
Abstract
Introduction:
The obstructed, infected kidney is a urological emergency. It has been accepted that the management of infected hydronephrosis secondary to ureteric stones is through prompt decompression of the collecting system. However, the optimal method of decompression has yet to be established.
Materials and Methods:
A PubMed and Medline search was performed of all English-language articles from 1960 using key words “sepsis,” “urosepsis,” “obstruction,” “obstructive pyelonephritis,” “pyonephrosis,” “infection and hydronephrosis” “decompression,” “stent,” “nephrostomy,” and “management.” The Cochrane database and National Institute for Clinical Effectiveness guidelines were searched using the terms “sepsis,” “urosepsis,” “stent,” “nephrostomy,” or “obstruction.” Scottish intercollegiate guidelines were reviewed and no relevant guidance was identified.
Results:
Two randomised trials have compared retrograde stent insertion with percutaneous nephrostomy with one trial reporting specifically on patients with acute sepsis and obstruction. Neither trial showed one superior modality of decompression in effecting decompression and resolution of sepsis. A further literature search regarding the complications of percutaneous nephrostomy and stent insertion was carried out. An overall major complication rate from percutaneous nephrostomy insertion was found to be 4%, although the complication rates from stent insertion are less consistently reported.
Discussion:
There appears little evidence to suggest that retrograde stent insertion leads to increased bacteraemia or is significantly more hazardous in the setting of acute obstruction. Further region-wide discussion between urologists and interventional radiologists is required to establish management protocols for these acutely unwell patients.
Introduction
The presence of two or more features defines systemic inflammatory response syndrome. 22
It is accepted that the management of infected hydronephrosis secondary to ureteric stones is through prompt decompression of the collecting system. Percutaneous nephrostomy has the advantages of avoiding general anesthesia and instrumentation of the urinary tract. This procedure is performed by either an interventional radiologist, or a trained urologist. However, retrograde ureteric stenting under general anesthesia by the urologist allows internalized drainage, may allow earlier patient discharge, and improves access for later ureteroscopy, if required. Classical urology teaching has suggested that retrograde instrumentation of the infected system is significantly more hazardous than percutaneous nephrostomy, and as such, the percutaneous approach is favored by urologists. 5,6 We reviewed the literature regarding the evidence for the optimal method of decompression for acutely septic, infected hydronephrosis patients.
Materials and Methods
A PubMed and Medline search was performed of all English-language articles from 1960 using key words “sepsis,” “urosepsis,” “obstruction,” “obstructive pyelonephritis,” “pyonephrosis,” “infection and hydronephrosis,” “decompression,” “stent,” “nephrostomy,” and “management.” The Cochrane database and National Institute for Clinical Effectiveness guidelines were searched using the terms “sepsis,” “urosepsis,” “stent,” “nephrostomy,” or “obstruction.” Scottish intercollegiate guidelines were reviewed and no relevant guidance was identified.
Articles regarding decompression of malignant obstruction alone were excluded, along with articles discussing elective stone treatment. Articles were excluded if they were of evidence level 4 (case series) or below. Articles that were single-center series with outcomes for nephrostomy insertion for a variety of indications, rather than just infected obstructed kidneys, were excluded. Single-institution cohort studies and nonrandomized controlled trials were included (evidence level 2b). Decision on inclusion or exclusion was made by the lead author (S.R.). Articles that used nephrectomy as the primary treatment were also excluded.
Results
Only one randomized controlled comparison of percutaneous nephrostomy versus ureteric catheterization specifically in patients with obstruction and infection is reported in the literature (Table 2; Ref. 7 ). This is a well-conducted but small study of 42 patients presenting over a 9-month period to a number of American medical centers. They reported no significant difference in time to definitive drainage, clinical normalization of index parameters (white blood count and temperature), or length of stay (4.5 days in the nephrostomy group vs. 3.2 days in the ureteric catheter group). However, they concluded that ureteric catheterization under general anesthesia was twice costly at $2401 versus $1137 for percutaneous nephrostomy. All patients undergoing nephrostomy had an 8F drain or larger, whereas the majority (80%) of stented patients had a 7F stent. There was no evidence that this increase in size translated into clinically significant increased drainage or an altered clinical course. In this study, no patients had unsuccessful ureteric stenting, although one patient could not have percutaneous access established and required salvage ureteric stenting. Six patients had gross pyuria but numbers were too small for further subgroup analysis.
PCN = percutaneous nephrostomy; WCC = white cell count.
One further randomized prospective study was reported, which comprised 40 patients requiring decompression of hydronephrosis, although only 11 patients in each group had evidence of sepsis at presentation. 8 They reported no failures of access in the percutaneous nephrostomy group, but retrograde stenting failed in 4 of 20 patients. Reason for failure cited in two cases was enlargement of the prostate, and further two patients, both young men, did not tolerate the procedure under conscious sedation. This would not be an issue in regions such as the United Kingdom, where general anesthesia is a standard practice for stent insertion. It is of interest that no stent insertion failed because of an impacted stone or edematous ureter. This study included quality-of-life assessment, and patients in the stent group required more analgesia and had a greater impact on their quality of life. In contrast, 75% of patients with percutaneous nephrostomy required intravenous antibiotics compared with 66% of patients who had a stent inserted. There was no subgroup analysis of the patients with sepsis and obstruction. This study concluded that percutaneous nephrostomy is superior to stent insertion, although it was not clear on what grounds this conclusion was made.
One further retrospective case study assessing the outcomes for patients requiring emergency treatment for infected hydronephrosis associated with upper ureteric calculi as opposed to elective treatment was identified. 9 This nonrandomized study used features of the systemic inflammatory response as outcome parameters and reported no significant difference between percutaneous nephrostomy and ureteric stenting. The numbers were again small, 24 and 35 patients in each treatment group, and there was no information regarding choice of decompression method other than stone size. Stones were significantly larger in the percutaneous nephrostomy cohort (9.7 mm vs. 2.6 mm). This group did not report any decompression failures for either method.
One paper reported successful conservative treatment of concurrent calculi and infection in 11 patients. 10 This was a retrospective audit of 394 patients with urolithiasis, with 11 (2.8%) patients identified as having evidence of urinary tract infection with spontaneous stone passage and improvement on supportive therapy alone. Despite discussion of obstruction with infection in the introduction section, no details were reported regarding the imaging of these patients, or the presence of upper tract dilatation or obstruction. Therefore, this paper was not considered further.
Complications of percutaneous nephrostomy
Percutaneous nephrostomy was first described in 1955. 11 A most contemporary British series 12 reported overall success rates for percutaneous nephrostomy ranging from 83% to 100%, depending on the grade of operator. The most junior trainees had a success rate of 83% overall, although approximately one quarter of the nephrostomies inserted required three or more passes of needle to be successful. They also had higher complication rates of 11% for both major and minor complications, compared with 4% and 2.4% for the specialist uroradiologists. All of the major complications reported were related to hemorrhage. In this longitudinal series which included metastatic obstruction as well as infected hydronephrosis, it is important to note that two patients died of fulminant sepsis, despite decompression by percutaneous nephrostomy.
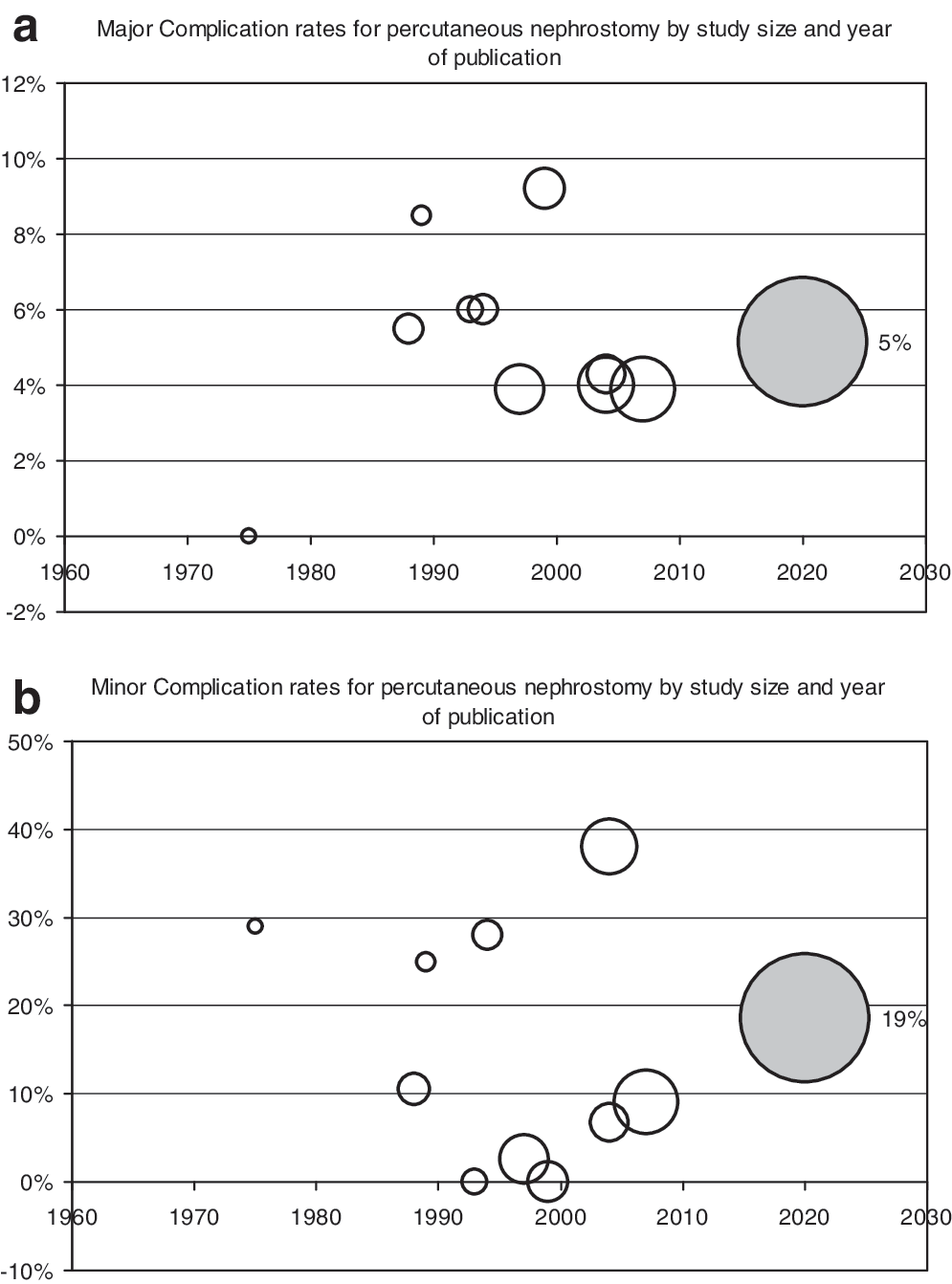
Eight further papers from Europe and the United States reported mostly single-institution series of percutaneous nephrostomy (Table 3, Fig. 1). The incidence of major complications was relatively constant at around 3% to 5% (mainly hemorrhage and pneumothorax). There was more variation in the frequency of minor complications, 6% to 38%, probably because of varying definitions. Currently, the standard of practice is 1% to 4% for hemorrhage and 1% to 9% for sepsis according to the Society of Interventional Radiology, although the American College of Radiology advises that both these complications should be less than 4%.
(
NA = not applicable.
At present, nephrostomy insertion is considered an advanced procedure by the Royal College of Radiologists, advised for Year 4 and 5 training, and not a core competency for all. The Royal College of Radiology specify only 20 to 40 procedures during training to gain basic competency, although previous opinion has suggested that at least 10 to 20 nephrostomies per year are required to maintain competency. 13,14 A survey of working practice for out-of-hours nephrostomy provision in the United Kingdom 15 has reported that nearly one quarter of radiology consultants provide out-of-hours service for nephrostomies despite not routinely performing these during working hours.
Complications of ureteric stenting
Use of a ureteric stent to decompress the ureter was described in 1967, 16 although early stents were far from ideal. One series reported failure of intubation in around 7 of 23 patients with clinical, infected hydronephrosis. 17 Improvements in cameras, fiberoptics, and stent construction mean ureteric intubation and stent insertion are less technically challenging than in the early days of endourology. Currently, the Intercollegiate Surgical Curriculum Program categorizes insertion of a ureteric stent as a surgical training level 2 competency. However, placement of a stent may be challenging in an acutely sick patient with an obstructed and edematous ureter.
Few modern papers detail immediate or acute complications of stent insertion, with only one contemporary study identified in the literature reporting successful stenting rates. 18 This was a prospective series of 92 patients, of which 52 had ureteric obstruction due to calculi, and 9 patients had other intrinsic causes for obstruction. They quoted a success rate for stenting in intrinsic obstruction of 94% but gave no further details of complications relating to stent insertion.
One paper assessing the role of emergency ureteroscopy in a retrospective study of 144 patients with acute colic but no infection was identified. 19 This study reported failure to gain ureteroscopic access in two patients, both of whom required salvage nephrostomy because intramural ureteric inflammation precluded the passage of a guidewire.
The major concern of many urologists regarding stenting is that manipulation of the lower urinary tract during an infective process may cause profound bacteremia and sepsis, whether or not decompression is achieved. The basis for this strongly held belief is unclear given the published evidence. One prospective study of 117 patients analyzing bacteremia and the systemic inflammatory response following elective endourological manipulation of upper ureteric stones reported that procedure type is the major determinant of postoperative pyrexia and endotoxin release. 20 In this study, percutaneous nephrolithotomy carried the highest risk of postoperative systemic inflammatory response syndrome, whereas insertion of a Double-J stent with subsequent extracoporeal shockwave lithotripsy carried the lowest risk.
In contrast to the lack of evidence regarding acute stent complications, the long-term issues of stent morbidity are well reported, 21 along with the requirement for a patient recall system and stent removal at a later date.
Discussion
Only two randomized controlled trials have assessed the optimal method of decompressing infected hydronephrosis in an acute situation. However, as shown in Table 2, the numbers are small, and the outcome measures used in the two trials are heterogeneous. Complications of percutaneous nephrostomy insertion are well reported and relatively consistent (Table 3, Fig. 1), although complications of ureteric stent insertion are less well established. The clinical presentations of infected hydronephrosis can vary widely: from loin pain and positive urine cultures to fulminant sepsis which also hampers meaningful comparison of outcomes.
Based on the available published literature, there is little evidence to support the superiority of percutaneous nephrostomy over retrograde stenting as primary treatment of infected hydronephrosis, despite traditional teaching to the contrary. There is certainly no current evidence of good quality to suggest that attempting ureteric stenting under general anaesthesia is significantly more hazardous than percutaneous nephrostomy in these patients. It also seems unlikely that an adequately powered multicenter randomized trial will ever be carried out to establish the definitive decompression method. Without quality evidence to support one method of decompression over another, urologists and radiologists need to develop algorithms for patients with infected hydronephrosis based on the local availability of out-of-hours theater, interventional team support, and acute care beds. At present, arrangements for decompression of acutely sick patients are relatively informal, with a significant proportion of consultant radiologists not trained in nephrostomy insertion. Options for service provision include contacting colleagues who are off duty to provide the service and interhospital transfer for speciality interventional radiology, which ultimately delays definitive drainage. 15 It has been suggested that urologists should be trained in nephrostomy insertion rather than relying on the relatively smaller numbers of interventional radiologists. The current evidence basis suggests that it may be preferable to have a urologist perform a regularly used skill such as ureteric stenting in the first instance, where patient fitness permits. The capability to place a nephrostomy competently would clearly be advantageous, but it is difficult to see how competency can be maintained for clinicians who do not regularly obtain percutaneous access to the kidney, such as for percutaneous nephrolithotomy. Adopting the “stent first where possible” approach may reduce the requirement for out-of-hours nephrostomy placement in patients with infected hydronephrosis, although clearly it will not eliminate the demand for nephrostomy placement in the most unwell.
Footnotes
Disclosure Statement
No competing financial interests exist.