular ligation clip and not as a suture anchor, sliding is a greater possibility. It should be noted that although a force of 9.0 N was required to dislodge the Lapra-Ty clip, this exceeded the 7.3 N of force at which the Lapra-Ty clips tore through the renal capsule. Therefore, clip failure will occur at this lower force, as suture tension is lost when the renal capsule is violated. By contrast, the large Hem-o-lok clip will tear through the capsule at 22.1 N of force, but failure of the clip is more likely to occur by suture slippage at 3.4 N for a single clip, or 10.0 N for double placement. In the clinical setting, the time required to apply a second clip is minimal, as it is applied immediately adjacent to the first clip, which has been properly tensioned.
A previous study demonstrated renal parenchymal laceration by sutures in porcine kidneys at a relatively low force of 2.2 N (±0.3). 6 However, to date, no study has utilized human kidney tissue to evaluate force vectors. In our study, we showed that human renal tissue has much more strength than its porcine counterpart. Previous studies have also demonstrated, as our study did, that Lapra-Ty clips have superior holding strength when compared with Hem-o-lok clips on no. 1 Vicryl suture. However, this advantage of the Lapra-Ty clip is undermined by its greater tendency to violate the renal capsule. Based on our findings, the use of a single Hem-o-lok clip on the knotted side and double Hem-o-lok clips on the unknotted side resulted in the most secure anchor (Fig. 6).
We measured the linear force at which each clip caused tearing of the renal capsule. Expressing these forces as a pressure may be more clinically meaningful and reveals the effect of clip size in renal capsular tearing. This calculation is made by dividing the force (N) by the area of the clip face (mm2), then applying a conversion factor to determine the pressure in millimeters of mercury (mm Hg). The large Hem-o-lok clip violated the renal capsule at a force of 22.1 N. The face of this clip has an area of 33.7 mm2, generating a pressure of 4916 mm Hg. The Lapra-Ty clip, which has an area of 7.5 mm2 facing the renal capsule, tore the renal capsule at a force of 7.3 N and a pressure of 7331 mm Hg. These calculations show that Lapra-Ty clips generated higher pressures than large Hem-o-lok clips, and these pressures increased more rapidly with increases in applied tension. In addition, because capsular violation occurred at different clip pressures for the two clip types, we can infer that pressure is not the only factor in causing capsular tearing, but other physical characteristics such as clip shape and material may play a prominent role as well.
Cost is also a potential consideration when selecting clips. Based on the 2009 data, the Lapra-Ty system costs US $2375 for the applicator and US $54.39 for a cartridge of six clips (US $9.06 per clip). The Hem-o-lok system uses an applicator that costs US $1195, and a cartridge of six clips is US $19.71 (US $3.28 per clip). 6 On a clip-for-clip basis, the Hem-o-lok system shows a substantial cost advantage, at 36% of the cost.
Based on these data, surgeons can select among different clips, or use combinations of clips, to minimize suture anchor failure. Because of the potentially devastating consequences of a failed repair, knowledge of each clip's performance characteristics can be invaluable in maximizing the strength of a repair.
Although we were able to demonstrate significant differences in the performance of these clips, there are several important limitations to our study. First, we compared clip performance by analyzing linear forces measured in newtons, but the clinical significance of these quantities is unknown. We also calculated the pressures generated by each clip on the tissue when a perpendicularly directed load was applied to the suture. Presumably, there is an ideal suture tension that maximizes tissue apposition and hemostatic tamponade while minimizing tissue injury and the potential for strangulation. Inside the repaired kidney is a complex mechanical environment where multiple sutures exert tangential forces that are distributed over a bolster. This makes assessment of the pressures experienced within the renal parenchyma difficult to calculate, and so the relationship between the forces measured in our study and the physiologic state of the repaired kidney remains unknown.
Second, our study used no. 1 Vicryl suture for all trials, so the performance of the clips may not be representative if used on monofilament sutures or braided sutures of smaller caliber. Another study has investigated the holding strength of Lapra-Ty clips when used with various suture types and found significant differences. 5
Third, we used fresh cadaveric human kidneys with intact renal capsules for our study. However, significant differences may exist between the characteristics of cadaveric tissue and living tissue that may make the findings of our ex-vivo study not applicable to in-vivo kidneys. In addition, the kidneys used in this study were harvested 1 day after declaration of death, but the degree and type of tissue changes in the postmortem period remain unknown. Also direct comparison trials do not exist that show the superiority of our cadaveric human kidney model over animal models in approximating the tissue characteristics of live human kidneys.
Despite these limitations, we hope to further investigate the performance of other suture anchors and broaden our current dataset with further trials. By testing various clip designs in varied combinations, we hope to better characterize the performance of a device that is becoming central to the practice of LPN.
Conclusion
Because of the technical challenges that exist in the performance of LPN, the utilization of suture anchors has become popular to minimize the need for time consuming and difficult intracorporeal knot tying. However, the safety profile of these clips has not been addressed, specifically with regard to the force needed to cause clip slippage and renal capsular violation in human kidney tissue. A single Hem-o-lok clip is more resistant to causing capsular violation, but less resistant to slippage when compared with a single Lapra-Ty clip. However, when two Hem-o-lok clips are placed in tandem, the force needed to slip off the suture exceeds that of one Lapra-Ty clip. In addition to these performance characteristics, Hem-o-lok clips also show a significant cost advantage when compared with Lapra-Ty clips. For these reasons, when compared with Lapra-Ty clips, the use of Hem-o-lok clips is a more secure and cost-effective method for anchoring sutures during LPN.
Footnotes
Disclosure Statement
No competing financial interests exist.