
Abstract
Background:
It has been postulated that laser insertion sheaths prevent mechanical damage to the inside of working channels of flexible ureteroscopes. The presented study, for the first time, aims at confirming this hypothesis and visualized the damage of the endoscopic working channel by video-endoluminal observation after a series of laser fiber passages with or without the protection of a laser fiber insertion sheath.
Materials and Methods:
Four nonassembled working channels of two different manufacturers (Olympus™, Wolf™) were tested in a deflection model (50° and 180°). Flexifib™ laser fibers (LISA laser products) with an optical core diameter of 273 μm were inserted through 0.9% NaCl irrigated working channels in cycles of 10 insertions either with or without protection of the Flexgard™ insertion sheath. After 30 insertions, the examination cycle was reduced to 5 insertions each cycle until breakage. Test cycles were followed by endoluminal video examination of the working channel with the 2.4F flexible fiber scope by Polydiagnost™. Damage to the working channel was classified as streaks with superficial stress marks of the surface, scratches with embossed margins, or perforations.
Results:
No scratching or perforation occurred in the insertion sheath group in up to 150 insertions in all working channels and both deflection grades. In the group without insertion sheaths, scratches were visible after 40 to 50 insertions with 50° deflection and 30 insertions with 180° deflection. Perforations of the working channels were seen after 95 insertions with 50° and 60 insertions with 180° deflection.
Conclusions:
Severe damage to working channels depends on the degree of deflection and may occur after 30 insertions only. Relevant damage to the working channel may be avoided by using a laser fiber insertion sheath.
Introduction
Despite the obvious utility of laser energy, the repeated insertion of laser fibers is one of the most common causes of mechanical damage to the working channel of flexible ureteroscopes (FU) during routine ureteroscopic procedures. 12 Seventy percent of the damage is caused by the sharp-edged tip of the laser fiber scratching or perforating the working channel during insertion, as reported by the producing companies. 13,14 Another issue is the deterioration secondary to inattentively firing of the laser inside the working channel or to thermal damage caused by malfunction or deterioration of the fiber itself. 15 Working channel protecting approaches have been reported by Hollenbeck et al 16 using a 2F catheter to protect the working channel before inserting laser fibers.
Since a laser insertion sheath with Touhy-Borst locking (Flexguard™) was introduced with the intention to reduce mechanical damage to the working channel in 2006, two studies have dealt with the feasibility of use. Durak et al 17 could show that the insertion sheath reduced the force required for laser fiber insertion while the ureteroscope is deflected. Further, we could demonstrate that the laser fiber carrying sheath could be inserted in a fully deflected instrument without moving the target out of sight. 18 The insertion sheath did not significantly enlarge the smallest achievable radius of curvature in these instruments (FU). As all previous studies regarding the lifespan of ureteroscopes reflected only on the end point of instrument breakage, the intrinsic gradual detoriation of the working channel with each use could not be demonstrated. The present study is the first to investigate the actual protective effect of a flexible laser fiber insertion sheath on the integrity of the working channel using a video-endoluminal examination of the deteriorations in the working channel after a series of laser fiber passages with and without the protection of an insertion sheath.
Materials and Methods
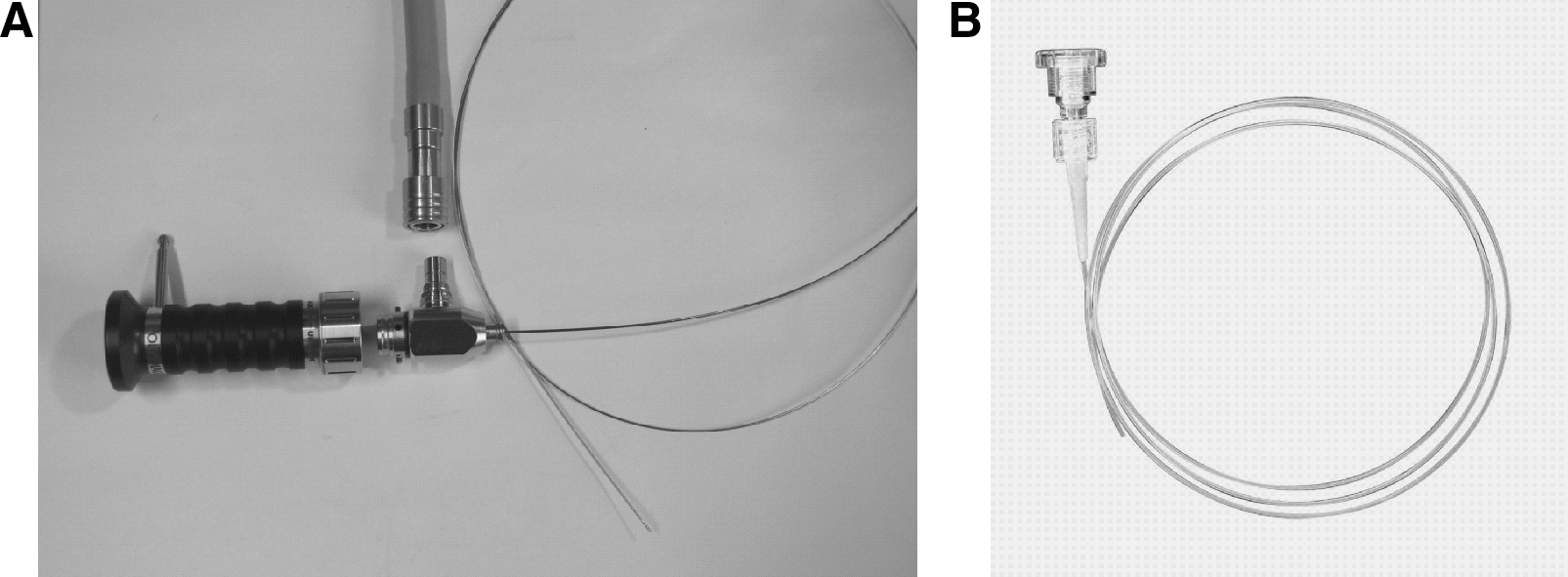
The FlexGuard laser fiber insertion sheath has an outer diameter of 0.77 mm (2.4F) and a luminal diameter of 0.7 mm (2.1F). The sheath is made from flexible PTFE (Teflon) tubing material with a proximal Touhy-Borst adapter and is compatible with the most common 200 and 273 μm laser fibers. The Touhy-Borst adapter allows the locking of the sheath on the laser fiber with the sharp-edged distal tip of the laser fiber in a “capped position” ∼2 mm inside the sheath for insertion into the FU (Fig. 1B). A 273 μm laser fiber (FlexFib™ bare fiber with an outer diameter of 0.42 mm [1.3F]) was used for the insertion study. The distal tip of the laser fiber was cleaved with a commercial fiber cleaving tool to produce a reproducible regular sharp-ended tip.
(
Four separate nonassembled working channels by two different manufacturers (Olympus and Richard Wolf) were each tested in a deflection model (Table 1) Two of each were kept for insertion of the laser fiber with the insertion sheath and two for without the insertion sheath.
Milling tract equates 50° or 180° deflection.
We provided a deflection model (Fig. 2) where four grooves were countersunk into a 3 cm thick synthetic board. Each groove mimics a deflection grade of its own. The embossing was carried out by a computer numerically controlled milling machine. The grooves were dimensioned exactly to accept the single working channels. The radii of the curvatures in the deflection model aimed at reproducing the bending of an FU in use. A certain amount of resistance is experienced when the fiber or the fiber inside an insertion sheath is pushed down the deflected working channel.
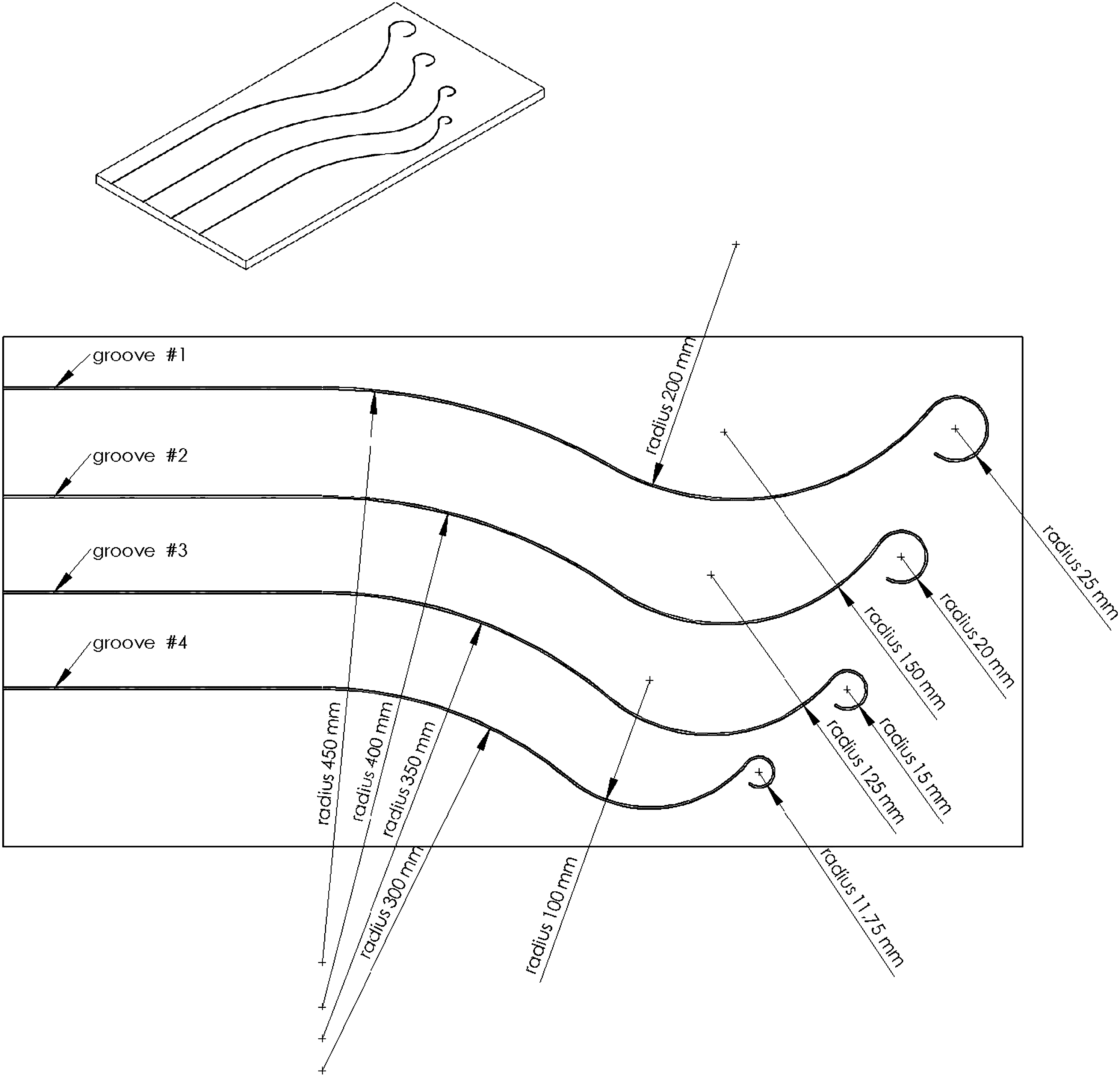
Deflection model.
Only two of four available grooves of the deflection model (Fig. 2) were used for our investigations: the groove (G1) to resemble a “close to straight” deflection (50°) with large radii through which the urologist still might push the fiber without an insertion sheath (Fig. 3A) and the 180° deflection which resembles a “lower pole” deflection (Fig. 3B) with smaller radii (G3).

(
Ten serial insertions in 0.9% NaCl irrigated working channels at the various test conditions were performed either with group A or without the Flexgard™ insertion sheath (group B) followed by endoluminal video examination of the working channel with the 2.4F flexible Polydiagnost endoscope (6000 Pixel, outside diameter 0.77 mm (2.4F), 120 cm length; Polydiagnost, Pfaffenhofen, Germany (Fig. 1A). The working channel was flushed with 0.9% NaCl by a syringe. Before video examination, all working channels were blown dry by pressured air.
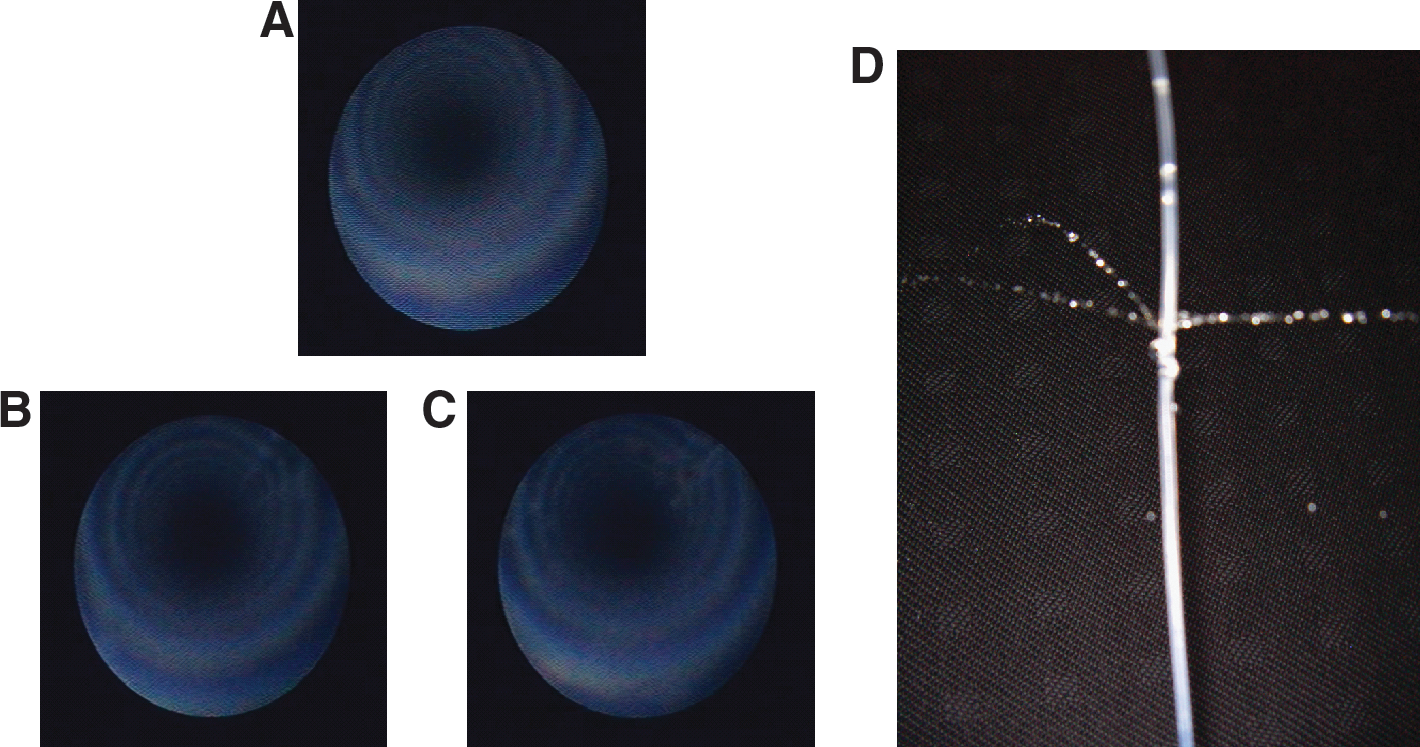
After the first 30 insertions, the cycle was reduced to 5 insertions each cycle until perforation for the fiber-only setup. Damage was classified as streaks with superficial stress marks of the surface, scratches with embossed margins, and perforations (Fig. 4).
(
Results
No scratches and no perforation occurred in the insertion sheath group in up to a 150 insertions in all working channels and at all deflection grades. Only streaks could be detected in this group (Olympus and Wolf) after 75 and 80 insertions in the 180° deflection position and after 100 and 110 insertions in the 50° deflection position, respectively. Scratches occurred in the setting without protection sheaths after 50 (Olympus) and 40 (Wolf) insertions at 50° and in up to 30 insertions at 180° deflection grade. Perforation occurred at 180° deflection in all working channels without insertion sheaths below 60 insertions and at 50° deflection at <95 insertions (Table 1). The perforations solely occurred in areas that had previously shown scratches.
Discussion
The presented study is the first to demonstrate the intrinsic protective effect of a laser fiber insertion sheath on the integrity of the working channel over its entire lifespan in a reproducible mechanical stress model. In addition to that, it is the first publication to deal with video-endoluminal assessment of damage to the working channel after a series of laser fiber passages with and without the protection of an insertion sheath. The sharp-edged tip of the laser fiber has been identified to be the main cause of mechanical damage to the working channel, accounting for up to 70% of the total damage occurring. 13,14 Advances in fiber optic technology and evolution of flexible endoscope design have allowed RIRS to evolve into a widely accepted concept for the treatment of upper tract abnormalities. The pitfalls of maintaining the endoscopes in proper working condition 19 and their extended use have led to concerns about the cost effectiveness in the changing economic situation of health care systems. 12,20
Earlier publications dealt with the problems related to instrument cleaning, the training of staff, 10 the storage of the ureteroscope during the procedure to avoid handling related damage 15 or had reported on techniques on how to improve the deflection of the working tip, shorten the duration of the procedure or the changing of operation strategies. 13,14 Approaches for the protection of the working channel have been reported by Hollenbeck et al 16 using a 2F ureteral catheter.
In contrast to the ureteral catheter, the subsequently introduced FlexGuard insertion sheath moves inside the working channel already loaded with the laser fiber, which remains stationary with regard to the sheath. The Touhy-Borst allows reversible locking of the fiber in this capped position. This combo insertion of sheath and fiber allows a safe passage without accidental scratching of fiber in the working channel.
Our findings in the nonassembled working channels could demonstrate that all relevant fiber-tip damage could be prevented by the use of the Flexguard laser fiber insertion sheath. We were able to show that severe early detoriations that precede final perforation already occur in a relatively early phase of the wear lifespan, even in moderately deflected instruments if the fiber is inserted alone. In contrast to all previous publications that proposed or hypothesized the protective effect of a laser fiber insertion sheath, this study could actually visualize the damage or the maintained integrity over time.
In our previous publication, we showed that the laser fiber carrying the sheath could be inserted in a fully deflected instrument without moving the target out of site. It did not significantly enlarge the achievable radius of curvature in these instruments. 18
Additionally, Durak et al 17 showed that the investigated insertion sheath reduced the force required for laser fiber insertion while the ureteroscope is deflected. The insertion sheath did not prevent thermal damage to the ureterorenoscope (UR) caused by accidental firing of the Ho:YAG laser. The experience showed that the reduction of irrigant flow due to the presence of the sheath can be avoided by withdrawing the insertion sheath, thus leaving behind the protective sheath threaded onto the laser fiber external to the FU.
Since costs of maintenance and reliable availability of flexible instruments have become an important issue in high volume centers of RIRS, the benefit of the investigated laser fiber insertion sheath and their market competitors outrun the extra costs for the additional disposable (55€). Preventing early damage and breakage elongates the maintenance intervals, avoids earlier necessity to repurchase, and further reduces the resentment of physicians and patients due to instruments not being available for their planned surgical treatment.
Conclusions
Severe early damage to the working channel occurs in an early phase of the wear lifespan, even in moderately deflected instruments if the fiber is inserted without protection. All relevant mechanical detoriations including perforation can be sufficiently avoided by using a laser fiber insertion sheath.
Footnotes
Disclosure Statement
No competing financial interests exist.