
Abstract
Background and Purpose:
Percutaneous nephrolithotomy (PNL) is a first-line management technique for staghorn stones and stones located in a horseshoe kidney (HK). We present our multi-institutional experience on the management of staghorn calculi within HKs.
Materials and Methods:
The study included 15 patients with 17 staghorn calculi in HKs who were treated by PNL in six academic institutions. All PNL procedures were performed in a standard one-session technique with fluoroscopic guidance. The following information was assessed: Number of access dilations, renal access location, blood loss, blood transfusion, stone-free rate, length of hospitalization. Intraoperative and postoperative complications as well as secondary procedures (second-look PNL, ureteroscopy, and shockwave lithotripsy) were reviewed.
Results:
Mean patient age was 50 years (range 24–72 y) years old. Subcostal (n = 16) or intercostal (n = 1) puncture was performed. The average anesthesia time was 126 minutes (93–200 min). The average blood loss was 450 mL, and transfusions were deemed necessary in 20% of the cases. Single skin incisions were made for the management of 11 renal units, and multiple incisions were made in 6. The average number of tract dilations per renal unit was 2.11 (range 1–4). The overall stone-free rate was 82%. The average length of hospital stay was 4.4 days (range 3–7). The average duration of nephrostomy tube drainage was 80 hours with a range of 72 to 96 hours. Major and minor complication rate was 20% and 46.6%, respectively.
Conclusion:
The performance of PNL is a safe and effective method to manage staghorn calculi in HKs.
Introduction
Horseshoe kidney (HK) is one of the most common congenital anomalies and is considered to be the result of incomplete cephalad migration and malrotation of the kidney during early gestation, due to the entrapment of the isthmus under the inferior mesenteric artery. 1,2 The higher insertion of the ureter into a typically elongated renal pelvis resulting in a deformed ureteropelvic junction is responsible for hydronephrosis, urinary stasis, and urolithiasis that 60% to 70% of patients present. 1 Thus, the management of HK urolithiasis presents particular challenges.
Staghorn calculi are defined as large stones that occupy at least the renal pelvis and two calices. Conservative management of staghorn stones carries a high risk of renal loss and a mortality rate of approximately 30%. 3,4 A significant factor for renal failure in cases of staghorn calculi is the presence of infection or obstruction. The ideal management of staghorn calculi includes a complete surgical removal of the entire stone burden, the treatment of any metabolic abnormalities and the management of anatomic variations contributing to stasis within the urinary tract. Proposed methods for the management of staghorn stones are extracorporeal shockwave lithotripsy (SWL), percutaneous nephrolithotomy (PNL), and open stone surgery (OSS). 5
The management of staghorn stones in the HK represents a challenge for the urologist because of the abnormal anatomy of the HK and the high stone burden. In the current study, we retrospectively report multi-institutional experience with the management by PNL of staghorn stones in patients with HKs.
Materials and Methods
We retrospectively evaluated 15 charts of patients who were treated with PNL for the management of 17 staghorn calculi in HKs. The data were obtained from six academic institutions. A staghorn calculus was defined as a calculus that filled at least the renal pelvis and two calices. The following information was accessed: Number of access tracts-dilations, renal access location, blood loss, blood transfusion, stone-free rate, and length of hospitalization. Moreover, additional intraoperative or secondary procedures for stone clearance were reviewed. Intraoperative and postoperative complications as well as the need for secondary interventions to address these complications were also reviewed. Clavien system classification of complications was performed. 6,7
Patients were either asymptomatic (n = 4) or manifested symptoms (n = 11) such as flank pain, urinary infection, and hydronephrosis. All patients were preoperatively evaluated with radiography of the kidneys, ureters, and bladder. Preoperative intravenous urography (IVU) was performed in six patients, and in the remaining patients, preoperative CT was performed. Biochemical and hematologic profiles of the patients were also included in the preoperative evaluation. Complete urinalysis and culture were performed before and after treatment.
Administration of antibiotics started 1 week before the PNL and continued for 1 week postoperatively. The administration of antibiotics took place in an attempt to avoid septic complications related to the staghorn stones. The antibiotic scheme was administered in all cases according to the results of the urine culture. Preoperative nephrostomy tubes were inserted with the patient under deep sedation. All PNL procedures were performed under general anesthesia.
Technique of PNL
An open-ended 6F ureteral catheter was advanced in a retrograde fashion into the renal pelvis, allowing the injection of contrast material to opacify the collecting system when necessary. The collecting system was visualized with the use of biplanar C-arm fluoroscopy. The patient was then placed in the prone position, and foam bolsters were placed bilaterally from the shoulders to the iliac crest to assist ventilation.
The following techniques were used according to the preference of the surgeon: The angular (single incision) access has been described previously in detail.
8
The angular puncture technique does not necessitate an intercostal approach and enables the performance of multiple punctures in all calices by the same incision. Single puncture and combined use of rigid and flexible nephroscopy with a laser lithotripter was also used. For the multiple tracts approach, direct puncture into the calix bearing the stone was preferred. Flexible nephroscopy was also used in all of the above techniques when deemed necessary to achieve stone clearance. Supracostal or subcostal access was selected according to the individual anatomic features of the patient and the preference of the urologist.
With the help of fluoroscopy, an 18-gauge needle was inserted to the desired calix; a guidewire was inserted. If the stone size allowed, a second safety wire was also placed. The dilation of the tract took place with the use of an Amplatz or balloon dilating system. The nephroscope was used through a low-pressure system with an Amplatz working sheath. Additional punctures and accesses were performed according to the preference of the surgeon and the technique used (Fig. 1). Rigid nephroscopy with the aid of an ultrasonic lithotripter and/or flexible nephroscopy with the aid of a laser lithotripter were performed to achieve stone clearance (Fig. 2). The small stone fragments were removed with either graspers or a stone basket.
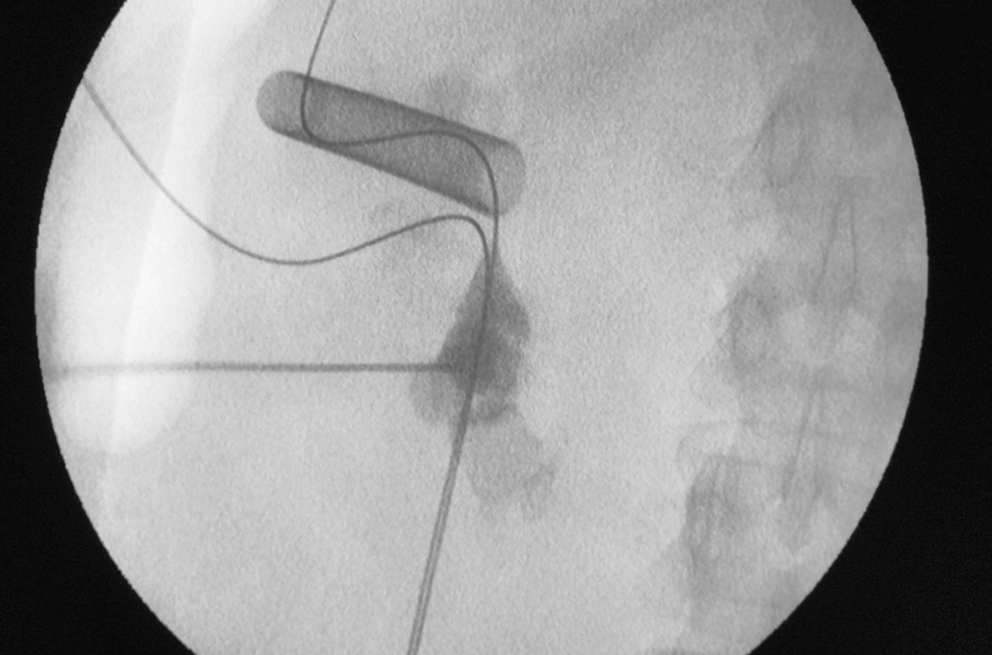
An additional puncture of the lower calix is performed. Note the previously installed guidewires and access sheath.
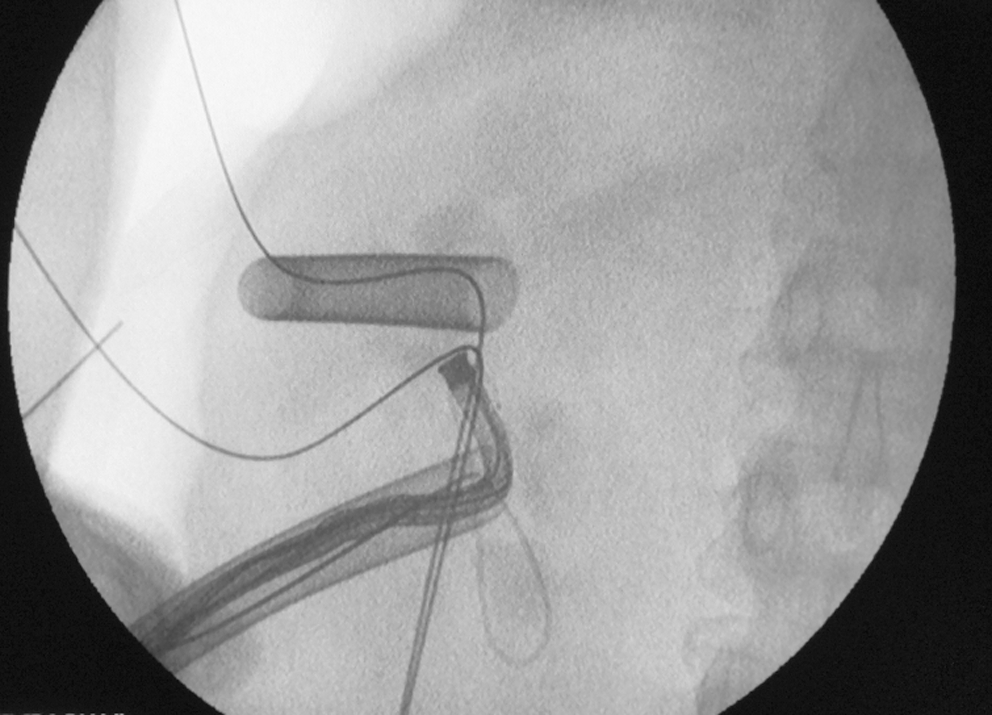
Flexible nephroscope is used through the lower access sheath to achieve stone clearance.
On completion of the procedure, a 24F reentry Malecot nephrostomy tube (Boston Scientific, Natick, MA) or nephrostomy catheter and double pigtail were inserted. The above maneuvers provided continuous drainage, tamponaded bleeding from the freshly dilated nephrostomy tracts, and/or maintained access to the collecting system for further manipulations. The insertion of both nephrostomy and double pigtail stent was performed for individual anatomic reasons. Tubeless PNL was not performed.
Antegrade pyelography was performed on the third or fourth postoperative day, and if there was no extravasation and contrast passed freely into the bladder, the tube was then removed. Stone clearance was documented by either postoperative nephrostomography (n = 3) or noncontrast spiral CT (n = 12).
Results
The results are shown in Table 1. Among the 15 patients with staghorn calculi reviewed, 2 patients had complete staghorn calculi extending in the pelvis and all the calices. Two patients had bilateral staghorn stones, for a total number of 17 renal units managed. Single incision and performance of angular tracts using the Amplatz dilator system were performed in 11 renal units (10 patients, group A). Six renal units (five patients) were managed by two or three incisions and respective number of tracts (group B). One of the five patients who were treated by multiple tracts PNL needed intercostals access (between the 11th and 12th ribs). Group C included two patients (two renal units) who underwent single puncture technique with combined use of rigid and flexible laser lithotripsy. Table 2 demonstrates the technical details of the performed procedures. All attempts were made for complete stone clearance.
Results of Management of Staghorn Calculi in Horseshoe Kidney
Technical Details of the Performed Procedures
Blood transfusion was necessary in 20% of patients, and the average transfusion was 1.5 units. A combination of rigid and flexible nephroscopy was used to achieve stone clearance in the two patients of group C and the additional two patients of group A as well as two patients of group B. Intraoperative additional procedures were necessary in two patients who underwent endopyelotomy (one procedure in each patient). One of the patients belonged to group A and one to group B. The overall stone-free rate achieved was 82% (14 of 17 patients). Stone clearance rates for groups A, B, C were 77.7%, 83.3% and 100%, respectively. Two patients underwent bilateral PNL simultaneously. One patient was treated by angular and the other by multiple accesses.
The major complication rate was 20%, including three cases of diffuse bleeding necessitating transfusion (3/15, Clavien grade II). Minor complications included urinary tract infection in 26.6% (4/15, grade II), fever of unknown etiology 24 hours postoperatively in 6.6% (1/15, grade I), and persistent leakage of urine in 13.3% of patients (2/15, grade IIIa). Urinary tract infections were managed by antibiotics while fever by antipyretics. One patient also reported stent discomfort (grade I) and was treated with analgesics. The two cases of prolonged urinary leakage were addressed by secondary double pigtail stent placement for 2 weeks. The leakage subsided after stent placement, and no complication occurred after removal of the stent. The remaining complications were managed conservatively without any renal unit loss or mortality.
A secondary procedure for stone clearance was necessary in three patients. All procedures took place 1 to 2 weeks after discharge. One patient (group A) needed retrograde ureteroscopy for a stone fragment that migrated down the ureter without causing obstruction. Residual stone fragments were managed successfully by SWL in two patients (one patient in group A and one in group B). Table 3 summarizes the results for each group of patients who were included in the study.
Comparison Between the Approaches Used for the Management of Staghorn Calculi in Horseshoe Kidney
SWL = shockwave lithotripsy; URS = ureteroscopy; DJ = double pigtail.
Discussion
The guidelines of the American Urological Association and the European Association of Urology on the management of large/staghorn stones propose the use of PNL followed by SWL (if necessary) as the preferred method. 5,9 Nevertheless, there have been limited reports of the percutaneous management of staghorn calculi in HK. 10 –12
An approach to the dorsal or dorsolateral aspect of the HK should be performed because of the abnormal blood supply. Moreover, the collecting system is abnormally low and centrally oriented. HK is also related to retrorenal colon. 13,14 The posterior and lateral orientation of the upper poles provides a safe direct puncture route that should be preferred for the management of larger, complex stones. Nevertheless, the lower poles are seldom suitable for puncture because they lie within a medially pointing coronal plane. 15 The approach is performed below the 12th rib on the posterior axillary line with caudad angle of puncture. 13 Flexible nephroscopy or multiple accesses are helpful in overcoming the length of the more anteriorly located renal pelvis tract and to provide access to lower medial calices. 1,15,16
Limited evidence on PNL management of staghorn calculi in HKs is present in the literature. Most of the series report the management of large stones in HK and include very limited numbers of staghorn stones. 10 –12 Shokeir and associates 11 achieved the clearance of large stones (three staghorn) by rigid nephroscopy in 82% of the patients with HKs at discharge day. The complications rate was 13.3%. In 82% of the cases a single tract approach was used. Raj and colleagues 10 managed three staghorn calculi in a series of 37 cases of HK lithiasis. The stone-free rate of 87% was reported for the patient population. The majority of the procedures were performed by a single access, and both rigid and flexible nephroscopes were used. Mosavi-Bahar and coworkers 12 reported the management of two staghorn stones in HKs. The patients needed additional SWL for the complete clearance of the stones and multiple access tracts.
Symons and associates 17 performed PNL in six patients with staghorn calculi in HKs. Two patients were rendered stone free in one session. Two patients needed two sessions of PNL, one patient three stages of PNL, and the remaining patients four stages. Ureteroscopy was not performed. Upper-pole access was used in approximately half of the cases, while a multitract approach for the remaining cases was deemed necessary. Major and minor complications rates for the total population of patients were 3% and 15%, respectively. Miller and colleagues 16 managed stones of an average diameter of 2.59 cm in 35 patients with HKs with a primary stone-free rate of 84.1%. A single percutaneous access was performed in 97.7% of the cases, while the majority of the kidneys were accessed by the upper pole (82.2%). The overall complication rate was 14.3%.
Recently, Gupta and coworkers 18 presented an extensive single-institution experience on PNL that was performed in abnormal kidneys. A total of 31 patients with HKs were treated by PNL. The stone size ranged between 1 and 5 cm. Thus, staghorn stones were also treated. Tubeless PNL took place in five cases; complications included a case of sepsis. Blood transfusion was deemed necessary in two patients. The authors observed that the medial tracts are more difficult to be dilated, and the tracts are usually longer. Colonic injury related to the HK was avoided by performing the puncture more medially, because the colon has a more posterolateral relationship to the kidney.
The current study presents probably the largest series of PNL procedures performed for the management of staghorn stones in HKs. In addition, we present a multi-institutional experience with the use of various techniques of PNL to address the above condition. The stone-free rate of the primary PNL procedure in our series was 82%, which is comparable to other series of large stones in HKs (range 81%–87%). 10 –12 The low number of patients included in each group of the current study does not allow us to draw any solid conclusions on the efficacy of each method in the management of staghorn stones in HKs. Moreover, we do not attempt to compare the presented groups, because any comparison would not have been reliable.
Subcostal upper-pole access was used in all cases except for one (one renal unit), which needed intercostal access through the 11th and 12th rib. The former approach was feasible in the majority of cases because of the lower position of the HK. Previous studies of the management of large stones in HKs report the requirement of an unusually long tract for approaching the medial and lower calices. 10 The flexible nephroscope is longer and could be used to overcome the latter problem. Moreover, the flexible nephroscope provides better maneuverability to address the high stone burden in medial and lower calices. The upper pole access in HK facilitates the entry of the instrument in all anatomic sites of the collecting system. 10
The selection of the number of tracts for access regardless of the kidney anatomy and stone size represents a point of debate in the literature. In a previous study, we proposed angular access for stone removal in normal kidneys. Single incisions were performed for the approach to upper, medial, and lower calices of the kidney. The subcostal triangulation technique achieved an 85% stone-free rate in one session. Excessive bleeding was observed in one case. 8 The use of an angular approach in HKs with staghorn stones proved to be effective in the current study. Auge and colleagues 19 reported similar complications for both single and multiple tract access in the management of complex stones. Multiple tract access was associated with a higher transfusion rate. Hegarty and Desai 20 prospectively compared the two approaches and observed similar complication rates. The multiple tracts method was proposed as a highly effective method for the management of high burden cases as well as staghorn calculi.
The management of staghorn calculi by multiple accesses has been reported to achieve 84% clearance, and the majority of the cases needed three to four access tracts. 21 Stone clearance in 85% of the staghorn calculi cases was also reported to be feasible with the use of a single-tract technique. 22 Netto and associates 23 achieved 80% to 87.5% stone-free rates for the single-tract technique, depending on the punctured calix. The upper calix puncture was more effective for stone clearance. The multiple tracts approach managed 84.8% of the cases. The incidence of transfusion was higher with the multiple-tract approach. Recently, multiple access tracts were reported to achieve a stone clearance rate of 70.7% and 89% for single session and second look procedures, respectively. Complications were encountered in 67 of 149 cases. 24
A single incision technique was feasible in 10 cases (11 renal units) of the current study; two to three incisions were performed in the remaining cases according to the number of punctures deemed necessary (Table 2). The cosmetic outcome is superior in the cases of angular approach. Multiple tract (group B) and angular access were associated with similar transfusion rates and higher complication rates in comparison with group C. Group C included only two patients, and the current results do not represent the technique accurately. A previous study on angular percutaneous access reported increased bleeding and a transfusion rate of 45%. 8 Comparative studies between single and multiple tract access are related to high frequency of transfusion in the case of the multiple tract approach. 19,20,23 Hospitalization time was observed to be higher in group B. Nevertheless, larger comparative series are necessary to draw scientifically sound conclusions.
Complication rates similar to those of the current study have been published by other investigators in cases of large stones in HKs. 10,11 Major complications were observed in 20% of the cases of the current series, and all patients were treated conservatively. We did not observe any colonic injury, which may happen because of the retrorenal position of the colon in some patients. The preoperative CT scan evaluation was helpful in distinguishing these cases, but it was not routinely performed by all participating centers. Minor complications were conservatively managed in all cases. The cases of persistent urine leakage after nephrostomy removal were addressed with double-pigtail insertion. The latter cases were associated with Malecot tubes inserted at the end of the procedure. The remaining minor complications were managed conservatively. The administration of antibiotics 1 week before PNL, especially in the case of large/staghorn stones, has been shown to minimize septic complications. 25,26 The current experience confirmed the effectiveness of the above antibiotic scheme.
The limitation of the presented series is the retrospective and multi-institutional nature of the study, which introduces biases in data collection. Although the current patient population is probably one of the largest studied so far, it is still limited and does not document adequately the outcome of PNL in the management of staghorn calculi in HKs. Nevertheless, the feasibility and successful outcome of the various methods in the management of the aforementioned lithiasis cases was proven. Further prospective clinical studies with larger patient populations are necessary for confirmation of the current results.
Footnotes
Disclosure Statement
No competing financial interests exist.