
Abstract
Objective:
Open partial cystectomy has been used as a curative option for select group of patients with bladder cancer. In recent years, the da Vinci Surgical Robotic System® is being increasingly used to perform complex urologic cancer surgeries. We report first on a consecutive cohort of patients undergoing robotic partial cystectomy (RPC) for bladder cancer.
Methods:
Three consecutive patients underwent RPC, two with diagnosis of papillary neoplasm of bladder and one with urachal adenocarcinoma at our institution from July 2008 to January 2009. Perioperative parameters were prospectively collected and analyzed after Institutional Review Board approval.
Results:
All three patients in the study were men with a median age of 50 years (range, 24–70 years). The RPC was completed transperitoneally in all three patients without the need for open conversion. The operative time, estimated blood loss, and time to hospital discharge for the three patients undergoing RPC were 185, 135, and 165 minutes; 25, 20, and 20 mL; and 5, 2, and 2 days, respectively. The percentage change in hematocrit after surgery was within 5% in all patients. There were no postoperative complications before discharge; however, one patient was readmitted and underwent small bowel resection secondary to bowel obstruction. Final pathology demonstrated high-grade carcinoma pT2bNxMx and pTaNxMx papillary urothelial carcinoma in two patients and invasive adenocarcinoma of the bladder pT3aNxMx in the remaining patient. The median follow-up was 6 months (range, 3–10 months). All three patients were alive with no signs of recurrent or metastatic disease on cystoscopic, cytological, or radiological follow-up.
Conclusions:
RPC is technically feasible using the da Vinci Surgical Robotic System in select patients with bladder cancer without disease recurrence in the short term. A larger cohort with long-term follow-up is necessary to validate our results.
Introduction
Although robotic partial cystectomy (RPC) has been performed for benign tumors, such as pheochromocytoma and bladder leiomyoma, data for its use in malignant disease are limited. Colombo et al 6 reported six cases of laparoscopic partial cystectomy (LPC) for bladder or urachal malignancy performed at three institutions. Another study by Tareen et al 7 reported on RPC in four patients, three for benign disease and one with cancer in the diverticulum. However, there is currently no report on a series of patients undergoing RPC for bladder malignancy. This study establishes the feasibility, safety, and short-term oncological efficacy of RPC in select patients with bladder cancer.
Materials and Methods
Surgical team
A surgical team consisting of well-experienced robotic and laparoscopic urologic oncologist, fellows, and nursing and anesthesia staff trained in DSRS was set up to plan for the study. Patient selection, operative techniques, trouble-shooting methods, and administrative issues were thoroughly discussed and prepared before beginning the study. After discussion of all the risks and benefits of the surgery, including novel application of DSRS technology, all patients provided fully informed consent before surgery.
Study design
After Institutional Review Board approval for the study, three consecutive patients undergoing RPC at our institution between July 2008 and January 2009 were included in the study. Two patients with diagnosis of papillary cell carcinoma and one patient with diagnosis of urachal adenocarcinoma underwent the procedure RPC.
The study included three men with a median age of 50 years (range, 24–70 years). All relevant data were gathered prospectively throughout the study period. All patients had a thorough clinical assessment; either cystoscopic biopsy or transurethral resection of the lesions was used to obtain a pathological diagnosis and for staging. Random bladder biopsies were also taken to identify any concomitant carcinoma in situ elsewhere in the bladder, which were negative in all three patients. Preoperative imaging studies, for example, computed tomography and magnetic resonance imaging (Fig. 2), were used to assess the extent of the primary lesions and the presence of any lymphadenopathy and visceral or bony metastases. In one patient with left lateral wall lesion, a left ureteral stent was placed during initial transurethral resection. In another patient with urachal adenocarcinoma, upper and lower gastrointestinal studies did not demonstrate a concomitant primary. All patients had flexible cystoscopy to confirm location, extent, and size of the lesions just before surgery.
Surgical technique
All procedures were performed using DSRS. Under general anesthesia, the patient was placed in low lithotomy and steep head down position after securing to the table using 2-inch tape. All pressure points were fully padded, and the entire abdomen, external genitalia, and perineum were prepped and draped in a standard fashion. We used the standard five-port transperitoneal approach (Fig. 1). The camera port was positioned at least 1 cm above the umbilicus for papillary lesions and at least 5 cm above umbilicus for urachal adenocarcinoma to facilitate adequate mobilization of the urachal remnant.
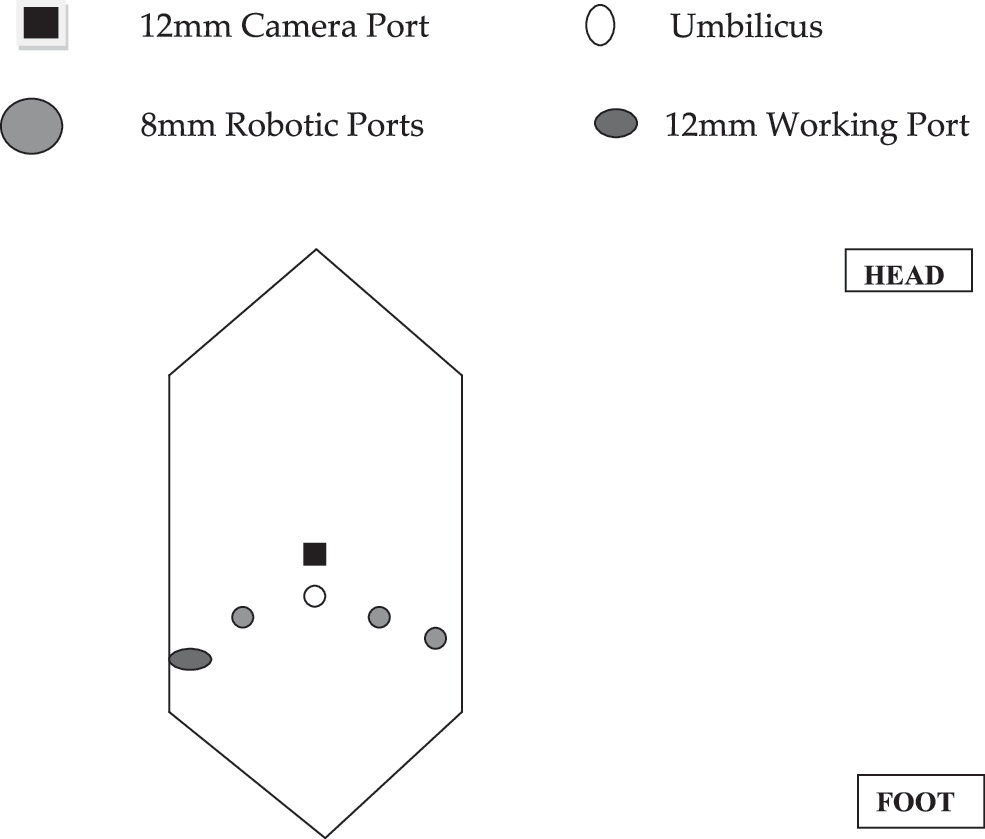
Port placement.

Preoperative (upper row) and postoperative (lower row) imaging studies of respective patients. Arrows show bladder tumors. TCC = transitional cell carcinoma.
The abdomen was insufflated with CO2 injected through a Veress needle inserted through a 1 cm supraumbilical incision. A 12 mm Ethicon® (Ethicon Endosurgery, Cincinnati, OH) port was inserted. Another 12 mm VersaStep® system (One-Step port; U.S. Surgical Corporation, Norwalk, CT) port was placed in the right lower quadrant, about 2 cm above and medial to anterior superior iliac spine. Three 8 mm DSRS working ports, one in the right lower quadrant and two in the left lower quadrant, were placed under direct vision. With all ports in place, the robot was docked. Both the medial umbilical ligaments and the urachus were divided close to the umbilicus, and the bladder was dropped down. A site approximately 2 cm from the presumed edge of the tumor was incised, and the bladder was entered and tumor excised with approximately 2 cm margin. In two of three patients the location of tumor was clearly visible on bladder surface, and we used our best judgment to make initial bladder entry. Once bladder was entered, the tumor was appreciated and adequate margin was obtained using the length of robotic instruments as internal control. In other patient, the bladder was entered at safe distance from presumed site of tumor and satisfactory margin was obtained. Intraoperative frozen section from bladder margins was negative for tumor. The bladder, pelvis, and the abdominal cavity were copiously irrigated using sterile water. The defect in the bladder was closed in two layers using running 2-0 Vicryl, and a watertight anastomosis was obtained. The specimen was placed in an Endocatch® device (U.S. Surgical Corporation) bag and was retrieved intact at the end of the procedure by extending the supraumbilical incision for additional 2 cm. A #19 Blake drain was placed in the pelvis. A slight modification in the port sites was used in patient with diagnosis of urachal adenocarcinoma. We placed the camera port 5 cm above the umbilicus, and remaining ports were placed in similar position as above. Both the medial umbilical ligaments were divided right up to the umbilicus, and the posterior rectus sheath was included in the specimen Fig. 3(4).
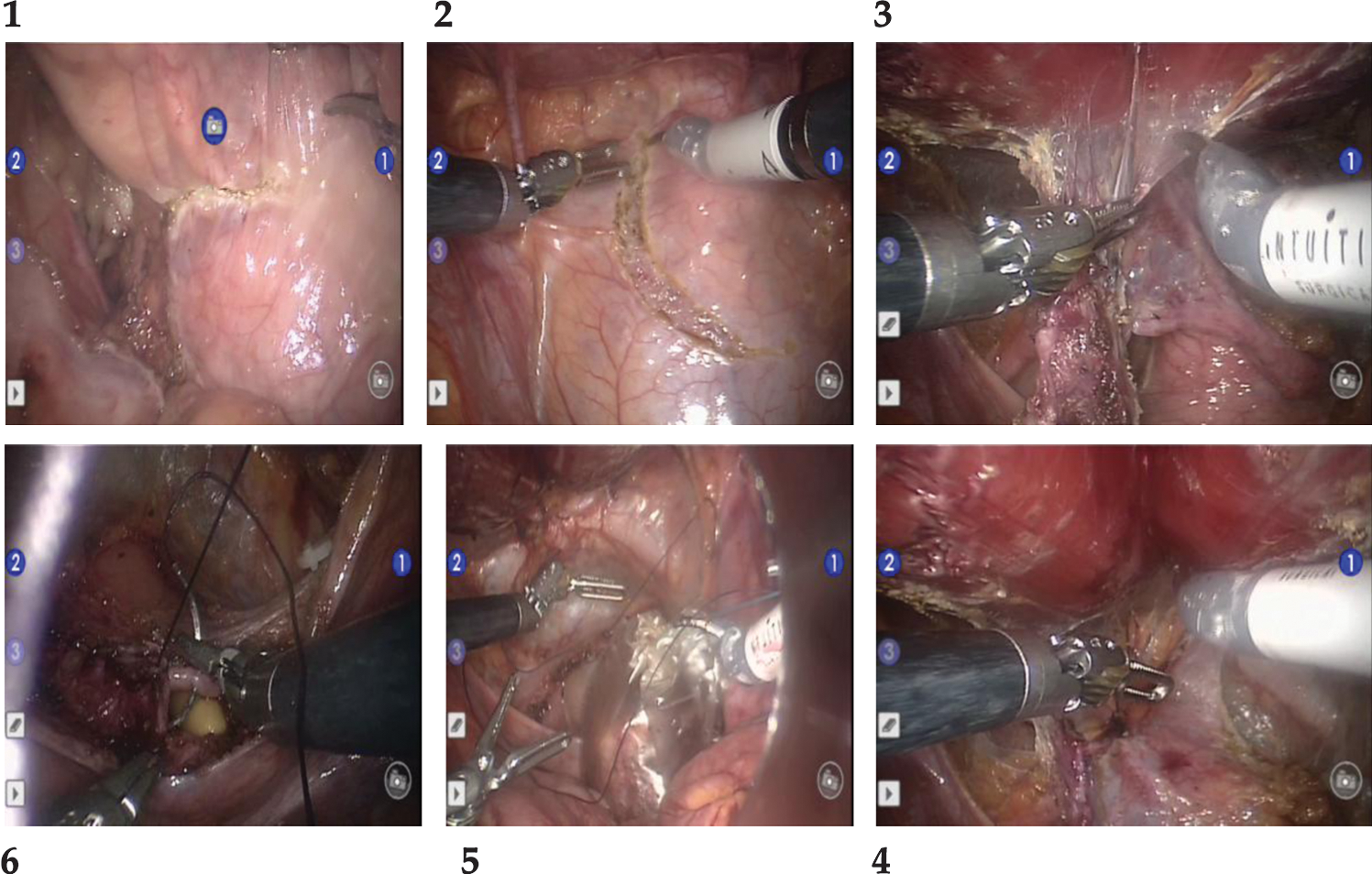
Intraoperative images. In clockwise direction: (
Results
The results are tabulated in Table 1. The RPC was done transperitoneally to mobilize the bladder, excision of tumor, and bladder reconstruction and was performed without the need for open conversion. No perioperative death or complications occurred before discharge; however, one patient was readmitted with small bowel obstruction requiring explorative laparotomy. The median estimated blood loss was 20 mL (range, 20–30 mL), the median operative time was 135 minutes (range, 135–185 minutes), and no intraoperative complications were noted. The median hospital stay was 2 days (range, 2–5 days). In all cases, the indwelling Foley catheter was removed on the 10th postoperative day. Intraoperative frozen section bladder margins were separately evaluated and were found negative for cancer in all cases. The final histopathologic analysis confirmed one case of urachal adenocarcinoma and two cases of bladder papillary cell carcinoma (Table 1). All surgical margins were negative for neoplastic cells. At a median follow-up of 6 months (range, 3–10 months), all three patients were alive with no signs of recurrent or metastatic disease on cystoscopic, cytological, or radiologic follow-up.
Discussion
RPC using DSRS has being increasingly reported. 8 –10 In addition, DSRS has also been used to perform partial cystectomy for benign and malignant bladder disorders. Tareen et al 7 reported RPC for benign bladder and diverticular lesions. The first LPC was described in 1993 by Nezhat and Nezhat, 11 for infiltrating bladder endometriosis. In 2004, Mariano and Tefilli 12 reported their initial experience with LPC for six patients with urothelial carcinoma of the bladder at a mean follow-up of 30 months. Recently, Milhoua et al 13 and Wadhwa et al 14 also reported their experience with LPC in managing urachal adenocarcinoma.
The current study is the first to report on a series of consecutive patients undergoing RPC with adequate short-term oncological follow-up. Partial cystectomy can be performed in select group of patients with bladder cancer. Partial cystectomy preserves bladder function and avoids potential complications of radical cystectomy and urinary diversion, which ranges from 25% to 30%. 15,16 Therefore, partial cystectomy is an attractive option for select patients with invasive bladder cancer, including patients with tumors located at the dome/anterior wall of the bladder, solitary lesions, or tumors confined to bladder diverticulum. 17,18
In our study, we evaluated the technical feasibility of RPC in select group of patients. The distinct advantage of DSRS over conventional laparoscopy is the facilitation of intracorporeal suturing. Although technological advances have been made in laparoscopic surgery, conventional laparoscopy is still limited by lack of three-dimensional vision, poor maneuverability, and ergonomic movement of instruments. 19,20 Robotic technology provides additional dimensions to laparoscopy by adding three-dimensional observation, improving the degrees and freedom of movement, improved ergonomics, stabilization of surgical movements, and ease of intracorporeal suturing. 20,21 The improved technical capabilities are particularly useful during RPC because of the need of precise delineation of tumor margin and intracorporeal suturing including need for ureteral reimplantation in some cases.
Although in our series we demonstrated the feasibility of DSRS in performing RPC, longer follow-up is needed to evaluate tumor recurrence and other potential long-term complications. A potential limitation of partial cystectomy is the risk of recurrence within the bladder, distal ureter, or prostate in men. 22 Two larges series demonstrated a local recurrence rate of up to 35% after open partial cystectomy. However, several of these recurrences were noninvasive in the bladder, which were managed by transurethral resection, and vast majority recurred concurrently locally and distally, resulting in bladder preservation about two-thirds of patients.
In addition to field disease, another risk factor for local recurrence is local spillage of tumor, which is potentially inevitable during partial cystectomy because of transiently open bladder. A detailed review of the literature regarding local recurrence after violation of bladder wall in patients with bladder cancer suggests that extravesical recurrence is extremely rare. In rare cases of tumor recurrence after spillage, progression is usually rapid. Lack of evidence of local recurrence in our study cohort at a median follow-up 6 months suggests that risk of adverse oncological outcome from tumor spillage is potentially minimal. 23 Another area of debate in the field of surgery for bladder cancer is the role and extent of pelvic lymph node dissection. We performed limited lymph node dissection in one patient with muscle invasive bladder cancer, which was negative. Although the current study does not address the issue of pelvic lymph node dissection using DSRS, extended pelvic lymph node dissection is technically feasible using DSRS and commonly performed in other circumstances such as endometrial cancers.
Conclusion
This study demonstrates the technical feasibility and utility of DSRS in performing RPC for bladder tumors. A study consisting of a larger cohort of patients and longer follow-up is needed to validate the utility and establish the oncological outcomes of this technique in patients with bladder tumors.
Footnotes
Disclosure Statement
No competing financial interests exist.