
Abstract
Background and Purpose:
The injection of dextranomer/hyaluronic acid (DHA) has become an accepted treatment for children with vesicoureteral reflux (VUR). Complete ureteral duplication has been considered by some practitioners as counterindication for its use. We reviewed the Texas Children's Hospital (TCH) records for children with complete ureteral duplication who were treated with DHA for VUR.
Methods:
We searched medical records at TCH for patients with a preoperative diagnosis of complete ureteral duplication who had undergone DHA injection between January 1, 2001, and October 15, 2008. Operative notes, imaging studies, and clinic notes were reviewed.
Results:
In this period, 28 kidneys in 24 children were treated. The average grade of reflux before injection was 3.44 (range 1–5). First injection resolution of reflux was 57% with an increase to 73% after a second injection with an average volume of DHA of 1.05 mL. New contralateral VUR developed postinjection in three (15%) children with unilateral VUR. There were no perioperative complications. The average age of the children who were treated was 41.4 months. Mean follow-up was 45.94 months. Success of DHA injection tended to be higher in girls (65%) and older children.
Conclusions:
High levels of success can be achieved with DHA injection in children with complete ureteral duplication. DHA injection is more likely to be successful for older girls with VUR and complete ureteral duplication. If initial injection does not result in VUR resolution, a second injection offers an opportunity for improved success. For physicians and families who are seeking an alternative to open surgical management, DHA represents an attractive option for selected children with complete ureteral duplication.
Introduction
Methods
We reviewed a prospectively collected database, approved by an Internal Review Board, that contained the clinical information of children who were undergoing DHA treatment for VUR over the last 8 years at Texas Children's Hospital (TCH). Only children with a preoperative diagnosis of complete duplication based on imaging and chart notes were included in the evaluation. Children with partial duplication or one ureteral orifice on the affected side were excluded from analysis. Children with untreated voiding dysfunction were excluded from the analysis.
Patient demographics were compared for age and gender. Clinical parameters, including preoperative VUR grade, side of VUR, length of follow-up, results of postoperative imaging, presence of new contralateral VUR, presence of previous or treated voiding dysfunction, and the presence of previous urinary tract surgery, were evaluated. Operative findings that were evaluated included the amount of DHA injected, technique of injection, and ureteral configuration after injection.
Once reflux had been considered resolved, families were instructed to call the clinic or return for a visit if urinary tract infection (UTI) developed. Follow-up was determined based on time from surgery until December 2008. Success was defined as no VUR on postinjection cystography. Children with resolved VUR who returned with a febrile UTI underwent repeated cystography to evaluate for recurrent VUR.
Results
A total of 28 ureters in 24 children were identified. Four patients had bilateral refluxing duplicated systems, 11 had right-sided only, and 9 had left-sided only. Average age at the time of surgery was 41.39 months (7–175 mos). Average follow-up was 45.94 months (5–73 mos). No child had voiding dysfunction in this series, and three had previous urinary tract surgery.
Average preoperative reflux grade was 3.44 (1–5) (Fig. 1). Reflux occurred into both the upper pole and lower pole moieties in 5 ureters, upper pole in only 2, and lower pole in the remaining 21 ureteral units. Average amount of DHA injected was 1.05 mL, and postinjection ureteral configuration was available in 24 ureters. Of the 24 patients, 22 did achieve a mound configuration, with the other two resulting in a bilobed configuration. All orifices were coapted after injection.
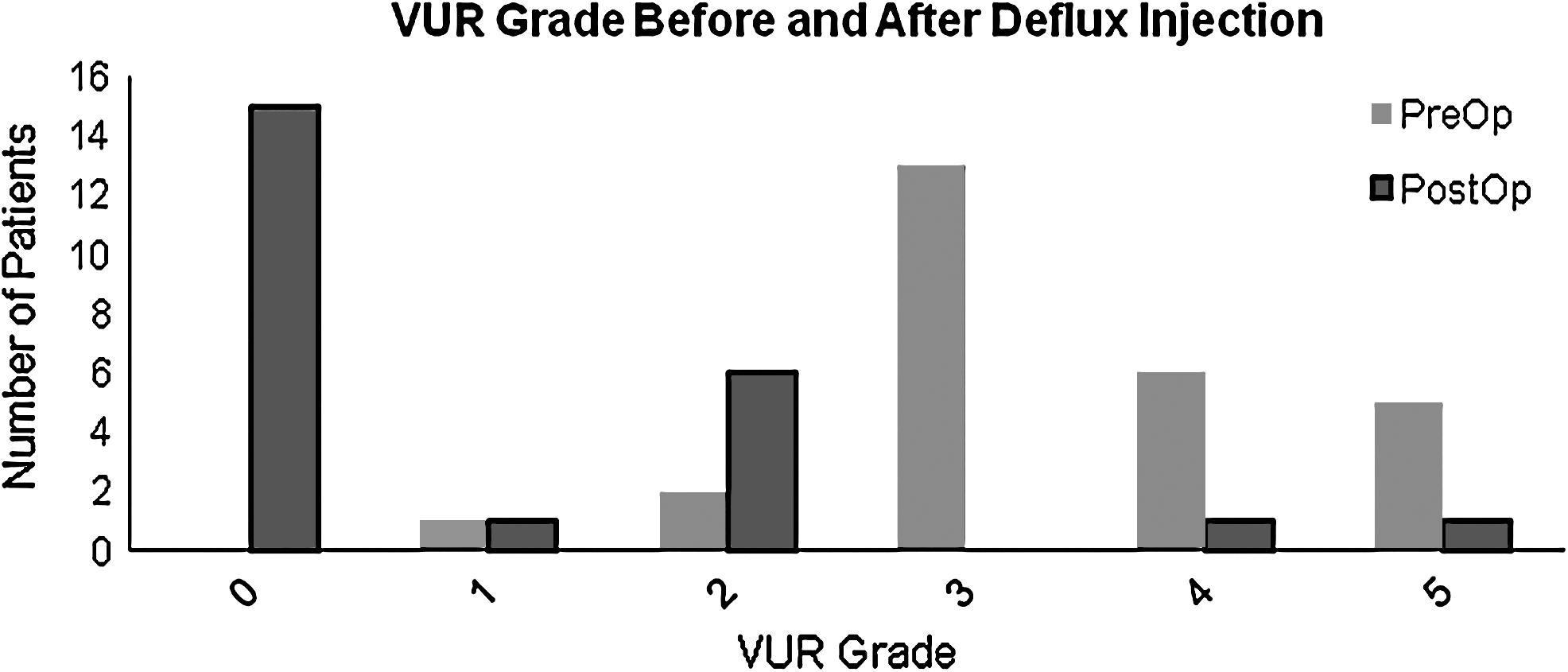
Comparison of preoperative and postoperative vesicoureteral (VUR) grade among patients who were undergoing initial deflux injection into duplex systems.
Results on postinjection voiding cystourethrography showed complete resolution of VUR in 57% of ureters (Fig. 1). Eight of nine patients underwent repeated injection for persistent VUR. Four of the eight had complete resolution of VUR after the second injection. One child underwent a third injection with resolution of VUR on postinjection imaging, and one child underwent ureteral reimplantation after the initial injection failed to resolve VUR. Overall resolution of reflux in our patients was 73% after up to two injections.
The success rate was higher in older children vs younger children (Fig. 2). The average age in the successes was 47.7 months; in the failures, it was 30.7 months (ns). Success rate in females after one injection was 65% compared with 3% in the males (ns) (Fig. 2). When comparing injection technique, the subureteral transurethral injection technique had a success rate after a single injection of 75%, and the hydrodistention implantation technique had a success rate of 60.0% (ns) (Fig. 2). Success was highest in children whose indication for surgery was parent preference or failed ureteral reimplantation and much lower when the indication was breakthrough UTI while the patient was receiving antibiotics prophylactically (Fig. 3). Preoperative grade of VUR did not correlate with success. VUR grade 3 had the worst success (46.15%) while every other grade had a success rate greater than 75% after a single injection (Fig. 4).
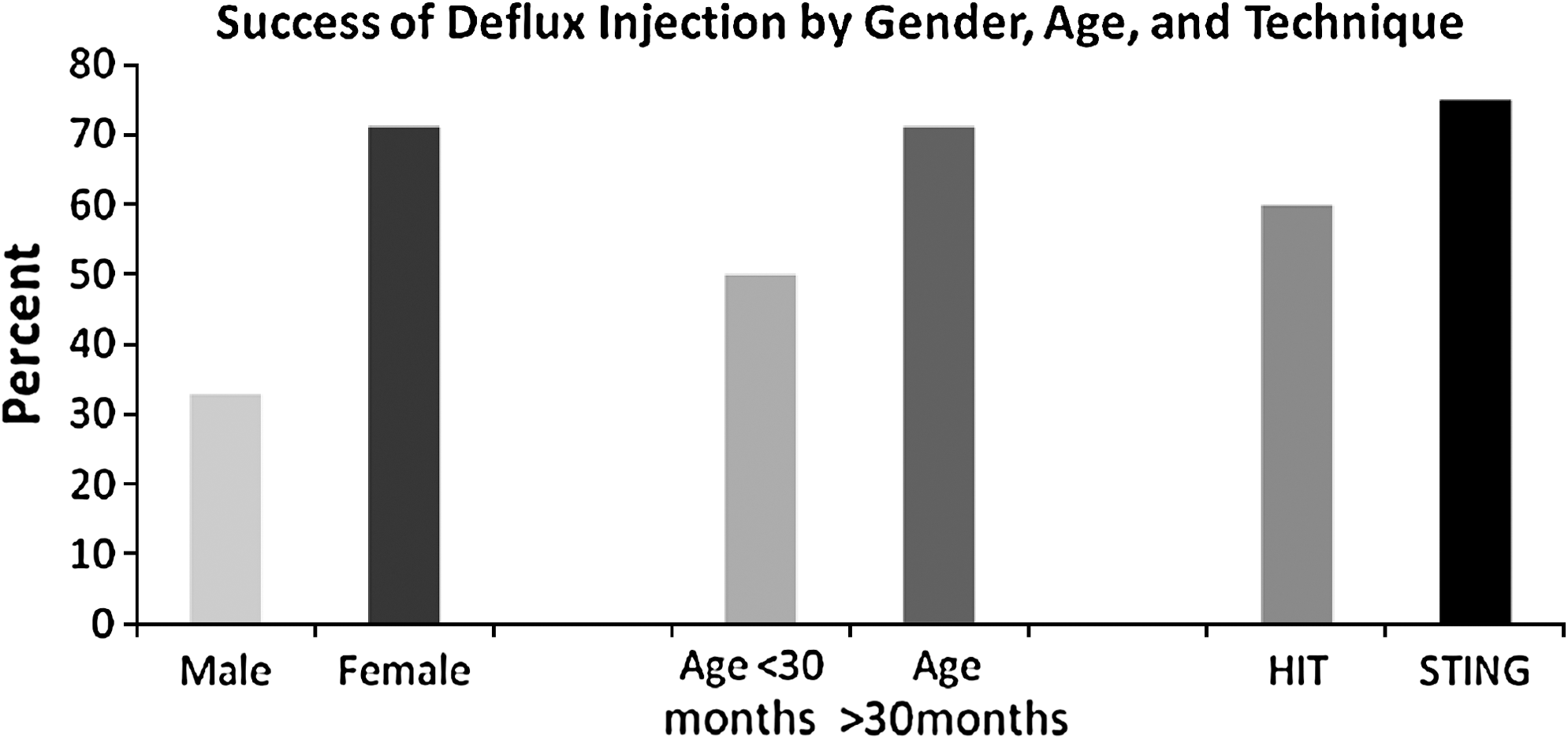
Success of deflux injection when compared for gender, age, and technique used. HIT = hydrodistention implantation technique; STING = subureteral transurethral injection.

Success per injection by varying indications for surgery. UTI = urinary tract infection; VUR = vesicoureteral reflux.

Success of first deflux injection by preoperative vesicoureteral reflux (VUR) grade.
Contralateral development of new reflux on postoperative imaging occurred in three patients (15%). Two had grade 2 VUR and one had grade 1. All three patients have been observed, and one has had spontaneous resolution of the VUR, reducing the overall rate of contralateral VUR to 10%.
Discussion
DHA has quickly emerged as many surgeons' treatment of choice for primary VUR. 8 Most of the initial experience has focused on VUR in children without complex congenital anomalies. Only a few articles have focused on outcomes of DHA injection in children with complex urinary tracts. 4 –7 In our analysis, we focused specifically on children with complete ureteral duplication anomaly and VUR into one or both moieties.
The surgical treatment of children with reflux into a duplex system has traditionally been common sheath ureteroneocystotomy or ureteroureterostomy with solitary ureteroneocystotomy. Success rates of well over 90% have been achieved in published series. 9 –11 During the early experience with DHA, most authors focused on uncomplicated reflux and considered a duplication anomaly to be a contraindication to treatment, favoring instead open surgery. Recently a few authors have reported their experience with complex urinary tract anatomy and DHA treatment. 4 –7
When compared with single system, DHA success rates for duplex systems is lower. This is shown in our study and by others. Many articles represent success after up to three injections, and we were also able to continue to achieve VUR resolution with our single patient who received a third injection.
Given the morbidity of an open operation, the risk to the ureters from either a common sheath ureteroneocystotomy or a unilateral ureteroureterostomy with ureteroneocystotomy, and difficulty of reoperation in the setting of complications, DHA offers a nice alternative for the management of VUR. It has a shorter convalescence time, there are few complications, and the bladder is left in a way that allows for traditional open surgery should DHA fail. Others have reported that ureteroneocystotomy is not significantly impacted after DHA, and the same should hold true for duplicated systems after DHA injection.
A number of interesting factors also arose from our review of the data that are difficult to explain. It seemed that younger children and males had worse outcomes and the children with breakthrough UTI did worse when compared with children whose parents chose surgery to stop antibiotic prophylaxis.
This raises a number of questions. Do boys with VUR in duplex systems have worse outcomes because they have higher grade VUR, are younger, or both? While the average age of the failures was more than a year younger than the average age of those in the success group, the failure group was comprised of mostly boys. While we cannot separate these two factors, it suggests that this population may be better served with a reconstructive procedure over DHA injection. Other authors have looked at these variables in the setting of single system VUR and have found on univariate analysis that both male gender and younger age are significant predictors of failure of DHA injection. 12
While these variables did prove significant on multivariable analysis, the results are intriguing. In almost all series published on using DHA for VUR, the younger age and male gender seem to always have poorer success rates. 12 –14 It would seem that if larger studies or compilations of studies were to be analyzed, it is possible that these factors would be determined to be significant.
There are a number of limitations to this study. First, the treatment for these patients was directed by the operating surgeon and parent preference. Randomization with larger numbers to DHA or ureteroneocystotomy would be a better study design, although difficult to enact. Second, the sample size is small. This may reflect the relative rarity of ureteral duplication or, conversely, that most of the ureteral duplications anomalies were managed through a different surgical approach or through observation. Despite the small sample size, we were able to show both safety and efficacy. Third, although we did account for the volume injected, there was not uniform recording of mound configuration, which is an important factor for predicting the success of DHA injection.
Finally, the success rate for DHA injection is defined differently than success after open or laparoscopic ureteroneocystotomy. In the endoscopic injection, most authors continue to define success as resolution of reflux after two or three injections. Success after open or laparoscopic surgery is defined as the resolution of reflux after a single procedure with persistence of reflux being a failure. These divergent definitions of success make comparisons between reconstructive and DHA treatments difficult. It is therefore not possible to recommend one treatment over the other but more accurate to portray DHA as a safe and viable treatment option in children, especially older girls, with VUR and complete ureteral duplication anomalies.
Conclusion
DHA can be used for management of VUR in renal units with complete ureteral duplication anomalies. Success rates may be improved with repeated injection and low morbidity for the child. Factors that influence success are older age at time of injection and female gender. Consideration for reconstruction should be given to young boys with VUR in the setting of complete ureteral duplication.
Footnotes
Disclosure Statement
A. Bayne, no competing financial interests exist; D.R. Roth, Oceana Therapeutics, instructor of technique.