
Abstract
Previous studies have shown that robot-assisted microsurgical vasovasostomy (RAVV) has technical advantages over pure microscopic vasovasostomy (MVV) in animal and human models. This study presents a video technique and initial results for RAVV in 20 human cases compared with 7 MVV cases by a single fellowship-trained microsurgeon from July 2007 to June 2009. A three-layer 10-0 and 9-0 suture anastomosis was performed with up to 22 months follow-up (mean 3 months). Mean operative duration for the RAVV cases was 109 and 128 minutes for MVV (p = 0.09). At 2 months postoperatively, all patients were patent. Mean sperm count was 54 million in RAVV and 11 million in MVV (p = 0.04). The use of robotic assistance in microsurgical vasovasostomy may have potential benefit over MVV in decreasing operative duration and significantly improving early semen analysis measures. Further evaluation and longer follow-up is needed to assess its clinical potential.
Introduction
Robotic assistance during surgical procedures has been utilized in a wide array of surgical fields. 1 –5 A scalable ergonomic control system with high-definition three-dimensional viewing may provide surgeons an advantage when performing complex procedures. Microsurgical procedures can be technically challenging. Vasectomy reversal is one such procedure. A number of groups have developed robot-assisted techniques to perform vasovasostomy and vasoepididymostomy in animal and ex vivo human models. 6 –10 Some studies suggest that robot-assisted reversal may have advantages over microsurgical reversal in terms of ease of performing the procedure and improved patency rates. 9,10 Two groups have actually performed a few human robot-assisted vasovasostomies using the initial DaVinci robotic system 11 (Intuitive Surgical, Sunnyvale, CA).
Intuitive Surgical now offers an enhanced four-arm DaVinci type S robotic system with high-definition digital visual magnification that allows for greater magnification than the standard robotic system. This new system allows greater range of motion and better microsurgical instrument handling. The additional fourth arm has improved range of motion and positioning capabilities to provide the microsurgeon with one additional tool during procedures. This study presents our technique (with video) and initial results of robot-assisted microsurgical vasovasostomy (RAVV) using the new robotic platform.
Technique
Patient preparation
The patient is placed in supine position. The arms of the patient may be placed alongside (gently wrapped in the draw sheets) or apart on arm boards with adequate padding to prevent any nerve compression injuries. The scrotum was prepared and a small 1 cm vertical incision made over the previous vasectomy site after infiltration with local anesthetic (Fig. 1). The two ends of the vas were brought out of the skin incision in standard microsurgical fashion (Fig. 2).

Small 1 cm vertical incision made over the previous vasectomy site after infiltration with local anesthetic.

The two ends of the vas brought out of the skin incision in standard microsurgical fashion.
Robot positioning
The robot is used to perform the microsurgical components of the procedure as shown in Figure 3. Since this is an open case, the trocars are loaded only to allow the instruments to function and to stabilize their movements outside the patient's body. The fourth robotic arm may be placed lateral to the left robotic arm to minimize instrument clashes. The zero-degree camera lens is used for left-sided scrotal/inguinal surgery, and the 30-degree down lens is used for the right side to optimize the visual field during procedures.
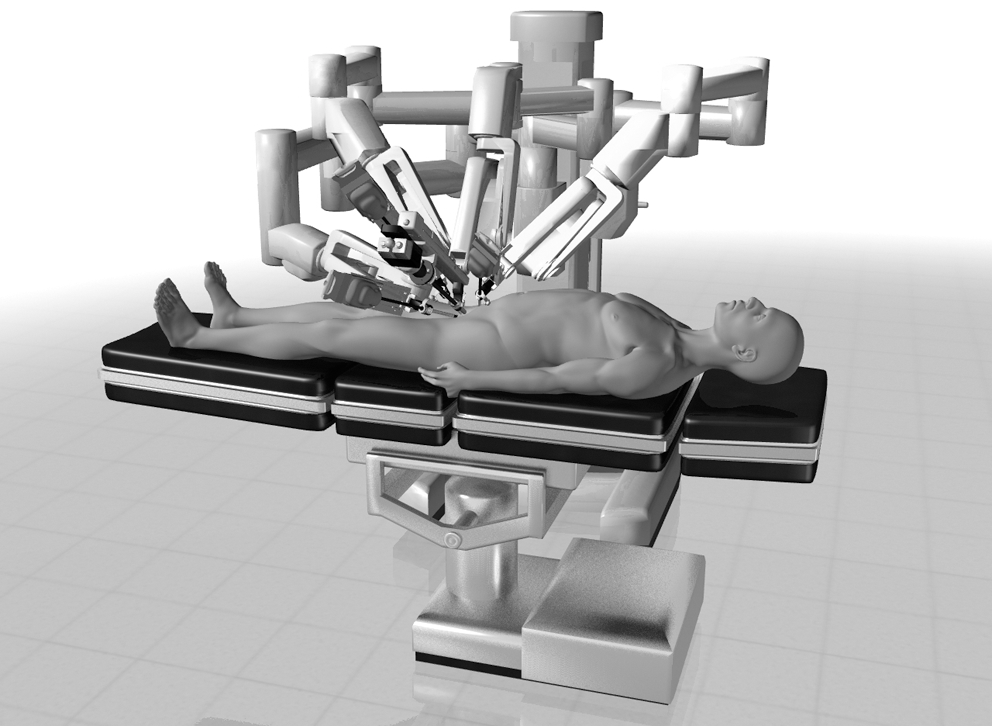
DaVinci S robotic system placement next to the patient.
Step-by-step technique
The proximal vas is carefully transected with an 11-blade scalpel, and the fluid effluxing from the lumen is collected on a glass slide and examined under phase-contrast microscopy to assess for the presence of any sperm. If there is sperm found or the efflux is copious and clear or milky, then a vasovasostomy is performed on this side.
The distal end of the vas is also transected, and the two clean ends of the vas are now approximated to each other to allow a tension-free anastomosis. Small hemostats are placed on the adventitia next to each end of the vas to avoid any direct manipulation of the vas. The same procedure is performed on the contralateral scrotal side. The robot is now positioned to perform the microsurgical vasovasostomy as described in the robot positioning section above.
The left side vasovasostomy is performed first. The black diamond microforceps are loaded on the right and left surgical robot arms. The zero-degree camera lens is loaded onto the robot camera arm. The micro Potts scissors are loaded onto the fourth robot arm. The two vas ends are placed over a 1/4″ Penrose drain. The assistant now irrigates the field with saline using a 10 cc syringe with an 18-gauge angiocatheter tip. Weck sponge sticks are used to dry the field. Each of the lumen of the vas is dilated with the black diamond forceps.
A 9-0 nylon suture is used to approximate the posterior muscularis layer of the two ends of the vas. The surgeon uses the black diamond forceps in both left and right arms as needle drivers. The fourth arm is used by toggling the surgeons left arm to use the micro Potts scissors whenever suture needs to be cut.
Two or three double-armed 10-0 nylon sutures are now placed to reanastomose the posterior mucosal lumen of the vas. The sutures are placed inside out to ensure good mucosal approximation. All sutures are placed before they are tied (Fig. 4).
Three double-armed 10-0 nylon sutures are used to close the anterior mucosal lumen of the vas (Fig. 5).
Five to six 9-0 nylon sutures are used to approximate the muscularis layer of the vas (Fig. 6).
The adventitia is approximated using a 6-0 prolene suture to relieve any tension in the anastomosis and to wrap the repair site.
The same procedure is now performed on the contralateral right side by repositioning the robot away from the patient to the right scrotum. The camera lens is changed to 30 degrees down to allow a better angle of visualization of the anastomosis. The robotic vasovasostomy is performed on the right side as previously described.
The dartos layer is closed using a running 3-0 chromic suture for both scrotal skin incisions. The skin is closed using a 4-0 chromic running suture. Fluff dressings with an athletic support are applied.
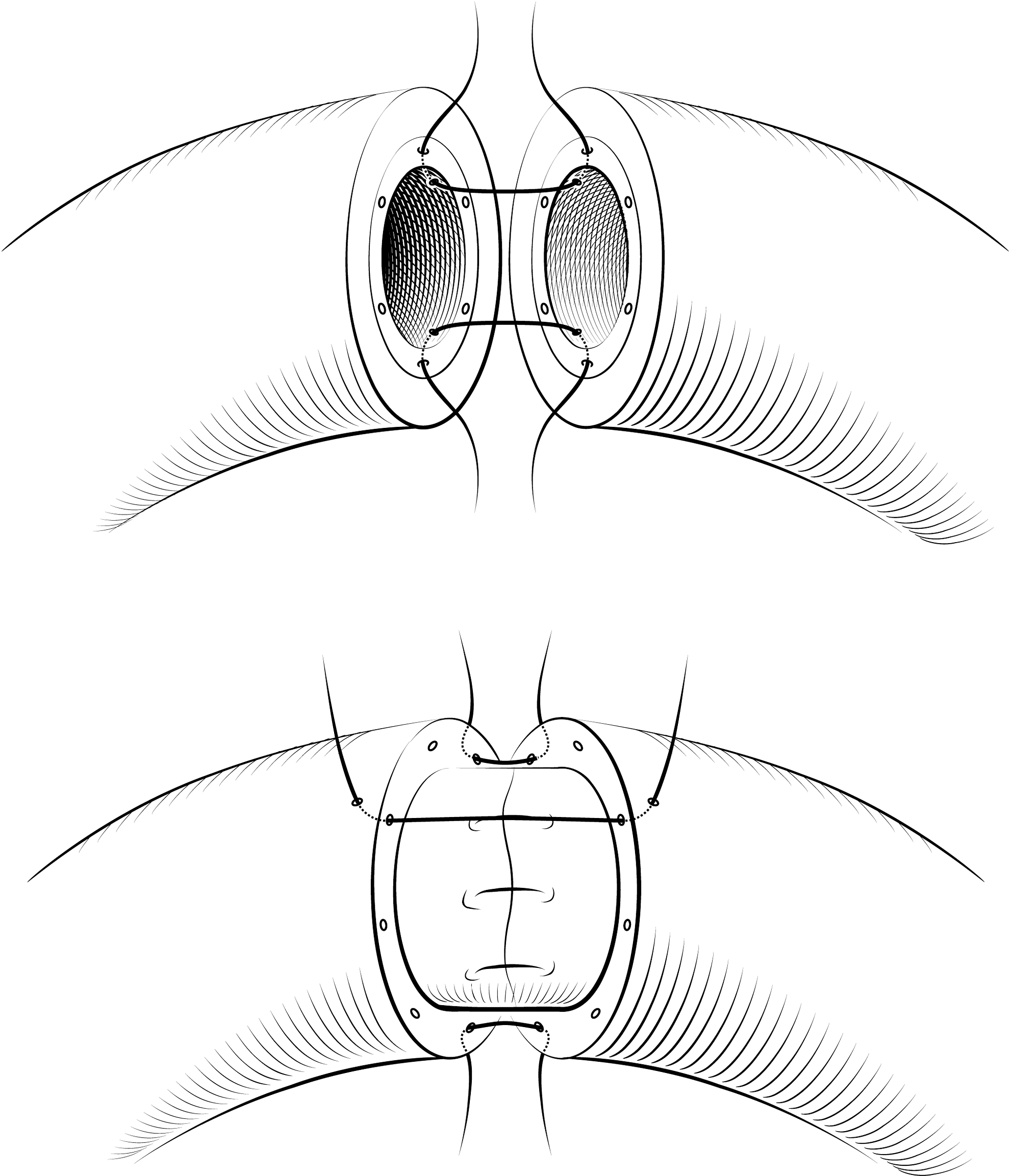
Robot-assisted vasovasostomy technique.
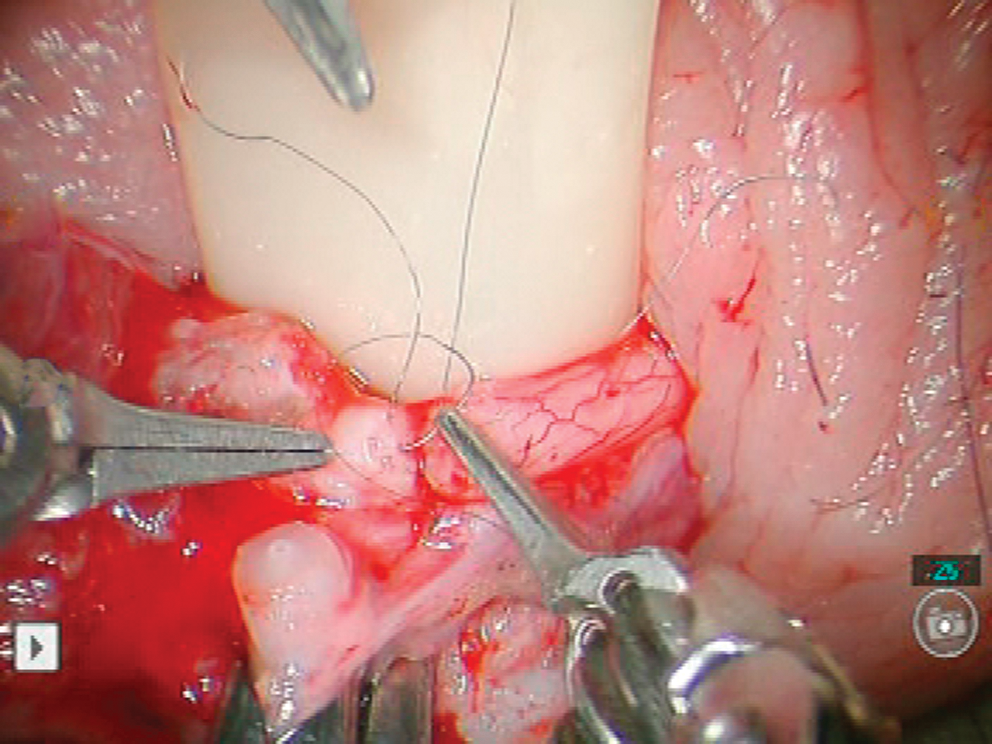
Placement of posterior 10-0 nylon sutures in the mucosal lumen of the vas.
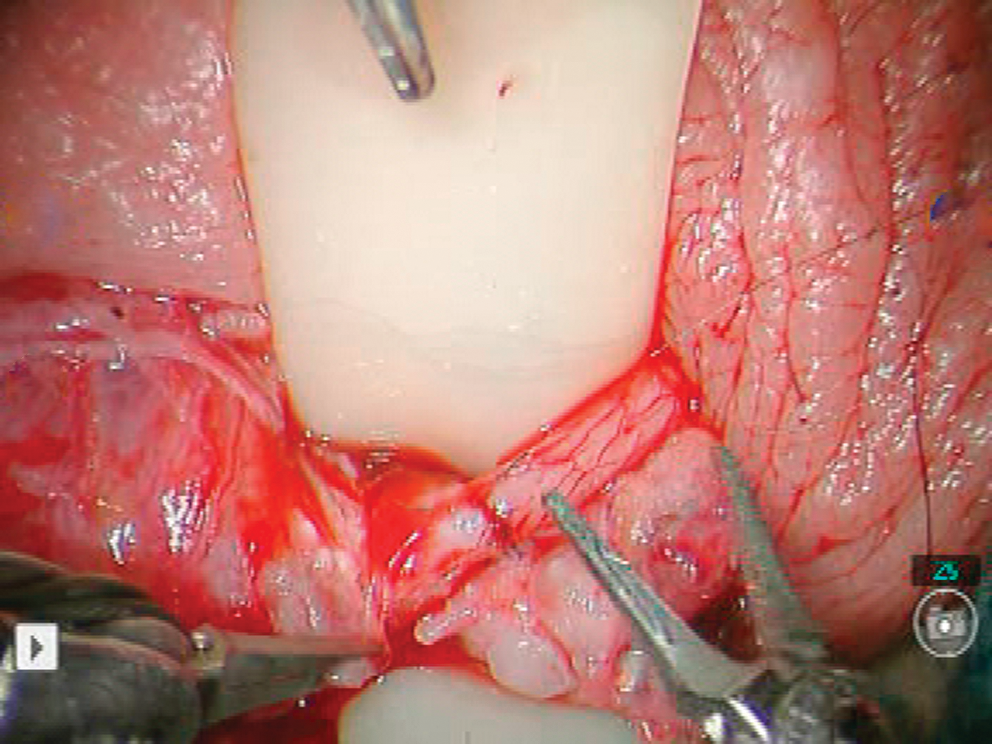
Placement of 9-0 nylon sutures to anastomose the muscularis layer of the vas.
The video accompanying this article presents the complete operative technique. A step-by-step operative image guide of our technique is also available at
Instruments
Ophthalmic hand-held microcautery is used for the dissection and release of the proximal and distal ends of the vas during the preparation portion of the surgery. During the robotic microsurgical portion, the black diamond microforceps are utilized for the left and right arms. The micro Potts scissors is used in the robotic fourth arm. The assistant irrigates the surgical site with saline during the case using a 10 cc syringe via an 18-gauge angiocatheter. The assistant also may dry the field using micro Weck sponge sticks. The assistant brings all sutures in their foam holders to the edge of the field so that the surgeon may grasp the sutures and cut them as desired to minimize any suture needle loss during the case.
Role in Urologic Practice
Twenty bilateral RAVV cases were performed from July 2007 to June 2009 by a single fellowship-trained microsurgeon (S.J.P.). These procedures were compared with seven microscopic vasovasostomy (MVV) cases performed by the same surgeon during the identical time period. Selection of approach (RAVV vs. MVV) was based on patient's choice after thorough discussion of options (the cost premium for RAVV was $3100 above MVV). A three-layer 10-0 and 9-0 suture anastomosis was performed with up to 22 months follow-up (mean 3 months). Mean duration of obstruction (time from vasectomy) was 9 years (range 1–19 years) for RAVV and 7 years (range 3–9 years) for MVV. Mean age of the patients was 43 (range 32–59) for RAVV and 34 (range 30–40) for MVV. Mean operative duration for the bilateral cases was 109 minutes (65–180 minutes) for RAVV and 128 minutes (105–150 minutes) for MVV (p = 0.09). None of the cases required delivery of the testicle. All cases were performed under general anesthesia. At 2 months postoperatively, all patients were patent. Mean sperm count was 54 million sperms in RAVV and 11 million in MVV (p = 0.04).
For RAVV, operative duration, number of suture breaks, and number of needle bending decreased with increasing surgeon experience. Operative duration started at 150 to 180 minutes initially and then dropped to about 65 to 120 minutes after nine cases. Suture breakage and needle bending reduced significantly and rarely occurred after 13 cases. During RAVV, there is a lack of haptic feedback, thus forcing the surgeon to rely heavily on visual cues. The enhanced type S high-definition DaVinci™ robotic platform (Intuitive Surgical, Sunnyvale, CA) allows for improved range of motion and enhanced digital magnification (up to 15–20×). This helps minimize the deficit in haptic feedback by enhancing visual acuity and instrument handling. However, there still is a learning curve associated with RAVV. Subjectively there appeared to be ergonomic and suture placement accuracy advantages to using the robotic system over the microscopic platform. There was an additional 30 minutes to 1 hour to prepare the robot at the beginning of the case—this time significantly decreased with experience as the operating room staff became more familiar with our setup (the last case was prepped in 20 minutes). Thus, there is a significantly increased time investment for robotic reversal initially. This was also found to be the case by Kuang et al. 7 However, Schiff et al 9 found that the robotic platform cut down operative times in an animal model. Based on our learning curves generated in this study, it is conceivable that the operative times should decrease compared with microsurgical series as the surgeon gains experience over more cases. The mean operative duration for RAVV (109 minutes) was decreased compared with MVV (128 minutes) in our study. However, this was not statistically significant.
Patency rates can be as high as 97% in traditional microsurgical vasovasostomy (MVV) patients who are less than 3 years out from their vasectomy. 12 Our RAVV patient series included several men who were many years out from their vasectomy (10 men >10 years out, 2 men >18 years out). Previous studies have illustrated that the success rate with microsurgical reversal for these patient could be in the 71% range or less. 12 At the 2 month follow-up point, all these patients are now patent (100%). Our sample size is small, but it is promising that the robotic technique faired well in this patient population. Usually sperm can be seen in the ejaculate within weeks after vasovasostomy. Ninety-five percent (19/20) of the patients have had large amounts (>1.8 million/mL) of motile sperm in their ejaculate within weeks after surgery.
The use of robotic assistance in microsurgical vasovasostomy may have potential benefit over MVV with regards to decreasing operative duration and significantly improving early semen analysis measures. Further evaluation and longer follow-up is needed to assess its clinical potential.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
*
A video demonstrating this technique is available online at