
Abstract
Purpose:
Laparoscopic treatment of parapelvic renal cysts, as a gold standard, is quick and effective. Ureteroscopic unroofing, however, could be used as an alternative technique in selected patients.
Patients and Methods:
Two men (aged 56 and 53 years) presented with parapelvic cyst. In the first patient, intravenous urography and CT scan revealed multiple renal cysts with a 6 × 5 cm parapelvic cyst, and the other patient showed a 6.5 × 7.5 cm parapelvic cyst, both with hydronephrosis. There were no solid tissues in the cysts. Semirigid ureteroscopy was performed and the parapelvic cyst was unroofed and marsupialized to the adjacent collecting system. Retrograde pyelography was performed within 5 hours of the procedure, and the ureteral catheter was removed. We evaluated our patients at 2 weeks and 3 months postoperatively.
Results:
We had no intraoperative or postoperative complications. Operative times were 35 and 30 minutes in patients 1 and 2, respectively. Retrograde pyelography showed contrast media filling the parapelvic cyst and the collecting system without extravasation. The first patient's flank pain was partly relieved. In the other patient, hypertension decreased noticeably (preoperational: 160/95 mm Hg, and postoperational 3 months: 135/85 mm Hg) and right flank pain totally disappeared. Intravenous pyelography and CT images showed objective improvement in hydronephrotic changes, with no evidence of symptomatic and radiographic recurrences.
Conclusions:
Ureteroscopic treatment is feasible and safe in selected patients with simple parapelvic renal cysts; however, further studies with longer follow-up periods are essential to document its durability.
Introduction
The majority of the peripheral simple renal cysts are asymptomatic. In contrast, parapelvic renal cysts are less common and more likely to be symptomatic. 1,2 Moreover, the treatment of parapelvic cysts is more difficult than the treatment of simple renal cysts. 3
In the current literature, laparoscopic cyst ablation is the procedure of choice. 4 –7 As we know, laparoscopic unroofing of parapelvic cysts require advanced surgical skills because of the complexity of the cysts and their proximity to the renal hilar structures and the collecting system. Percutaneous approach is a safe and effective method to treat peripherally located simple renal cysts, 8 but similar attempt for parapelvic cysts may carry a risk of damage to hilar structures. 9 Considering the above, however, we chose a ureteroscopic approach to drain a parapelvic cyst to assess both its feasibility and safety in selected patients as a substitute to either laparoscopic or percutaneous treatment of a parapelvic cyst.
Patients and Methods
Two men (aged 56 and 53 years) were referred to our clinic, one with a 2-month history of left flank pain, and the other with hypertension accompanied by right flank pain. Urine parameters and serum creatinine levels were within normal range. Intravenous urography and abdominal CT scan revealed multiple renal cysts with a 6 × 5 cm parapelvic renal cyst that had compressed and displaced the upper major calix (Fig. 1), and the other patient showed one 6.5 × 7.5 cm parapelvic renal cyst that had compressed and displaced the upper and middle calixes, causing moderate to severe hydronephrosis. There were no solid tissues in the cysts.
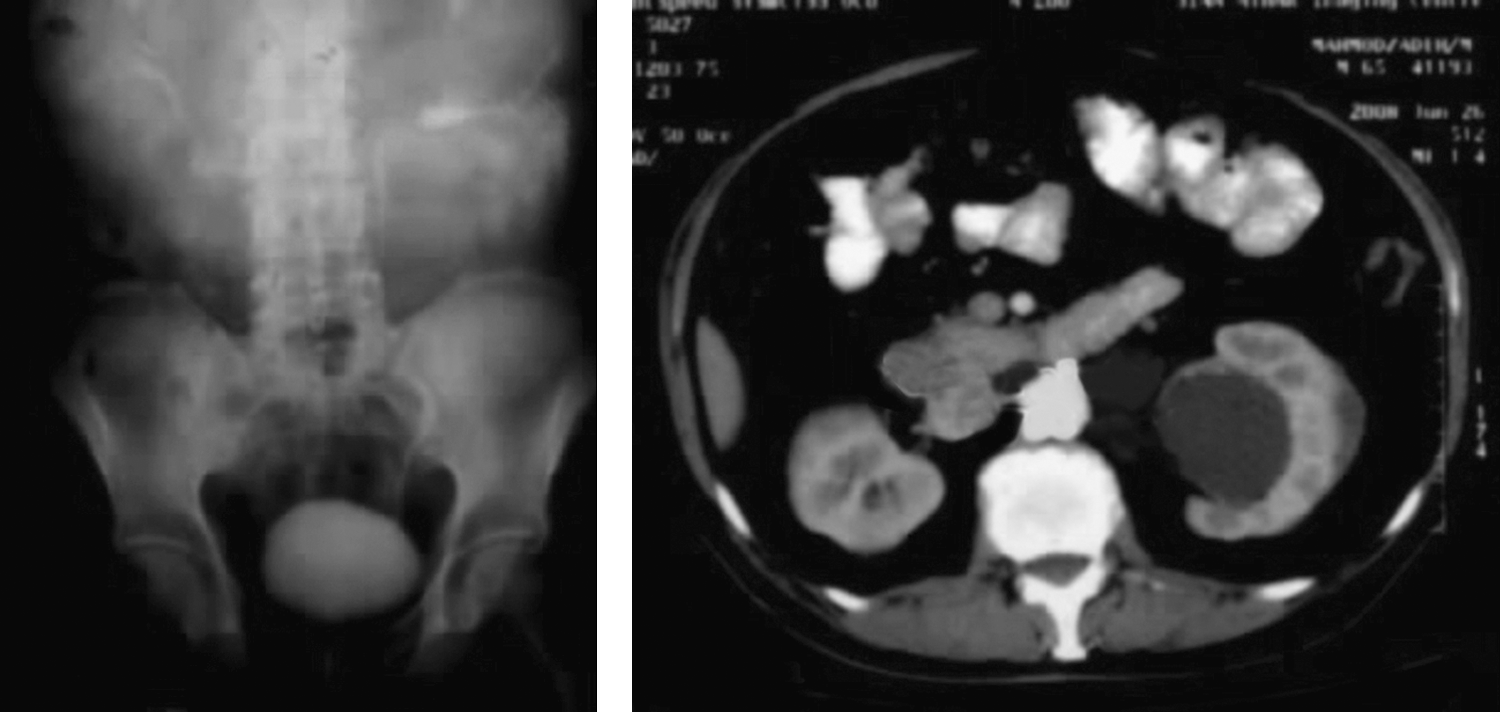
Preoperative intravenous urography and CT show simple parapelvic renal cyst with compressing effect causing hydronephrosis.
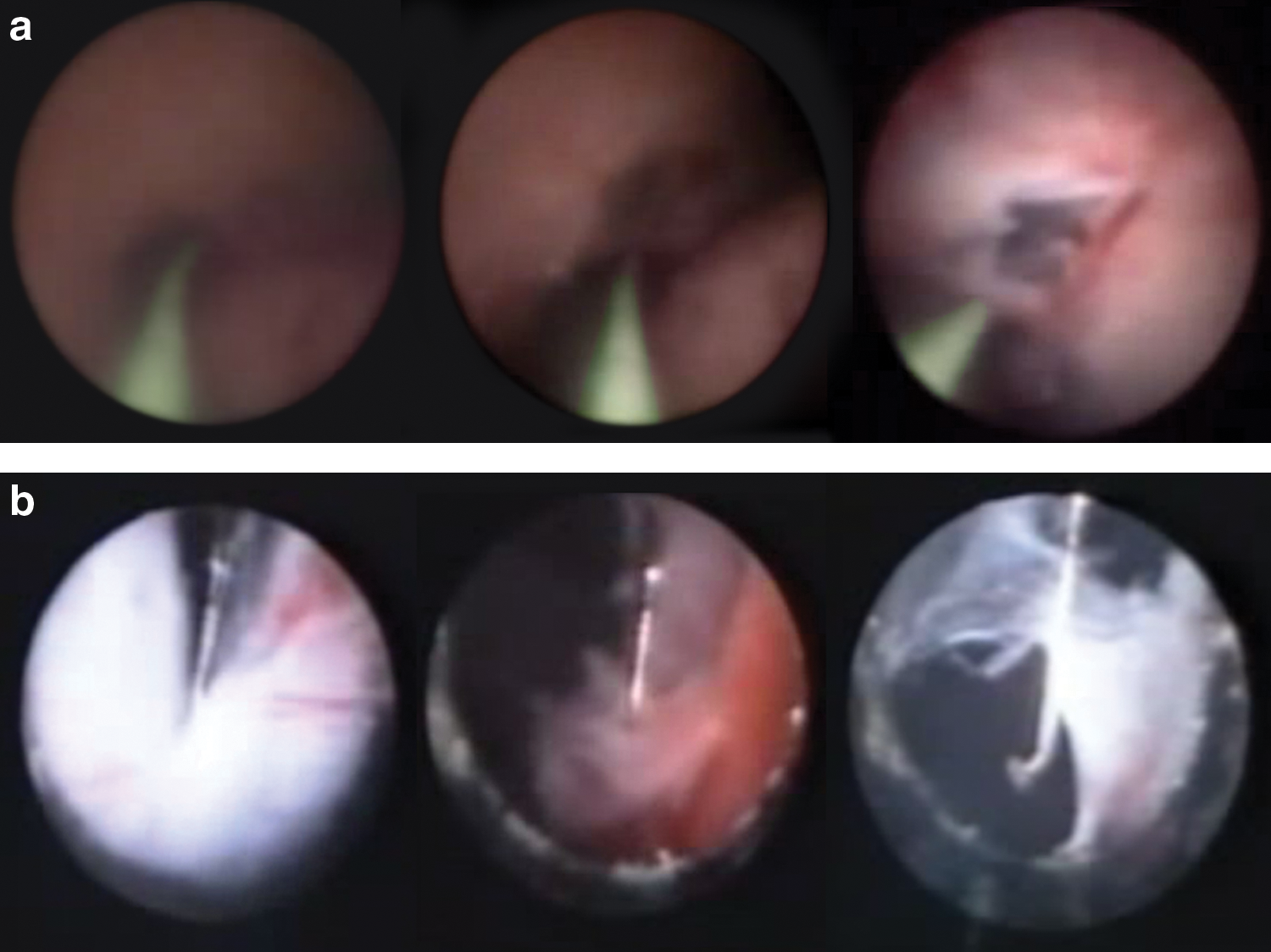
Diagnostic ureteroscopy with an 8.5F semirigid ureteroscope was done under anesthesia. The lateral renal pelvis wall was bulged because of the cyst (Fig. 2a). During the procedure, the urothelium was stripped away by the tip of the ureteroscope and the cyst wall appeared to be very thin and transparent (Fig. 2a). Afterward, the cyst wall was incised extensively by electrocautery hook in the first patient (Fig. 2b) and by holmium laser in the second one. For this, first, the middle of the cyst wall was incised. Then, the whole cyst wall was ablated by either electrocautery hook or holmium laser as mentioned earlier. The inspection of the cysts' cavities revealed no pathologic findings. At the end of the procedure, a 5F ureteral catheter was inserted into the unroofed cyst to examine the patency of the cyst into the renal pelvis. Next, retrograde pyelography was performed within 5 hours of the procedure, and the ureteral catheter was removed. A follow-up was done at 2 weeks and 3 months postoperatively.
(
Results
No intraoperative or postoperative complications were reported. The operative times were 35 and 30 minutes in patients 1 and 2, respectively. After the procedures, retrograde pyelography showed contrast media filling the parapelvic cyst and the collecting system without extravasation (Fig. 3). The first patient's flank pain was partly relieved. In the second patient, hypertension decreased noticeably (prior to operation: 160/95 mm Hg, and 3 months after the operation: 135/85 mm Hg) and the right flank pain vanished completely. Intravenous pyelography (IVP) and CT images showed objective improvement in hydronephrotic changes (Fig. 4). The patients had no evidence of either any symptomatic or radiographic recurrence at 3 months postoperatively.

Postoperative retrograde pyelography shows filling of cyst after marsupialization.
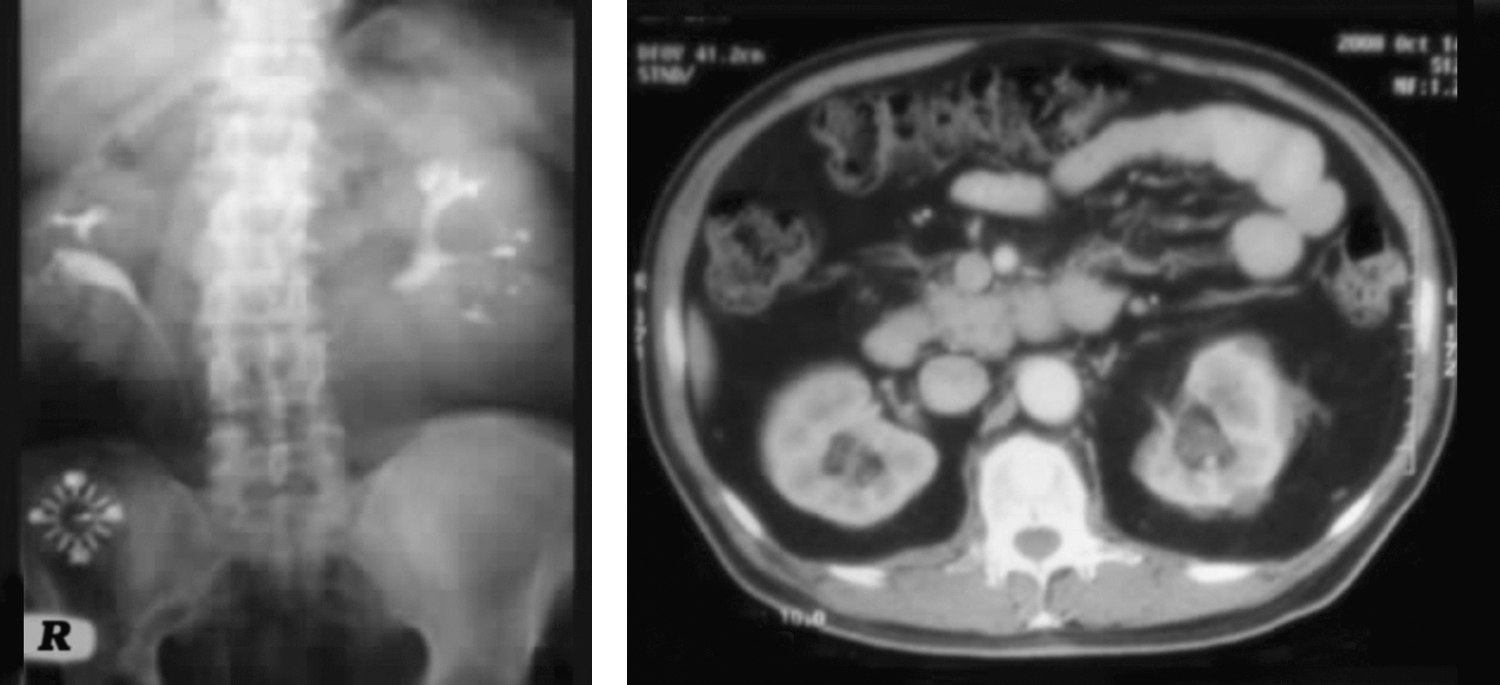
Postoperative CT and intravenous pyelography show improvement of hydronephrosis.
Discussion
Renal cysts are approached using various methods, including laparoscopic unroofing or percutaneous ablation, with varying outcomes. 4 –8 In contrast to the treatment of simple renal cysts, treatment of parapelvic cysts is more difficult. 3 This is due to the proximity of the cysts to the renal hilar structures and the renal pelvis. Percutaneous aspiration can be performed, but it carries extra risk, because of the proximity of the cyst to the renal hilar structures, and is less effective for peripheral cysts. Sclerotherapy is relatively contraindicated because spillage of the sclerosing agent into the retroperitoneum could induce severe perirenal inflammation and secondary ureteropelvic junction obstruction. 9 Rubenstein et al 10 for the first time reported laparoscopic ablation of a parapelvic cyst in 1993. Comparing laparoscopic unroofing of parapelvic renal cysts with the simple ones, they are associated with a greater significant estimated blood loss and operative time and also with a possible increased length of hospital stay. Nonetheless, the complication rates are similar. 7 Laparoscopic unroofing of parapelvic cysts requires advanced surgical skills because of the complexity of the cysts and their proximity to the renal hilar structures and the collecting system. In addition, urinary tract reconstruction may be necessary in cases of inadvertent injury to the collecting system.
Flexible ureteroscopy has been used in other previous studies 11,12 ; however, flexible ureteroscopes are not always available in all centers because of their relatively high purchase cost and their limited life-span. We used the semirigid ureteroscope because of the advantageous location of the parapelvic cyst in relation to the collecting system. This technique, however, may not be possible in all parapelvic cysts, particularly in those situated inferiorly. We concede that the follow-up periods were short in our study and this means that the results have to be considered as preliminary. Considering the aforesaid elaborations, our conclusion is that ureteroscopic treatment is feasible and safe in short term. Further research with longer follow-up periods, however, seems essential to demonstrate the durability of the outcome.
Conclusions
Ureteroscopic treatment using a semirigid ureteroscope is a feasible and safe technique in selected patients with simple parapelvic renal cysts; nevertheless, our follow-up periods were relatively short in our study. Hence, studies with longer follow-up periods are suggested to establish the durability of the outcomes.
Footnotes
Acknowledgment
The authors thank Dr. Mehdi Mansouri for his contribution in composing this article.
Disclosure Statement
No competing financial interests exist.