
Abstract
Purpose:
To create and evaluate an inexpensive novel model for training in retroperitoneal laparoscopic dismembered pyeloplasty.
Materials and Methods:
The retroperitoneal cavity was simulated by five boards fixed together by detachable hinges; the extent of operating difficulty could be adjusted by changing the angle of inclination. The middle of a plasticine model kidney was imbedded into a metal clip, and a carp swim bladder was fitted to the kidney to model the dilated pelvis. The “ureter” was a 10-cm long porcine ureter. Semicircular-shaped simulator, laparoscopic camera system, scissors, needle holder, and surgical forceps specific for training were used. Ten rounds of intensive training of the “ureteropelvic” anastomosis procedure was provided for five laparoscopic surgeons. Each trainee's mean time of achieving dismembered pyeloplasty in three patients was recorded; the corresponding index in the last three ureteropelvic junction obstruction operations performed by each person before intensive training was retrospectively revised. Subjective evaluation was also performed, and a general self-efficacy (GSE) scale was applied to evaluate the self-confidence of trainees.
Results:
This model reproduced the technical complexity of laparoscopic dismembered pyeloplasty. The operative time significantly declined from 41.84 ± 3.00 minutes to 25.04 ± 2.37 minutes after intensive training. GSE scores after training were also higher than before (27.60 ± 1.14 vs 22.20 ± 1.79). Correlation between operative time and GSE was significant. After training, all participants were more skillful in performing ureteropelvic anastomosis. This is a small study with a middle-term follow-up. The operation also cannot be simulated completely because the ureter is separate from the renal pelvis in the beginning.
Conclusions:
This model demonstrates satisfying fidelity and practicality; it could easily be built and reused, and could result in lower costs than those incurred using the traditional model.
Introduction
The laparoscopic procedure requires considerable skill, has a marked learning curve, and involves longer operative times compared with the open technique. The mean operative time described in four major series of laparoscopic dismembered pyeloplasty was 193 minutes (range 90–480 min); this is much longer than the time needed for open pyeloplasty. 5,6 Thus, a simulator for laparoscopic pyeloplasty and skill training for urologists is necessary initially outside the operating room. Laparoscopic virtual reality simulators are also becoming a ubiquitous tool in resident training and assessment in different specialties in recent years. 7 –9
A valid simulation should provide as realistic an environment as possible; it must mimic the visual-spatial and real-time characteristics of the procedure and must provide realistic haptic feedback. 10 Live animal models have been developed to simulate this challenging procedure; however, these procedures are restricted by high cost as well as by ethical considerations. 11
We describe a simple inexpensive model for retroperitoneal laparoscopic dismembered pyeloplasty and analyze the practical effect of training.
Materials and Methods
The model kidney was made of plastic clay that can be obtained easily in a supermarket (length/width/height: 10/6/6 cm separately); the middle part of the model was imbedded into a metal clip; then a carp swim bladder was fitted to the kidney model by the clip to simulate the dilated pelvis. The model ureter was composed of a 10-cm long porcine ureter (Figs. 1a–1d).
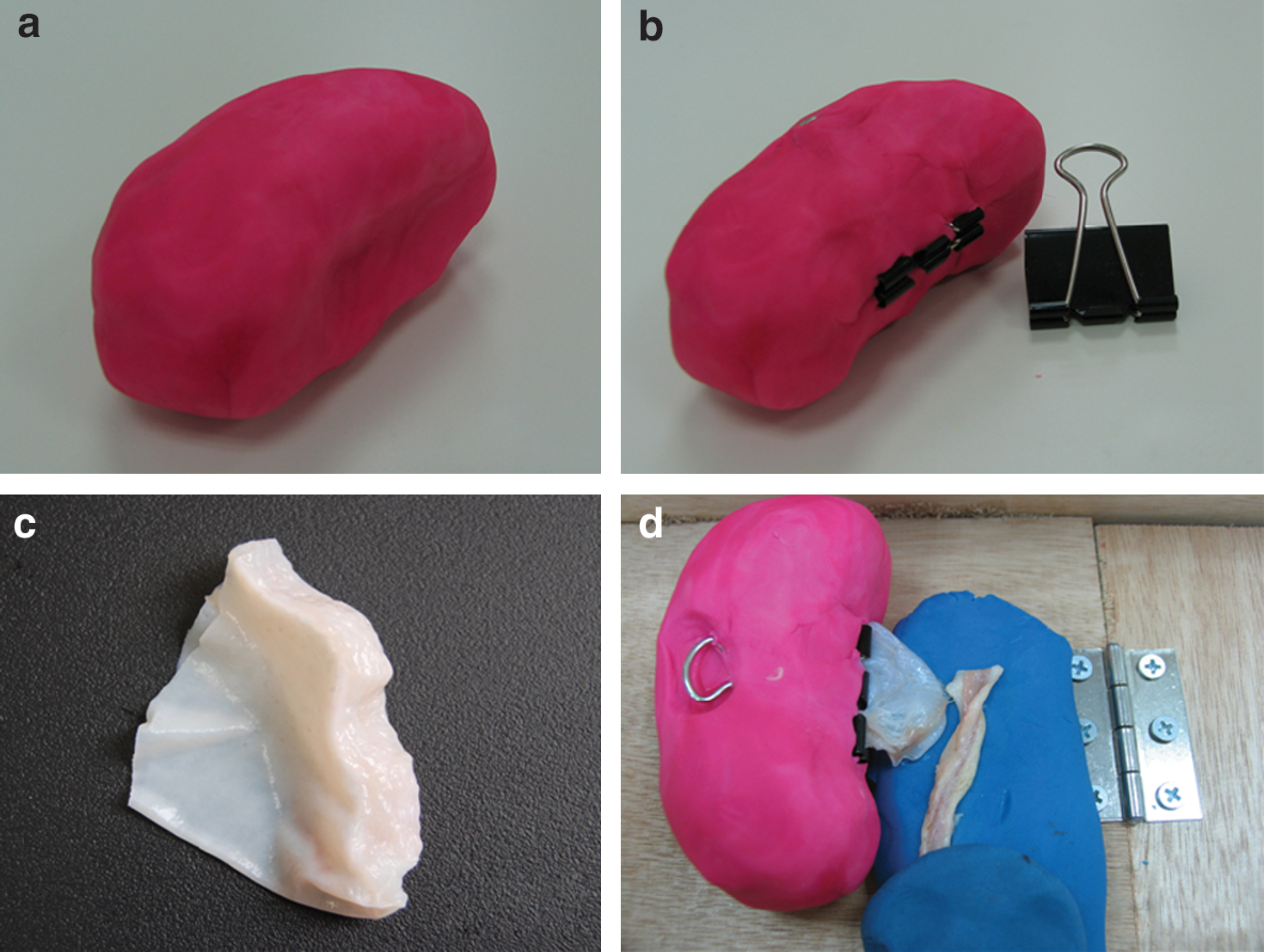
Creating a model for UPJO training. (
The maneuvering space in the retroperitoneum was simulated by five boards. Two laterally placed movable boards, which were fixed by detachable hinges to the base frame, simulated the psoas major muscles and limited the mobility of instruments during a simulated operation. The fixation rod, when placed in the lateral-most keyhole, increased the maneuvering room for instruments and the ease of operation by changing the inclination of the boards through adjustment of the hinges and fixation rods (Figs. 2a–2d). Once the model kidney with dilated pelvis and ureter was moved into the artificial extraperitoneal cavity and fixed by pins, the integrated simulator for UPJO was completed.

Simulating the procedure of retroperitoneal laparoscopic dismembered pyeloplasty. (
Other necessary training equipment included: Semicircular-shaped simulator for laparoscopic training-Universal–Trainer, Storz, Tuttlingen, Germany) laparoscopic camera system (Telepark, Telecam SL 20043020-020, Medipack, Storz) (Fig. 3), one laparoscopic needle holder (Storz), one pair of laparoscopic scissors (Storz), one pair of laparoscopic separating forceps (Storz), and 3-0 polyglactin stitch. Dismembered pyeloplasty, which is a routine procedure used for UPJO in our institute, was performed as the standard procedure during the training course.

The semicircular simulator that was used for laparoscopic training.
The metal clip was released after the last step of training, and the model was removed. Water was injected with a fine needle through the wall of the sutured swim bladder to test for watertightness and for patency of the anastomosis. The swim bladder was then opened to measure the stitch length and to reevaluate the suture quality.
To verify the efficacy of application of this UPJO simulator, intensive training was provided for five laparoscopic surgeons in our institute whose scores on the basic laparoscopic skills test were comparable. In the past 2 years, no less than 10 cases of dismembered pyeloplasty for UPJO had been performed by each of these surgeons.
According to current literature, 12 the learning curve for laparoscopic surgeons generally reaches a plateau after about 8 repetitions; therefore, 10 repetitions in 5 days were necessary in our intensive training. The “ureteropelvic” anastomosis was performed according to the standard operation steps. All trainees were asked to accomplish eight stitches of simple interrupted suture when reconstructing the ureteropelvic junction (UPJ), with four anterior and four posterior sutures (Fig. 4).

Close view of the ureteropelvic junction obstruction simulator shows that the model simulates the procedure of ureteropelvic anastomosis very well; the suture is sturdy when the posterior part of pelvis and ureter was sutured together.
In the next 6-month period, 15 patients with UPJO and with moderate hydronephrosis assessed by B ultrasound and intravenous urography (IVU), a moderate somatotype of body mass index of 24 to 28, and without crossing vessels confirmed by CT angiography were randomly assigned. Each trainee's mean time of achieving dismembered pyeloplasty after training in three patients was recorded; then, we revised the corresponding index in the last three UPJO operations performed by each person before intensive training. This was done retrospectively by video, and the mean was used in the comparison.
Two blinded experts independently assessed the extent of hydronephrosis before operation and exposure before dismembered pyeloplasty for each patient by reading the IVU film, the intravenous CT scan, and the live video of the operation.
Subjective evaluation was also performed, and a general self-efficacy (GSE) scale, including a 10-item questionnaire, was applied to evaluate the self-confidence of the trainee.
The median follow-up time was 7.1 months (range 6–9 mos). Perioperative and midterm complications were recorded.
Statistical analysis was performed with the SPSS 11.0 software package. Results were reported as mean ± standard deviation; correlation analysis of GSE and operative time were also evaluated.
Results
The extent of hydronephrosis before operation and exposure before dismembered pyeloplasty for each patient are comparable, according to two blinded experts' independent assessment.
All surgeons were more skillful in dismembered pyeloplasty after intensive training than they were before. Mean operative time was significantly shorter after training (Table 1). GSE score after training was also higher than before (Table 2). Correlation between operating time and GSE was significant (correlation coefficient: −0.959).
GSE = general self-efficacy.
Regarding the subjective evaluation, all surgeons felt more confident on finishing this advanced laparoscopic procedure and more relaxed during the operation after intensive training had taken place.
A postoperative complication of an instance of prolonged urine leakage was noted in one patient in group A. All patients in groups A and B with an obvious UPJO on excretory urography before surgery demonstrated symptom relief and an improvement of renal function on diuretic renography at a minimum follow-up of 6 months. A case with mild restenosis in the UPJ was observed in group A (Table 3).
Discussion
Since the initial description of laparoscopic nephrectomy by Clayman and colleagues 13 in 1991, there has been a dramatic increase in the use of laparoscopic surgery in urology. Laparoscopic reconstructive techniques, however, such as laparoscopic pyeloplasty or ureteral reimplantation, represent an increase in the complexity of laparoscopic surgery. Because of this, laparoscopic reconstructive techniques are still not universal in many hospitals.
Despite its difficulty, different techniques and approaches of pyeloplasty have been applied laparoscopically. The transperitoneal approach has the advantages of a larger working space and readily identifiable anatomic landmarks. Access to the renal pelvis, however, necessitates considerable mobilization and retraction of the overlying loops of bowel.
The retroperitoneal approach has the perceived disadvantage of a somewhat limited working space and absence of readily identifiable intra-abdominal anatomic structures. The retroperitoneal approach, however, has the advantage of greater familiarity, better detection of crossing vessels, direct and rapid access to the UPJ, and less risk of ileus. 14
In expert hands, retroperitoneal laparoscopic pyeloplasty is still preferable to open surgery because of the high success rate and low complication rate. 15 For residents, however, the issues are how to acquire advanced laparoscopic reconstructive skills and how to shorten the learning curve. Adequate operating table practice is the best way to develop expertise, but good simulation training and experienced laparoscopic teachers are also helpful for the students.
An ideal model should provide haptic feedback to the trainee and should closely mimic the true operative environment; convenience and cost should also be taken into consideration. Current training models can range from live animals to simulators. The use of live animals can provide the sufficiently realistic simulation to a trainee for issues such as pneumoperitoneum, blood circulation, bleeding, tissue manipulation, and anatomic environment. 11,16,17 Cost and ethical considerations, however, limit the use of live animals.
Ramachandran and coworkers 18 described a simple model for laparoscopic pyeloplasty using the crop and esophagus of a dead chicken. This is a low-cost, easily available model that can give a more realistic feel of the tissue and anatomy. It cannot, however, simulate the retroperitoneal cavity and reflect these difficulties.
The difficulty of retroperitoneal laparoscopic pyeloplasty may be that it requires a more delicate technique to perform this procedure in so small a space. To our knowledge, there is no workable simulation model for the retroperitoneal approach at the present time. Inspired by modeling-clay toys, we constructed a high-fidelity UPJ model in which we used plastic clay and metal clips to simulate the kidney and the inner membrane layer of a swim bladder to simulate the dilated renal pelvis. Based on our study of surgical videos, we designed a special wooden box with movable boards that could limit the mobility of the laparoscopic instruments and thereby adjust the ease of operation; this more closely mimics the actual surgical environment.
Because of the diversity of patients and the unstable technical conditions of the surgeons, it is very challenging to evaluate the operating skills of the surgeons in a real operational environment. Our primary results, however, proved the effectiveness of this model to a certain degree.
All trainees undertook 10 repeated trainings in 5 days, and their anastomosis time decreased significantly in later operations. Furthermore, our study showed that intensive training in this simulator can enhance the self-confidence of trainees; this may be conducive to finishing the procedure successfully. Regardless of other factors, such as the interaction between training effect and self-confidence, operative time is negatively correlated to GSE. This also indicates that simulator training improves the trainee's skill comprehensively.
Indeed, the most important question about the value of simulation in procedural training on UPJO is whether such educational interventions can ultimately be beneficial for improving patient outcomes. It is very difficult, however, to design an impeccable control study to prove the effect of this model because of the lack of a suitable live animal model and relatively rare clinical cases. In addition, it is restricted by ethics of the beginners as a training target.
Our study has some shortcomings, such as lack of long-term study, small sample, and inevitable interference factors. Based on these results, however, we still believe that this is a new, available simulator and can improve laparoscopic education.
During these training courses, we also found some important shortcomings of this model. (1) The operation cannot be simulated completely because the ureter is separate from the renal pelvis in the beginning. (2) The internal lining of the swim bladder does not contain muscle fiber and is not as tenacious as the renal pelvis. It is easily torn if the needle is improperly pulled out. Hence, a smooth suture is recommended. (3) During the operation, the modeling plastic clay is likely to stick to the instruments; this affects the procedure when the instruments touch the kidney model. (4) Because all the swim bladders and ureters should be fresh, it is difficult to obtain the raw material.
Conclusion
In a small study sample, our novel model for training in retroperitoneal laparoscopic pyeloplasty demonstrates a satisfying fidelity and practicality and may be more helpful for beginners. It could be built easily, and most of the elements can be reused time after time. Of course, a larger study sample and long-term follow-up would be necessary to confirm our results more conclusively.
Footnotes
Disclosure Statement
No competing financial interests exist.