
Abstract
Purpose:
The goal of this study is to demonstrate the feasibility of transurethral radical prostatectomy in the canine model. We describe the surgical procedure for natural orifice translumenal endoscopic surgery-radical prostatectomy (NOTES-RP).
Materials and Methods:
NOTES-RP was performed on six nonsurvival male canines. The 100 watt holmium:yttrium-aluminum-garne laser, 550 μm end-firing fiber, 28F laser resectoscope, 7F stabilizing catheter, and continuous irrigation were used to radically resect the prostate. A Vest vesicourethral anastomosis was performed using a laparoscopic suture device that was delivered through the nephroscope. In the initial cases, the prostate was removed manually; for the last two cases, the prostate was removed endoscopically with a tissue morcellator.
Results:
NOTES-RP was successfully executed in all canines. Visualization was not obscured by bleeding. Dissection times ranged from 40 to 120 minutes. Fluid absorption was problematic in cases lasting more than 1 hour, because of the intraperitoneal location of the canine prostate and bladder.
Conclusions:
The feasibility and technique of NOTES-RP was successfully demonstrated in the living canine model.
Introduction
Recently, our group reported the feasibility of NOTES-radical prostatectomy (NOTES-RP) in the human cadaver. 15 Using the holmium:yttrium-aluminum-garnet (YAG) laser and a laser resectoscope, as used for holmium laser enucleation of the prostates (HoLEP), we radically resected the prostate transurethrally with apparent preservation of the sphincter and neurovascular bundles. While the goal of our previous study was to develop the surgical technique, we were unable to assess hemostasis and the impact of bleeding on endoscopic visualization. Furthermore, although normal saline irrigant is used for the procedure, it is unclear how fluid absorption by living tissue would affect the procedure. The goal of the current study was to assess the feasibility of NOTES-RP in the living canine model.
Materials and Methods
After institutional animal ethics committee approval, the procedure was performed on six male hounds. All animals were adults; however, exact age was unknown. The weight of the animals varied from 50 to 70 pounds. The procedure for each canine was carried out in similar fashion. Anesthetic agents used in all cases were sodium thiopental 2.5% at a dose of 2 to 20 mg/kg administered intravenously and Isoflurane
Equipment used consisted of: 100 watt holmium:YAG laser (Verapulse; Lumenis Inc, Santa Clara, CA), 550 μm end-firing quartz laser fiber (Slimline; Boston Scientific Corp, Natick, MA), continuous-flow 28F resectoscope with laser bridge, 7F laser stabilizing catheter (Cook Medical Inc, Bloomington, IN), saline irrigation, rigid offset 27F nephroscope with 5-mm working channel, and tissue morcellator (Lumenis Inc, Santa Clara, CA). The vesicourethral anastomosis was performed in one animal using a nitinol basket and SR-5LS Sew Right
After induction of general anesthesia, the canine was positioned supine, and a perineal urethrostomy was performed (Fig. 1). The anterior urethra was dilated to 30F using van Buren sounds or Otis urethrotome, depending on urethral size. A 28F continuous-flow resectoscope sheath was placed into the bladder, followed by the laser bridge, stabilizing catheter and fiber. Continuous gravity inflow and outflow of normal saline irrigation was used. The holmium laser was set at our standard HoLEP settings of 2 J and 40 Hz for the majority of the dissection, but it was decreased to 2 J and 20 Hz at the level of the verumontanum near the sphincter to limit energy-related injury to the external sphincter.

Perineal urethrostomy was performed in each canine to facilitate insertion of the 27F resectoscope.
After the ureteral orifices and sphincter were visualized, a 7 o'clock incision was made lateral to the verumontanum. The incision was carried through the transition zone, peripheral zone, and prostatic capsule into the periprostatic tissue. The resection was then carried circumferentially to the 5 o'clock position after ensuring position outside the prostate capsule. Position was confirmed by visualization of the periprostatic fat, reinforcing all prostatic tissue was excised.
Dissection was next carried toward the bladder neck anterior to the prostate but below the level of the dorsal venous complex. At this point, the apical dissection was complete except at the verumontanum bridge from the 5 to 7 o'clock position. The bridge was then divided and the plane posterior to the prostate above the rectum was developed.
Next, the neurovascular bundles were dissected away from the prostate. The magnification of the resectoscope allowed for identification of individual vessels, and the holmium laser achieved precise hemostasis (Fig. 2). After the posterolateral pedicles were controlled bilaterally, the scope was repositioned inside the prostatic urethra, and a bladder neck incision was made at the 12 o'clock position. The prostatic bladder neck attachments were severed circumferentially until the only remaining connection was the seminal vesicles and vas deferens. Using the scope beak, the prostate was then displaced anteriorly toward the bladder in the prostatic fossa. The seminal vesicles and the vas deferens were amputated bilaterally, completely freeing the prostate.
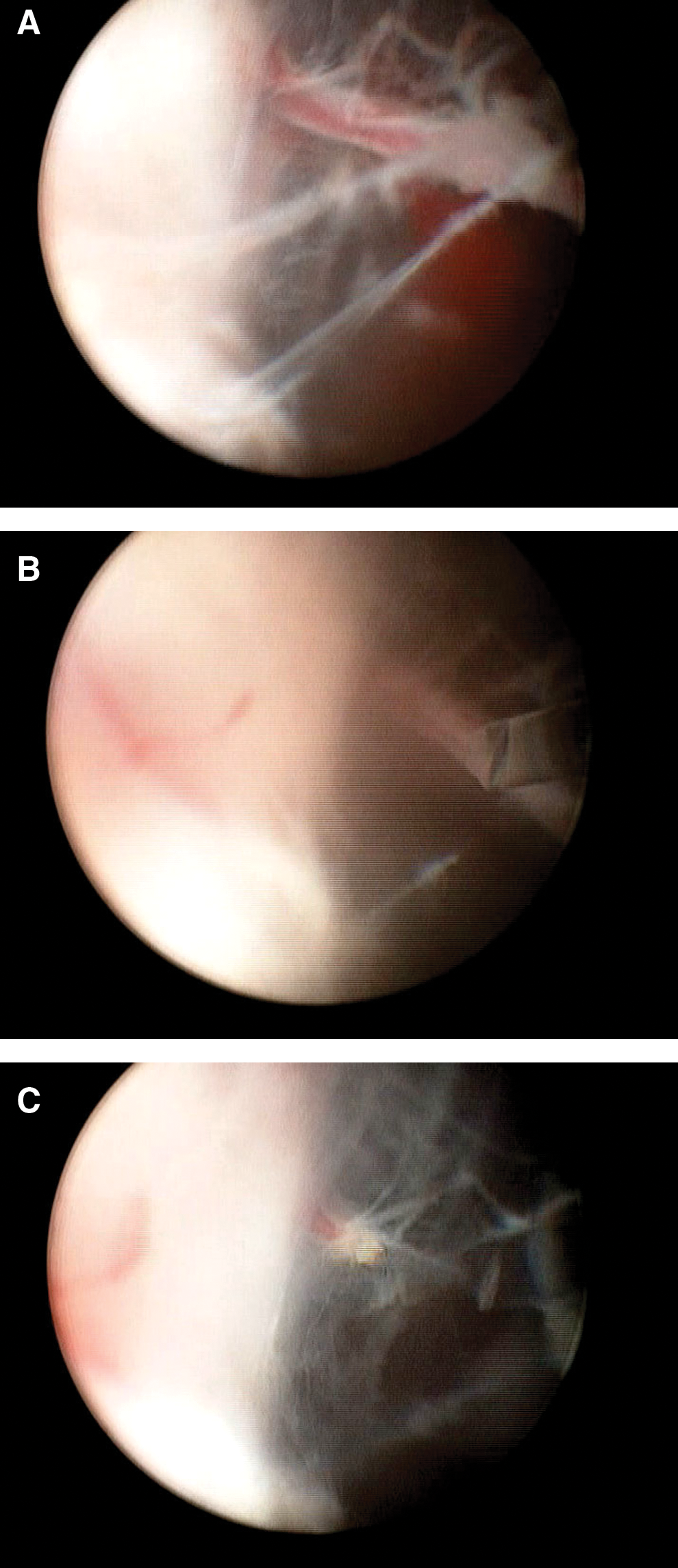
The holmium:yttrium-aluminum-garnet laser can perform pinpoint, exact hemostatis of individual prostatic pedicle vessels. The left lateral pedicle vessel attached to the prostate is visualized (
To define the best specimen retrieval method, several approaches to tissue removal were used. The abdomen was opened and the prostate retrieved manually in the initial four canines (Fig. 3). In the subsequent two canines, the prostate was morcellated with a tissue morcellator, as described for HoLEP. 16 Despite attempts using several different techniques, the vesicourethral anastomosis was performed successfully in only one canine using perineal Vest sutures. Using a 27F nephroscope and the SR-5LS device, a 2-0 poliglecaprone suture was placed through the bladder neck at the 3 o'clock position. A stab incision was made in the perineum to allow passage of sequential fascial dilators under fluoroscopic monitoring to create a 10F tract.
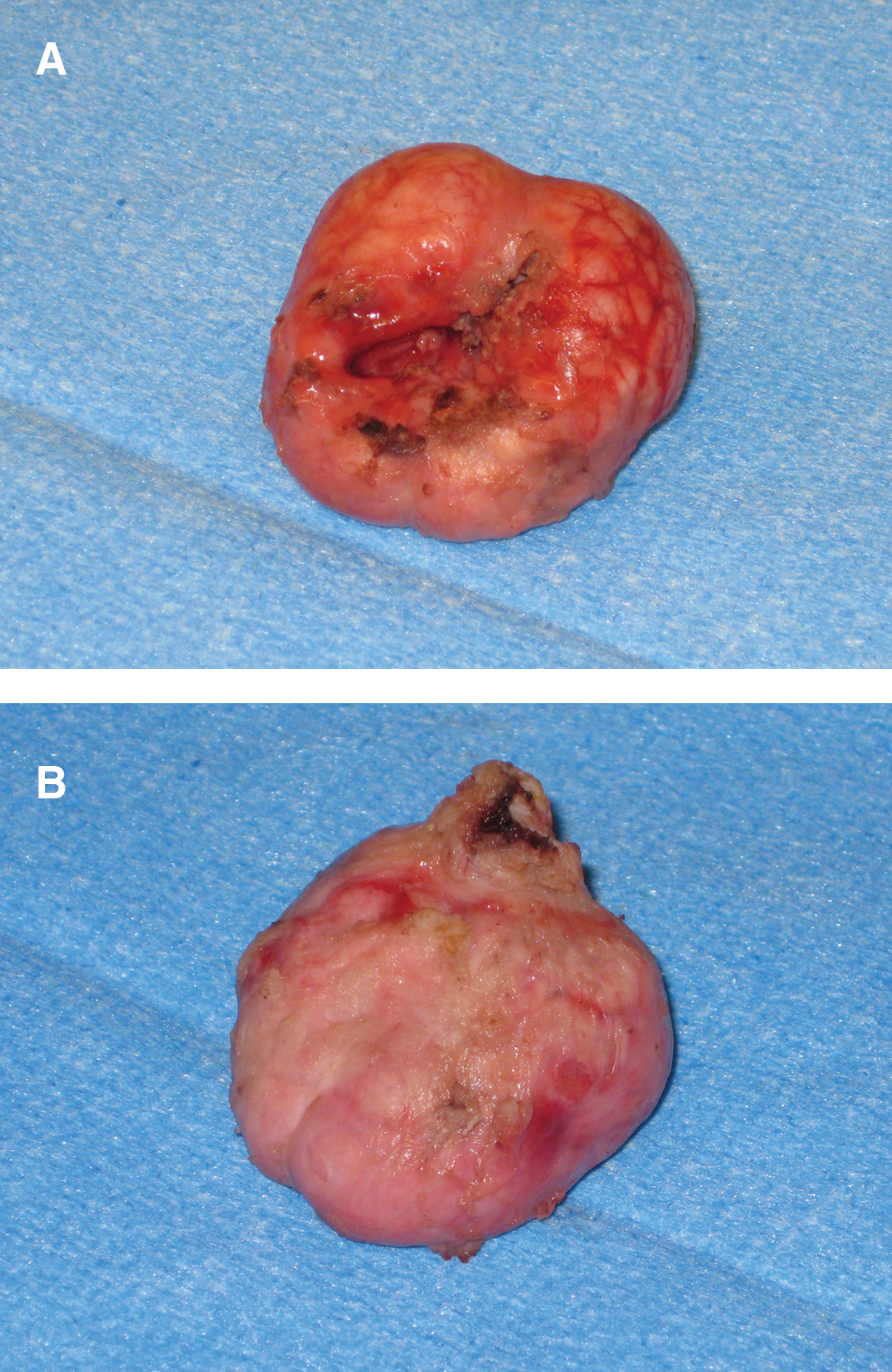
Anterior (
With the nephroscope in the urethra, the last dilator, the 10F dilator, was visualized endoscopically in the prostatic bed and a 2.2F nitinol basket passed through the dilator. Using the grasping forceps passed through the nephroscope, the poliglecaprone suture placed at the 3 o'clock bladder neck position was stabilized that it could be snared by the basket and pulled through the perineum. The procedure was then repeated on the opposite side and the 9 o'clock bladder neck position. All animals were killed at the completion of the procedure.
Results
The canines weighed between 50 and 70 pounds. NOTES-RP was successfully performed in all animals. Bleeding was controlled in all cases using the holmium laser, and estimated blood loss for each animal was ≤50 mL (excluding perineal urethrostomy). All animals were hemodynamically stable throughout the procedure. Operative times ranged from 45 to 120 minutes. In the first four cases, more than 1 hour in length, significant abdominal distention occurred, limiting mechanical ventilation. The intra-abdominal location of the dog bladder and prostate resulted in significant fluid displacement into the peritoneal cavity. To complete the procedure, a small 3 to 5 cm abdominal skin incision was made for fluid evacuation using a disposable wall suction in those four cases.
The intra-abdominal location of the canine prostate also hampered our ability to perform an ideal vesicourethral anastomosis because the bladder was held in place by its attachments to the prostate and, once detached, would float away. Only in the last case, in which complete prostate resection occurred in 30 minutes with little fluid extravasation, were we able to complete the perineal Vest sutures.
Discussion
NOTES-RP for the potential management of localized prostate cancer was successfully demonstrated in the canine model. In this case, the natural orifice was the meatus of the urethra, the transluminal component was the extraprostatic dissection through the urethra, and endoscopes were used for visualization, meeting the definition of NOTES by the Urologic NOTES Working Group. 1 We previously described our technique for NOTES-RP using the holmium laser in the cadaver model. 15 To our knowledge, this report is the first description of NOTES-RP in a living model.
The unique properties of the holmium laser make it ideal for minimally invasive surgery. The 2140 nm wavelength is highly absorbed by water with only 0.4 mm of tissue penetration, thus allowing for precise dissection while maintaining hemostasis. In the canine, the holmium laser precisely controlled all blood vessels, generally before bleeding occurred. Although the holmium laser has a limited depth of tissue penetration, it is uncertain how the use of this laser for prostate resection would affect nerve function should NOTES-RP be considered for clinical application.
Because the holmium laser operates with normal saline irrigation, electrolyte changes secondary to absorption of hypotonic fluid should be of minimal concern; however, the risk of fluid absorption is not trivial. Shah and colleagues 17 demonstrated that more than 26% of patients who were undergoing a standard HoLEP procedure will absorb saline at a mean of 459 mL per procedure. 17 The authors found that prostate weight, irrigant time, and fluid used increased absorption. Although fluid was absorbed, it did not affect serum electrolytes. It is logical to assume that fluid absorption will be even greater with NOTES-RP because the initial step of the procedure is to perforate the prostate capsule. Assuming normal renal and cardiac function, however, the absorption of saline should theoretically be tolerated.
The accumulation of fluid in the abdominal cavity and development of compartment syndrome is another concern of NOTES-RP in this model. Because of the intra-abdominal location of the canine prostate and bladder, compartment syndrome was indeed problematic. The potential for similar fluid extravasation in the human should be less because, unlike the canine, the procedure is entirely retroperitoneal. In our previous cadaveric models, no intra-abdominal fluid was noted. 15 Because the procedure is further refined, concerns of abdominal fluid collections could be potentially alleviated by the initial placement of a retropubic drain.
Another limitation of the procedure is the vesicourethral anastomosis, because a poor anastomosis risks fibrosis and the development of bladder neck contractures, as well as incontinence. Because of equipment and anatomic limitations, we were only able to perform the anastomosis in one canine. The incompatibility of the endoscopic equipment and the suturing device makes the reconstruction of the urethra difficult. It is possible that an apposition catheter such as that described by Hruby and colleagues 18 could be used. We anticipate with further equipment development and fixation of the bladder to the pelvis, a mucosal to mucosal vesicourethral anastomosis can be achieved in humans.
Furthermore, to perform a NOTES-RP and maintain oncologic priniciples, a tissue retrieval device, other than morcellation, needs careful consideration. Once morcellation is performed, only tissue grade can be determined, not stage. Staging of prostate cancer is necessary to assess risk of tumor progression and severity of disease; thus, some other means of tissue retrieval will need to be developed.
Before introducing the procedure in the living human, technologic advancements and preliminary studies will be necessary. Performing the surgical procedure with a pelvic drain in place and with open surgical removal of the tissue specimen will be necessary to assess safety and oncologic success before pure NOTES-RP can become a feasible surgical option.
Conclusions
NOTES-RP appears to be feasible in the living canine model. Bleeding was minimal, easily controlled, and did not obscure endoscopic visualization. Although tissue approximation is feasible, further equipment refinements are necessary to perform a true mucosal to mucosal vesicourethral anastomosis. While NOTES-RP is not currently clinically applicable, this work represents a critical step in the translation of the concept.
Footnotes
Acknowledgments
We would like to thank LSI Solutions, Inc. (Victor, NY) and specifically Jude Sauer, M.D., for gracious donation of time, innovation, and materials.
Disclosure Statement
No competing financial interests exist.