
Abstract
Introduction:
Laparoendoscopic single-site surgery (LESS) represents the latest innovation in laparoscopic surgery. We compare in dry and animal laboratory the efficacy of recently introduced pre-bent instruments with conventional laparoscopic and flexible instruments in terms of time requirement, maneuvrability, and ease of handling.
Materials and Methods:
Participants of varying laparoscopic experience were included in the study and divided in groups according to their experience. The participants performed predetermined tasks in dry laboratory using all sets of instruments. An experienced laparoscopic surgeon performed 24 nephrectomies in 12 pigs using all sets of instruments. Single port was used for all instrument sets except for the conventional instruments, which were inserted through three ports. The time required for the performance of dry laboratory tasks and the porcine nephrectomies was recorded. Errors in the performance of dry laboratory tasks of each instrument type were also recorded.
Results:
Pre-bent instruments had a significant advantage over flexible instruments in terms of time requirement to accomplish tasks and procedures as well as maneuvrability. Flexible instruments were more time consuming in comparison to the conventional laparoscopic instruments during the performance of the tasks. There were no significant differences in the time required for the accomplishment of dry laboratory tasks or steps of nephrectomy using conventional instruments through appropriate number of ports in comparison to pre-bent instruments through single port.
Discussion:
Pre-bent instruments were less time consuming and with better maneuvrability in comparison to flexible instruments in experimental single-port access surgery. Further clinical investigations would elucidate the efficacy of pre-bent instruments.
Introduction
A major problem for the wider introduction of LESS is the acquisition of sufficient laparoscopic skill and the potential to overcome the demanding learning curve of laparoscopy. Current literature included several studies on laparoscopic training schemes aiming to train urologists in the demanding laparoscopic surgical practice without reducing the quality of provided services. 9,10 Moreover, ergonomic difficulties are always present in laparoscopic surgery and should be overcome to adopt the techniques. Optimal instrument positioning in laparoscopy has a significant impact on the surgeon's ability to successfully accomplish the procedure. Traditional triangulation of the used instruments is considered a critical point for the technical accomplishment of the procedure since it facilitates surgical dissection and the performance of necessary surgical maneuvres. Nevertheless, single-port technique does not provide the potential for triangulation of the instruments used. Innovative instruments have been designed in an attempt to overcome the above difficulty. The use of these instruments facilitates the performance of the procedure and overcomes any time-consuming, instrument-related difficulties during the operation. Instrumentation remains one of the main challenges for further development of single-port surgery. 11,12 Recent development in the instrumentation of LESS is the introduction of the pre-bent instruments.
The current experimental study compares flexible (e.g., Real Hand™; Novare Surgical Systems, Cupertino, CA, and Autonomy Laparo-angle™; Cambridge Endo, Framingham, MA) with pre-bent instruments (Olympus, Hamburg, Germany) and conventional laparoscopic instruments in dry and wet laboratory settings to evaluate the following points: The performance of each instrument design in terms of time requirement for the accomplishment of laparoscopic tasks. The maneuvrability and ease of handling of each instrument design in the execution of basic laparoscopic tasks.
Materials and Methods
Instruments
The following instrument sets were used for both dry and wet laboratory studies: A set of conventional laparoscopic pair of scissors and graspers (rigid and straight instruments). A set consisted of articulating laparoscopic graspers (RealHand; Novare Surgical Systems) and standard laparoscopic scissors. A set of a pair of pre-bent graspers (Olympus) and standard laparoscopic scissors.
Figure 1 shows the pre-bent graspers (A), scissors (B), and articulating laparoscopic graspers (C). The pre-bent design (Fig. 1A) was introduced in an attempt to provide instrument angulation inside the abdomen and increased maneuvrability for dissection, grasping, and retraction. The conventional instrument set was placed through three ports in both dry and animal laboratory according to the conventional laparoscopic triangulation fashion. The flexible and pre-bent instrument sets were placed through a single port (Tri-port-Advanced Surgical Concepts, Wicklow, Ireland) in both dry and wet laboratory experimental studies. The Tri-port has three channels for instruments and one for gas insufflation. One of the instrument channels is 12 mm in diameter and the remaining 5 mm. All tasks in dry as well as animal laboratory were performed with the use of a 5-mm rigid laparoscope with 30° lens (Olympus). All instruments used were 5 mm in diameter, and only clipping devices and staplers used for vascular control in the wet laboratory setting were 12 mm in diameter.
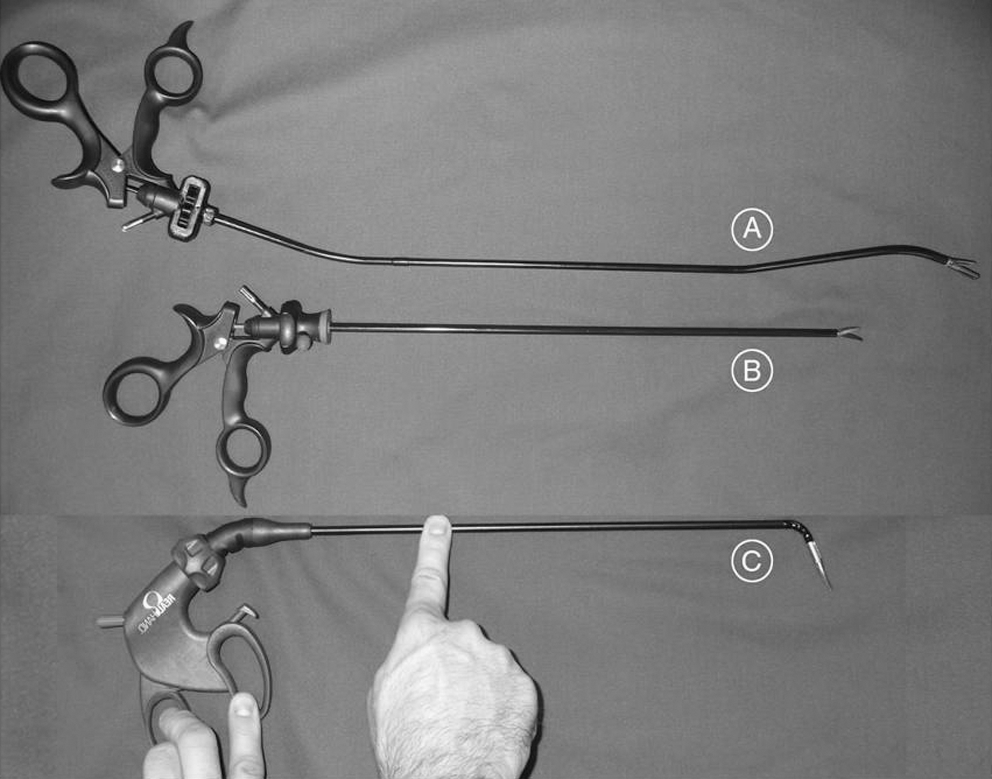
Instruments used in the dry and animal laboratory. Pre-bent grasper (
Participants
Two groups of participants were included in the study and performed the assigned tasks in a manner similar to the traditional laparoscopic training in dry laboratory. Each group included three participants. Group A consisted of three medical students with limited exposure to laparoscopic surgery (holding camera in at least 30 laparoscopic procedures), and group B consisted of three laparoscopic surgeons who had performed maximum 10 laparoscopic procedures each. None of the participants had previously used flexible or pre-bent instruments.
Dry laboratory
We evaluated basic laparoscopic surgical tasks (grasping, retraction, and cutting) in a dry experimental laboratory using three different sets of instruments. The participants had never before used flexible instruments and were allowed to familiarize themselves with the instruments for 5 minutes before the initiation of the experiment. Measurements for each participant took place. The use of different instrument sets took place in random order. During the tasks, the camera position was fixed to avoid interference with the instruments and to provide the best possible view. The first task was practicing of grasping (task 1). The participants had to use alternatively each hand to grasp five objects (match sticks) placed in a container and transfer them between the two containers (Fig. 2A). For the cutting task (task 2), the participants had to grasp and apply tension (with the nondominant hand) on a stomach shape drawn on a paper and to use the dominant hand to cut out the stomach shape (Fig. 2B). The intended line of dissection was performed between the stomach wall and vessels as shown by arrows in Figure 2B. The same tasks were repeated using all three aforementioned sets of instruments. Dropping/or misplacement of a stick, a cut into the shape of stomach, or tearing of paper while making a dissection were considered as errors.
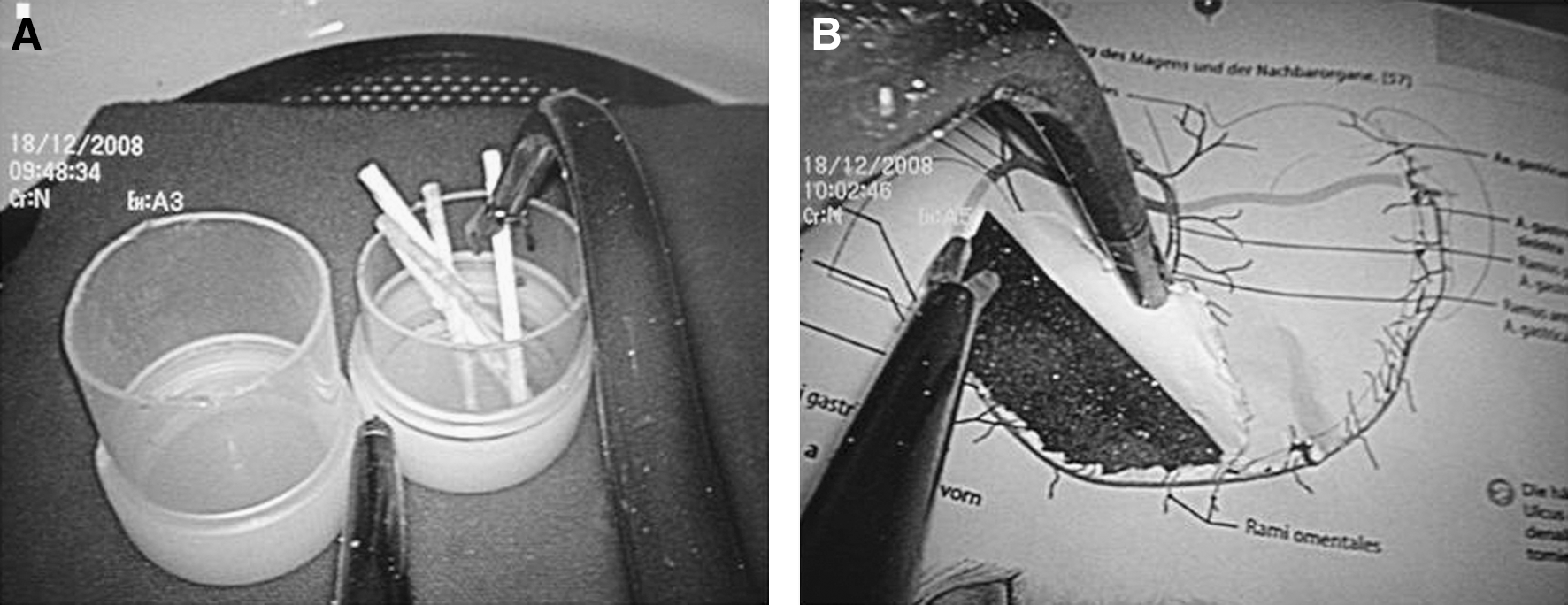
Tasks performed in the dry laboratory. (
The following parameters were recorded for the evaluation of the outcome: time required for the accomplishment of each task and the number of errors that were made during the execution of each task. In addition, the quality of stomach shape excised was assessed for smoothness of cutting line and incorrect advancement of dissection line into the stomach shape during the performance of the task. The quality of the excised shape was evaluated by two experienced surgeons who rated the outcome as fair, good, very good, and excellent depending upon the smoothness of cutting line and any advancement of dissection line in the shape. The evaluation of the excised stomach shapes took place without the surgeons knowing which participant performed the task and the instrument set used. All participants were asked to subjectively report which instrument set was easier to use and more maneuvrable at the end of the dry laboratory experiments.
In general, the tasks of the dry laboratory were carefully selected to be simple so that the differences between the two groups reflect the influence of instruments. Moreover, we investigated with the above setting the influence of laparoscopic experience in adaptation with each instrument configuration.
Wet laboratory
The experimental procedures in the wet laboratory consisted of nephrectomies bilaterally in porcine model using the three sets of instruments in random order (conventional, flexible, and pre-bent instruments). Each instrument set performed four right-sided and four left-sided nephrectomies.
Twelve domestic pigs weighting between 20 and 25 kg were included in the experiment. The protocol was approved by the Animal Care Committee of our Institution. All animals were allowed a minimum period of 72 hours before the procedure to recover from the stress of transportation. Food was withheld for 12 hours before anesthesia. A combination of ketamine, xylazine, and atropine sulfate was administered to induce anesthesia. All pigs were intubated and ventilated. Intravenous propofol 5% was used to maintain anesthesia for the whole duration of the procedure. High doses of anesthesia were administered for euthanasia.
The procedures were carried out using three ports (for conventional instruments) and single-port laparoscopic access (for flexible and pre-bent instruments) as described above. All procedures were performed by an expert surgeon (J.-U.S.) with the assistance of the same camera holder. Pneumoperitoneum was obtained via Veress needle insufflation. Single-port access took place through a 3-cm midline incision performing an already described method. 13 In each pig, nephrectomies bilaterally were performed using the same instrument set, and each procedure was divided into four steps that included trocar placement, mobilization of the renal pedicle, clipping and division of the renal pedicle, and mobilization of the whole kidney (Fig. 3). The wet laboratory study took place to assess the successful accomplishment of each step of the procedure using the aforementioned sets of instruments. The ease to use and maneuvrability of each set of instruments by the participant were recorded. A total number of 24 nephrectomies were performed in 12 pigs. Eight nephrectomies were performed with each instrument set.
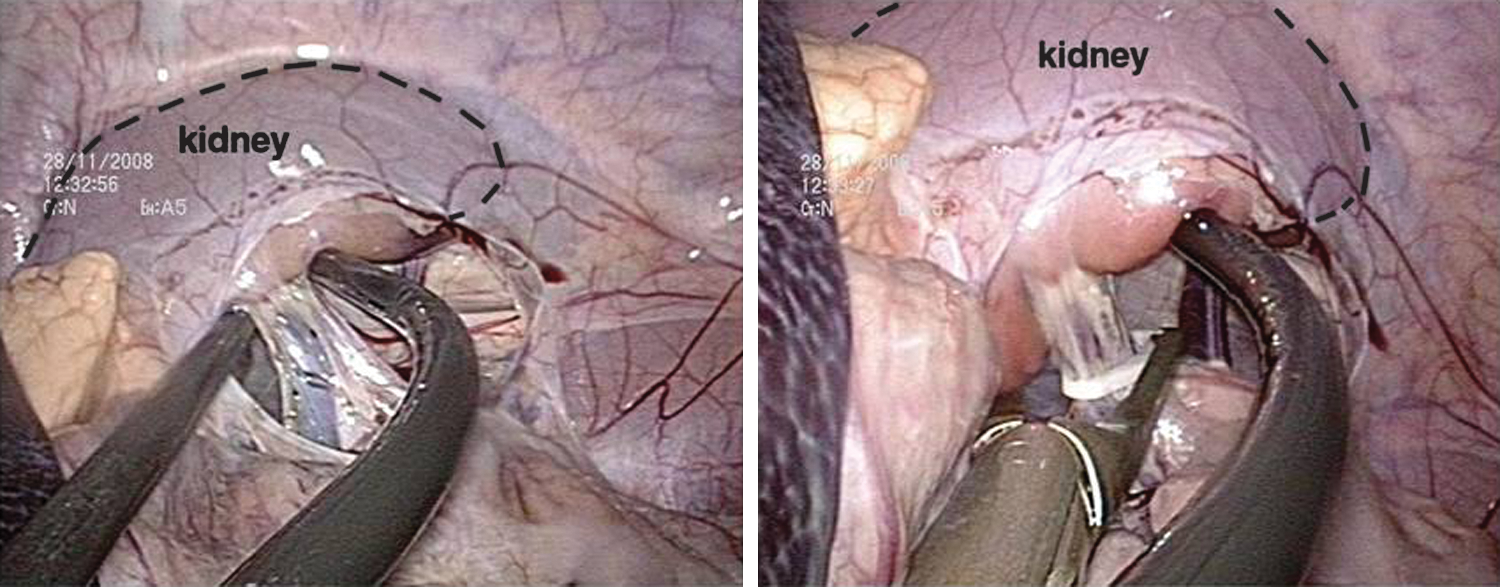
Dissection of the pedicle using pre-bent instruments. Note outlined kidneys.
Statistical analysis
Possible differences in either the time required for performing each task by the participants of the aforementioned groups in the dry laboratory or in the time required for performing the various steps of nephrectomy by the surgeon in the wet laboratory using three sets of instruments were investigated using one-way analysis of variance (ANOVA) or its nonparametric form (Kruskal–Wallis test) where appropriate. In cases where significance was reached, the Tukey–Kramer test was used to identify the particular pairs that differ significantly. Differences in the time for performing step 1 in particular were tested with the nonparametric Mann–Whitney test, because it only involves two groups. Statistical significance was set, and p-value was defined as <0.05.
Results
Dry laboratory
Table 1 demonstrates the comparison of time required to perform task 1 by the two groups of participants using the three types of instruments. Longer time was necessary for both groups to complete the task using flexible instruments in comparison to the conventional or pre-bent instruments. Significantly longer time necessary for the accomplishment of task 1 was only observed when flexible instruments were used in comparison to the conventional instruments by group A (p-values 0.0469 and 0.0538 reported by Kruskal–Wallis test—preferred because of the small sample size—and ANOVA, respectively). There was no statistically significant difference between the time required to complete the task using conventional or pre-bent instruments in both groups.
Task 1 was practicing of grasping. Five objects were transferred between two containers with the use of each instrument set.
The observed significant difference in group A is attributed to the pairs flexible versus conventional (Dunn's multiple comparison post hoc test).
ANOVA = analysis of variance; SD = standard deviation.
No significant difference was observed in the time required to perform task 2 among the groups and various instruments (Table 2). The use of flexible instruments by both groups resulted in higher number of errors (Table 3). The quality of stomach shape dissected from the paper in task 2 was rated good to very good in all participants except for two shapes in group A (less experienced surgeons), whose task was rated as fair. The latter shapes were both cut using flexible instruments.
Task 2 was the cutting task; the participants had to grasp and apply tension (with the nondominant hand) on a stomach shape drawn on a paper and to use the dominant hand to cut out the stomach shape.
No significant difference in error rates between two-port and single-port access was observed among groups A and B (Fisher's exact test). Task 1, p = 0.5603; task 2, p = 1.
Wet laboratory
Porcine nephrectomies were successfully completed in 12 pigs (24 renal units). There was no statistically significant difference in the time required to place ports for both techniques (Table 4). Performance time for step 4 of the procedure was significantly longer using flexible in comparison to the conventional instruments or pre-bent instruments. The time required to complete steps 2 and 3 of nephrectomy was not significantly longer in using flexible instruments. Blood loss was minimal during the procedures.
Median time ± SD (minimum–maximum).
The observed significant difference is attributed to the pairs flexible versus conventional and flexible versus prebent (Tukey–Kramer post hoc test).
All participants found flexible instruments difficult to use with poor maneuvrability during the tasks. All participants favored pre-bent instruments over flexible ones.
Discussion
The performance of laparoscopic operation requires three to six ports for a given operation. Each port increases the risk for bleeding, internal organ injury, port-site hernia, and decreases cosmetic outcome. 7 Single-port access surgery was introduced as a new technique that could reduce the aforementioned problems of laparoscopic surgery. A number of recent reports have been published on single port or incision-free surgery. 6 –8,11 –14 Several terms have been used to describe single-port surgery, and there is an ongoing effort for standardization of nomenclature. 15 Preliminary studies indicate that single access surgery may have advantages over standard laparoscopic approach such as less postoperative pain, faster convalescence, and better cosmetic result. 8 Nevertheless, current data do not indicate any significant advantage of LESS over laparoscopy in terms of operative time, analgesic use, blood loss, and complication rate. 7,18 Further comparative clinical evaluation of the technique would elucidate the potential advantages of LESS.
The performance of LESS procedures is associated with technical challenges for several reasons including minimal or no triangulation of the conventional laparoscopic instruments leading to clashing of the instruments (both inside and outside the abdomen) and poor range of movements. 14 To overcome these limitations, various instruments have been introduced in medical market. Recently, flexible laparoscopic graspers have been evaluated in experimental models and used in clinical practice. 12,16,17
In this study, we compared flexible graspers with conventional laparoscopic instruments and recently introduced pre-bent instruments in dry and animal laboratory settings for their time requirement and maneuvrability to complete basic laparoscopic tasks by two groups of participants with varying level of laparoscopic experience. Evaluation in the operative field included an ablative procedure in the form of nephrectomy by an experienced surgeon in pig model. The conventional laparoscopic instruments were included in the study as the standard type of instrumentation with which newer instruments should be compared. Since rigid instruments perform poorly in LESS, the use of multiple ports for the latter instrument set enabled the direct comparison of each instrument set in appropriate conditions. Our experimental results with the new pre-bent instruments revealed that these instruments were more maneuvrable and less time consuming in the accomplishment of dry laboratory tasks and various steps in the nephrectomy procedure in comparison to the flexible instruments. These findings were consistent between the two groups of participants irrespective of their level of experience. In addition, experience with flexible instruments revealed that these instruments clash outside the port and were difficult to be exchanged by the assistant. 12 The pre-bent instruments have the advantage that they did not interfere with other instruments in the operative field as well as there was limited clashing of the instrument outside of the port because of their bent design. Figure 4 presents an ideal setting for the performance of LESS operations with the use of pre-bent instruments by both hands of the surgeon (we used only pre-bent graspers during our investigation). Pre-bent instruments are longer than the usual laparoscopic as well as flexible instruments. The longer and bent design provides in the above setting even more space for the movement of the instruments outside the port. The latter feature in addition with the aforementioned limited interference of the pre-bent instruments in the operative field renders the pre-bent instrumentation as an appealing option for LESS. The use of a flexible laparoscopic camera, which was bent outside the port, proved to prevent clashing of camera with the instruments (Fig. 4).

Pre-bent instruments in both hands along with flexible endoscope during the performance of nephrectomy in the pig model. An ideal instrument configuration is presented with a new laparoscopic camera design that was not used in the experiments. The experiments were performed with the use of combination of flexible or pre-bent graspers with conventional laparoscopic instruments. The camera used in the experiments was a rigid 5-mm laparoscope with 30° lens. Note the relationship of flexible endoscope with pre-bent instruments.
The pre-bent instrumentation, because of the limited degrees of freedom, was expected to require longer time to overcome the learning curve in comparison to the flexible instruments. 7 The results of our study show that these instruments were easy to use and less time consuming even in the hands of less experienced participants. Even though the evaluation of ease of use and maneuvrability was subjective, the subjective factor remains an important aspect for the selection of instruments by a surgeon. Moreover, the objective results of the measurements and the statistical analysis were confirmed by the subjective evaluation of the participants.
A limitation of the current study is introduced in the wet laboratory setting. An expert surgeon performed all procedures, and possible difficulties in the manipulation of instruments were probably overcome by the higher expertise of the surgeon. Thus, the expected steep learning curve of the new instrumentation mentioned above could have been easily overcome. Considering the fact that the limitation was present in all sets of instruments, the results of the current study are reliable and probably reflect the efficacy of instruments in cases where the learning curve has been overcome. Moreover, experienced surgeons perform the LESS nephrectomy procedures in the real setting. Thus, the evaluation of the instruments in the simulated conditions of the wet laboratory by these surgeons is probably the best method for obtaining reliable results.
The design of pre-bent instruments provides angulation of devices in the operative field and facilitates dissection by imitating instrument triangulation of standard laparoscopic technique. The above feature probably explains the statistically faster accomplishment of step 4 in nephrectomy procedure with the use of pre-bent in comparison to the flexible instruments. Moreover, even experienced laparoscopic surgeons have no experience in the use of flexible instruments, and adaptation to the specific instrument characteristics probably requires training. In fact, Raman et al 18 observed that previous experience with the use of new instruments in animal laboratory setting contributed to the shortening of learning curve. All participants subjectively evaluated the maneuvrability of articulating instruments as poor. The above difficulty was reflected in the higher number of errors and poor quality of dissected shapes seen during the performance of tasks in the dry laboratory (even in the hands of experienced participants). The latter observation could be attributed to the less predictable force transmitted to the tip of the graspers because of the dissipation of force along the flexible portion of instrument shaft that is a known disadvantage of flexible design. 14
Flexible instrumentation has been evaluated in animal models. Raman et al 16 successfully accomplished eight porcine nephrectomies using articulating graspers. The mean operating time was 49 minutes, which is significantly higher compared with the current results. In addition, we used the same articulating instruments. Time required to perform nephrectomy using pre-bent instruments was significantly lower, in the cases of pedicle dissection in comparison to the flexible instruments. Laparoscopic experience could probably be responsible for less time consumption during nephrectomy in a porcine model in comparison to the reported results by the aforementioned investigating group. 16
An important limitation of the current study was the limited sample size and the absence of a power analysis during the design phase of our experiments. It is always better to have large sample sizes. Nevertheless, the evaluation of a given sample size as too small or adequately large takes place only with the adaptation of a power analysis. The fact that not all time differences prove to be significant does not by itself render the sample size smaller than it should be. An optimal power analysis should be performed before the actual measurements took place, but we overcome this problem using robust nonparametric tests. We used nonparametric forms of the traditional t-test and ANOVA, where appropriate, to ensure robustness of the results against small sample sizes.
The current study was based only on dry and animal laboratory to evaluate the presented instruments. Thus, the newly introduced pre-bent instruments should be further evaluated in animal experimental procedures and clinical investigation to draw scientifically solid conclusion for their advantages. Moreover, clinical evaluation is the most appropriate way to confirm and to definitively assess the efficacy of the pre-bent instruments.
Conclusion
In conclusion, pre-bent instruments were less time consuming and with better maneuvrability in comparison to the flexible instruments in experimental single-port access surgery. There were no significant differences in terms of time between the conventional instruments through three ports and pre-bent instruments through single port for performance of porcine nephrectomies. Further clinical investigations would elucidate the efficacy of pre-bent instruments.
Disclosure Statement
No competing financial interests exist.