
Abstract
Dissection of the bladder neck is particularly important in patients who have previously had prostate surgery due to hyperplasia. We describe an endoscope-assisted radical perineal prostatectomy (RPP) technique that facilitates the dissection of the prostate–vesical junction. The technique was employed in four patients with a history of transurethral prostate resection. Before dissecting the prostate from the bladder neck during RPP, we circumscribed the bladder neck perurethrally with a Collins knife. The remaining of the RPP procedure was performed via the traditional approach. The incision of the prostate–vesical junction with the Collins knife protected the bladder-neck integrity and made the dissection of this junction easier. The final pathologic diagnosis was organ-confined prostate cancer with negative surgical margins. All the patients had continence during a 6-month follow-up. The major advantage of this technique is to precisely locate the prostate–vesical junction under direct vision. Our modified technique may prove to be a simple, less invasive, and oncologically safe method to manage the bladder neck perurethrally.
Introduction
The introduction of prostate-specific antigen (PSA) screening in the late 1980s has led to significant increases in the detection rate of prostate cancer. Patients usually have their PSA checked during a routine follow-up and are scheduled for a prostate biopsy in case of an elevated PSA level. Unfortunately, 25% to 35% of cancers are missed at the initial biopsy, and most of the patients with a negative first biopsy undergo at least one subsequent biopsy. 1,2 Even in the PSA and prostate biopsy era, the detection rate of prostate cancer by transurethral prostate resection (TUR-P) has been reported to be as high as 18% in unselected patients. 3,4
Active treatment is usually recommended for patients with localized disease and a long life expectancy, with radical prostatectomy being shown to be superior to other treatment options in appropriate patients. 5 However, radical prostatectomy may present difficulties in patients who have previously had TUR-P and is associated with worse outcomes with respect to operative time, length of stay, positive margin rate, and overall complication rate. 6
Radical perineal prostatectomy (RPP) is a minimally invasive and cost-effective surgery that provides good oncological and functional results. 7 However, RPP may be challenging, especially with respect to the dissection of the prostate–vesical junction in patients who have previously had prostate surgery (TUR-P). We describe a novel and practical technique involving an inside approach to the bladder-neck area by a resectoscope dissection, thus allowing easy removal of the prostate and minimizing the potential risks of an incision during the procedure. This endoscope-assisted RPP technique facilitates the dissection of the bladder neck.
Patients and Methods
From March 2003 to May 2009, we performed RPP in 132 cases of localized prostate cancer. Of these, four patients had previous prostate surgery (TUR-P) in the past 10 years. To preserve ureteral orifices, the bladder neck, and urinary continence, we utilized endoscopic instruments in the RPP procedures of these patients.
Technique
The patient is placed in the exaggerated dorsal lithotomy position. Then, an inverted, U-shaped incision is made and the Belt subsphincteric approach is used to reach the prostate. 8 The right angle dissector is passed directly behind the urethra and the urethra is amputated just at its insertion into the apex of the prostate (Fig. 1). Then, the Foley catheter is removed. After division of the urethra, a 24F continuous flow resectoscope with a 30° lens is passed transurethrally into the bladder from the apex of the prostate (Fig. 2). The bladder neck is circumcised perurethrally with the Collins knife (Figs. 3 and 4). After dissection, the anterior bladder neck is opened (Fig. 5). Minimal traction and dissection are applied to the prostate to free it from the bladder. The ureteral orifices are identified, and the rest of the bladder neck is transected. After an 18F Foley catheter is inserted, anastomosis of the bladder neck to the urethra is performed. The remaining of the procedure is completed as described previously. 9,10 Data on these four patients were analyzed retrospectively.

The urethra is cut just at its insertion into the apex of the prostate. White arrow: urethra; black arrow: prostate.
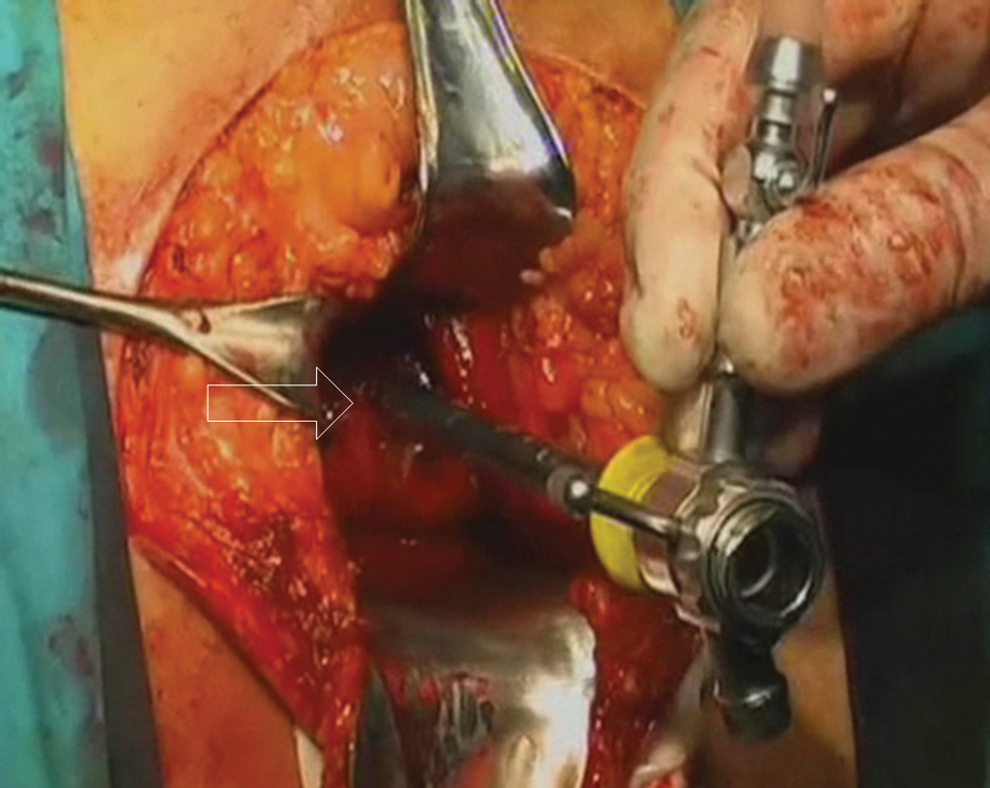
The resectoscope is passed transurethrally into the bladder from the apex of the prostate. White arrow: apex of the prostate.

Endoscopic bladder-neck incision using a Collins knife.

The bladder neck is circumcised perurethrally with the Collins knife. White arrow: circumcised prostate–vesical junction.

After dissection with the Collins knife, the anterior bladder neck is opened. B: bladder; P: prostate; F: Foley catheter.
Results
The incision of the prostate–vesical junction protected bladder-neck integrity and made the dissection of the prostate–vesical junction easier. The mean operation time (135 ± 15 minutes) with this technique was similar to that recorded (125 ± 32 minutes) for the remaining 128 patients. Dissection time for the bladder neck was about 15 minutes. Minimal blood loss was observed during the transurethral dissection. The Penrose drains were removed in the morning of the first postoperative day and the patients were discharged within 48 hours of surgery. The catheter was removed in the clinic on postoperative day 14. The final pathology report was organ-confined prostate cancer with negative surgical margins. All the patients had continence during a 6-month follow-up.
Discussion
The endoscope-assisted RPP technique described provides a practical guide to determine the incision line in the treatment of difficult cases. The primary advantage of this technique is the precise location of the prostate–vesical junction under direct vision. Use of this technique requires skills that are already part of the urological practice. The main disadvantage is that the patient is subject to two different kinds of surgeries on the same day. However, this can be easily accomplished if appropriate preparation for endoscopic and open-surgery instruments is made before surgery. Because endoscope-assisted RPP facilitates bladder-neck dissection, which is the most challenging step in radical prostatectomies, 11,12 this technique can be performed in localized cancer patients who have previously had TUR-P.
Endoscopic approaches have been advocated to assist in seminal vesicle and bladder-neck dissections when observation is poor. 10,13 Teichman et al 13 described laparoscope-assisted RPP. They performed laparoscopy for pelvic lymph node dissection and seminal vesicle mobilization before RPP. The median surgical time for laparoscope-assisted RPP was 237.5 minutes. 13 Later, Ellison et al 10 described another technique to facilitate dissection in RPP. Despite its similarities, there are some major differences in our technique. First, a bipolar transurethral resectoscope was used to manage the bladder neck and seminal vesicles. The grasping forceps, which were introduced via a trocar above the symphysis pubis and passed into the bladder, were used to stabilize the bladder edge of the incision. Ellison et al performed their technique in four human cadavers and then applied it to one patient. The bladder neck and seminal vesicles were successfully dissected in 55 minutes, and the total operative time was 3 hours. 10
As bladder-neck identification and dissection is a difficult step in radical prostatectomy surgeries, various techniques have been developed. 11,12,14 Barre et al 11 improved bladder-neck division in radical retropubic prostatectomy by prior dissection of the seminal vesicles and vasa deferentia. Laparoscope- and robot-assisted laparoscopic prostatectomy (RALP) was also used for bladder-neck dissection. 12,14 Bird et al 12 described a transurethral technique to facilitate laparoscopic identification and incision of the bladder neck. All cases in their series were successfully treated, with clear and sharp bladder-neck margins. 12 Recently, van der Poel et al 14 examined the role of peroperative transrectal ultrasonography for the dissection of the bladder neck during RALP. As peroperative transrectal ultrasonography during RALP decreased the positive surgical margin rate at the base of the prostate, they recommended its use, especially during the initial experience of RALP. 14
The bladder neck is the most distal point of perineal dissection where observation is the poorest. Additionally, it is sometimes difficult to perform bladder-neck dissection in RPP, especially in patients who have previously had prostate surgery. The endoscope-assisted RPP technique appears to be a simple, less invasive, and oncologically safe method to manage the bladder neck perurethrally.
Footnotes
Disclosure Statement
No competing financial interests exist.