
Abstract
Objective:
The objective of this study was to compare the results of antegrade (AG) ureteral stenting with retrograde (RG) stenting during laparoscopic dismembered pyeloplasty.
Materials and Methods:
Between October 2003 and April 2007, a case series of 47 laparoscopic dismembered pyeloplasties were done by three surgeons of equal expertise in laparoscopic surgery, where the Double-J ureteral stent was placed by the RG method (RG stenting group) in 15 cases and by the AG method (AG stenting group) in 32 patients. Intraoperative findings and operative data were recorded. Clinical and radiological outcomes were evaluated during the follow-up visits at 3, 6, 12 months and then annually.
Results:
Differences in patient's age and body mass index were not statistically significant. Laparoscopic pyeloplasty was successfully completed in 45 patients, with two cases of conversion to open (one in each group). A crossing vessel was identified in 42% of RG stenting group versus 45% of AG stenting group. A state of high ureteral insertion was identified in 16% of AG stenting group, a finding that was never seen in RG stenting group. Mean operative time was 271 ± 21 minutes for RG stenting group versus 199 ± 34 minutes for AG stenting group, a difference that was statistically significant (p ≤ 0.01). Differences in estimated blood loss, hemoglobin decline, time to oral feeding, duration of urethral catheter, and length of hospital stay were not significant. Postoperative complications were seen in two patients: postoperative hematuria belonging to RG stenting group was managed endoscopically and prolonged urine leakage belonging to AG stenting group ceased spontaneously by postoperative day 8. Clinical and radiological improvement was evident in 97%, with a mean follow-up of 30 ± 17 months.
Conclusions:
AG ureteral stenting is technically feasible and provides better dissection, especially in patients with high ureteral insertion and secondary ureteropelvic junction obstruction, with good long-term outcome in both groups.
Introduction
Laparoscopic dismembered pyeloplasty is a well-established procedure in the treatment of ureteropelvic junction obstruction (UPJO) since its early descriptions in 1993. 1,2 Classically, the Double-J stent is inserted in a retrograde (RG) manner before starting the procedure. Antegrade (AG) stenting is rather an unpopular method being described in only three reports. 3 –5 Although the description of the technique is well established in these three reports, technical failures in terms of stent malposition were defined, and impact of AG stenting on the operative time was analyzed; in none of these reports a follow-up beyond 3 months was mentioned. 3 –5 In this study, we are comparing the results of AG stenting to the RG stenting in a case series of laparoscopic dismembered pyeloplasty, stressing on the intraoperative differences and long-term outcome (with a mean follow-up period of 30 ± 17 months).
Technique
Patients
Between October 2003 and April 2007, laparoscopic dismembered pyeloplasty was performed in 47 patients in a single center; the procedure was performed by three surgeons of equal expertise in laparoscopic surgery. The RG stenting group included the first 15 cases in which the Double-J stent was placed endoscopically in a RG fashion before starting the procedure. The AG stenting group included the remaining 32 cases in which the Double-J stent was placed intracorporeally during the procedure in an AG fashion. The protocol of this study was reviewed and approved by the hospital review board and the patients agreed to participate in this study. Patients' demography is illustrated in Table 1. The type of UPJO was primary in the RG stenting group, whereas in the AG stenting group, the type of UPJO was primary in 29 patients and secondary in 3 patients (two cases after failed trials for open pyeloplasty and one case after an open pyelonephrolithotomy). There was no clear randomization in our series; we began our practice with laparoscopic pyeloplasty by RG method in patients with primary UPJO only (patients with secondary UPJO were considered exclusion criteria during our early experience) until we encountered technical difficulties in placing the Double-J stent by the RG method. For this, we explored the feasibility of AG stenting in laparoscopic pyeloplasty to overcome such technical difficulties. We were even able to perform laparoscopic pyeloplasty in patients with secondary UPJO, and since then, we were convinced by the effectiveness of AG stenting. Preoperative work-up included serum creatinine and urine analyses, abdominal ultrasonography, intravenous urography (IVU), and/or diuretic renography (Tc99m-labeled diethylenetriamine–pentaacetic acid or mercaptoacetyltriglycine). These assessments were repeated during the follow-up visits at 3, 6, 12 months and then annually. Data were recorded and analyzed using Excel XP (Microsoft, Redmond, WA). The Student's t-test was chosen for making the univariate analysis, with the p-value of <0.05 as a statistical significant value.
Patients' Demography, Intraoperative Findings, and Operative Results in Both Groups
NA = not assessed; UPJO = ureteropelvic junction obstruction.
Operative details
Port arrangement
The patient is placed in the flank position with 45° to 60° lateral inclination. The transperitoneal approach is advocated using three to four ports. The first trocar is a 10-mm trocar at the umbilicus for the zero-degree telescope; the second (5 mm) and third trocars (10 mm) are placed more laterally (8–10 cm from each others) to make an isosceles triangle with the first trocar. Occasionally, a fourth trocar is placed in the flank for assistance.
Steps of pyeloplasty
In RG stenting group (15 patients), the patient was first placed in the lithotomy position to place a Double-J stent endoscopically in a RG manner and then repositioned in the flank position to place the ports (as previously described). Conversion to open was done in one patient because of inability to pass the Double-J stent across the ureteropelvic junction during the initial cystoscopy. Reflection of the whole colon was done to expose the Gerota's fascia, which was incised to expose the lower pole of the kidney, the renal pelvis, and the proximal ureter. Once the ureteropelvic junction was identified, it was freed from its surrounding adventitia. An anterior crossing artery was identified in six patients of the RG stenting group (42%). The ureter was sharply transected, taking care to not cut through the Double-J stent, and it was spatulated laterally for a 2 cm distance. Next, the renal pelvis was spatulated medially and reduced. The site of the new ureteropelvic junction was selected at the most dependent point of the renal pelvis and was performed with free-hand intracorporeal suturing using 3-0 or 4-0 polyglycan suture (Vicryl® SH-plus needle, Ethicon, Johnson & Johnson Medical Ltd., Somerville, NJ). In patients with anterior crossing vessel, the new ureteropelvic junction was reconstructed anterior to the crossing vessel. Anastomosis was made in running fashion, starting with posterior suture line and followed by the anterior suture line. By the end of the procedure, a 16F tube drain was placed through the lowermost trocar site, and a urethral catheter was placed in the bladder for 6 days to promote the drainage of the renal pelvis.
In the AG stenting group (32 patients), the laparoscopic procedure was carried out without placing a ureteral stent. As such, the renal pelvis remained distended and was easily observed underneath the mesentery of the colon, even before starting colon dissection. Because of this, the colon was mobilized only for a short distance, enough to expose the dilated renal pelvis and the ureteropelvic junction (omitting the need for whole colon mobilization). An anterior crossing artery was identified in 14 patients (45%), and a state of high insertion of the ureter was identified in 5 patients (16%). The site of the new ureteropelvic junction was selected at the most dependent point of the renal pelvis while it was still fully distended. Next, the ureter was sharply transected and spatulated.
At this stage of the procedure, an appropriate Double-J stent was selected according to patient's height and was prepared on the instrument's table. The Double-J stent was mounted over its guidewire and excess length of the guidewire was cut off so that it would extend for only 3 to 4 cm on either side of the Double-J stent. It was then introduced totally into the abdominal cavity through the 10-mm trocar or the cannula of the suction device, to be inserted in the spatulated ureter until its upper end. The guidewire was withdrawn while holding the upper 1 to 2 cm of the Double-J stent with a nontraumatic grasper. Observation of urine efflux from the upper end of the Double-J stent is crucial to ensure its proper descent in the bladder; for this reason, the urinary bladder was filled with 100 to 150 mL saline prior to Double-J stent insertion to keep the bladder half-full.
After insertion of the Double-J stent, spatulation of the renal pelvis was made along its medial aspect to reconstruct the new ureteropelvic junction in the same manner described with patients in the RG stenting group. Conversion to open was done in one patient of the AG stenting group after placing the Double-J stent because of inability to complete the new ureteropelvic junction laparoscopically. The cause was a malfunction of the needle holder, which occurred after taking the lower stay suture (the spring of the needle holder broke and the needle holder could not hold the needle steadily anymore), and thus conversion to open was necessary to complete the ureteropelvic anastomosis.
Postoperative care and follow-up
A plain X-ray and abdominal ultrasonography were done postoperatively to confirm the correct position of the Double-J stent. Analgesia was given upon request, using nonsteroidal anti-inflammatory drug (usually a single dose of Diclofenac sodium 75 to 150 mg intramuscularly), which was sufficient during the first 1 to 2 days. The urethral catheter was removed by postoperative day 6 to be followed by the drain. The Double-J stent was endoscopically removed after 4 to 6 weeks. A pyeloplasty is defined by the absence of flank pain, absence of pyuria, and good pyeloureteral drainage in the follow-up IVU (Fig. 1), and/or the renogram of the affected kidney (Fig. 2). On the other hand, failure is defined by persistence of symptoms, concurrent urinary tract infection, deterioration of the renal function, and/or radiological evidence of obstruction in the IVU or renogram, any of which would require another intervention to revise the UPJO.
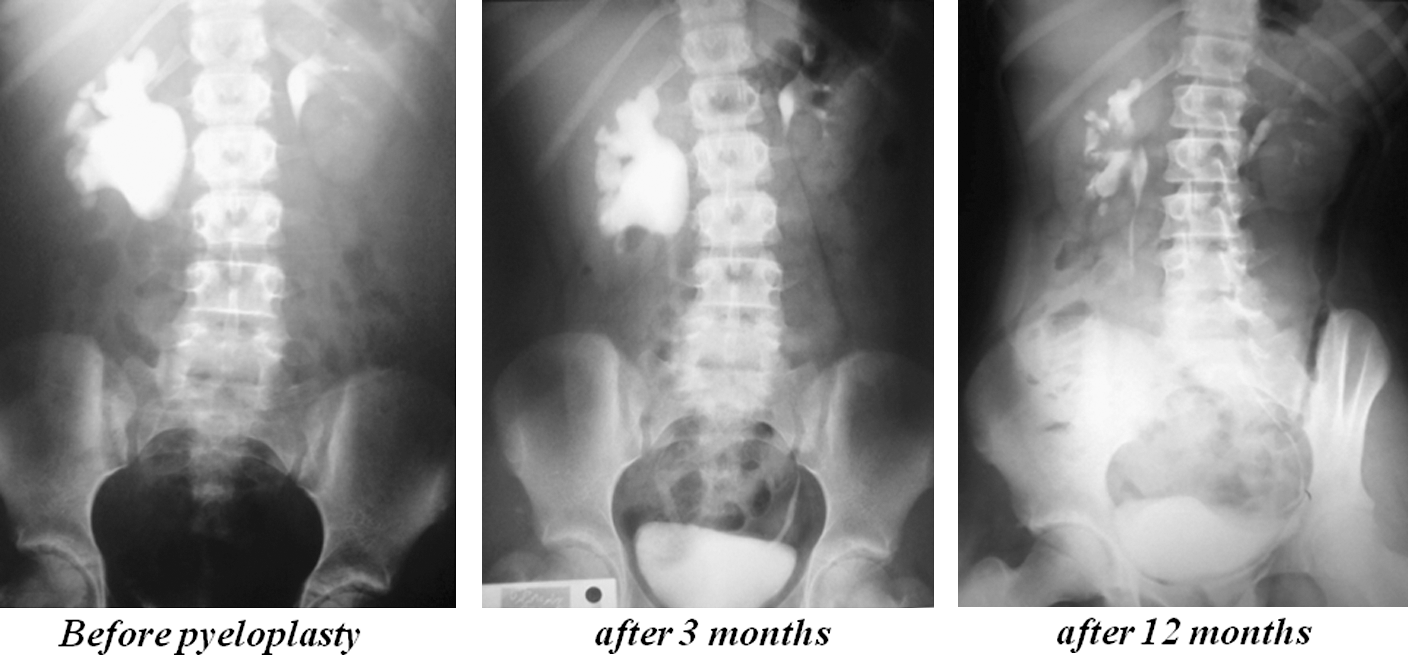
Serial intravenous urography before and after pyeloplasty.
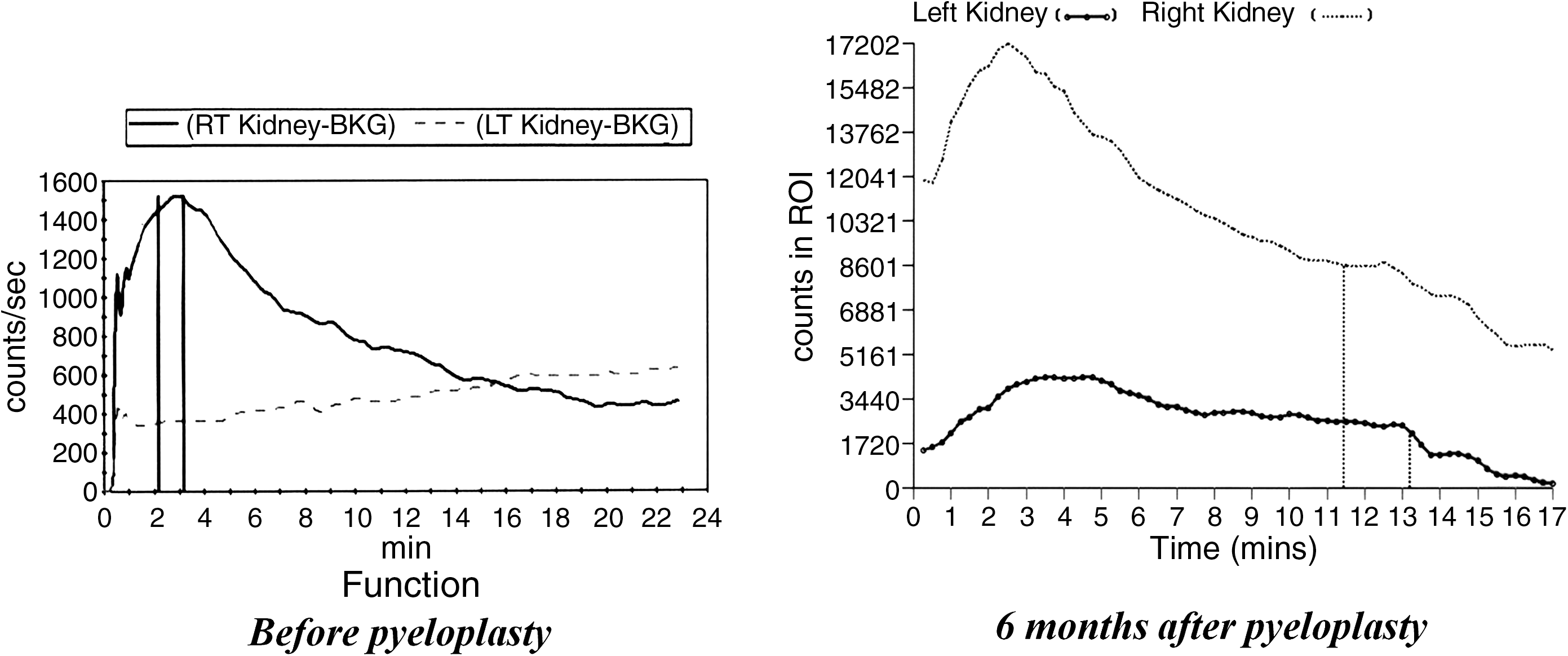
Serial renogram before and after pyeloplasty.
Results
Pyeloplasty was completed laparoscopically in 14 of 15 cases in the RG stenting group and in 31 of 32 in the AG stenting group, with a single case of conversion to open in each group. The results of both groups (after exclusion of the two cases of conversion in both groups) are illustrated in Table 1. Differences between both groups in terms of age (26 ± 9 vs. 24 ± 10 years; p = 0.6) or body mass index (28.9 ± 2.9 vs. 27.1 ± 3.6 kg/m2; p = 0.2) were not statistically significant. The mean operative time was calculated from the time of insufflation till the closure of port sites (not including initial cystoscopy or repositioning of the patient in the RG stenting group). For the RG stenting group, it was 271 ± 21 minutes versus 199 ± 34 minutes for the AG stenting group, a difference that was statistically significant (p ≤ 0.01). The mean operative time for the Double-J stenting in the AG stenting group was 8 ± 3 minutes (range, 2–12 minutes). Other differences in both groups in terms of mean blood loss (44 ± 12 vs. 55 ± 26 mL; p = 0.1), hemoglobin decline (0.2 ± 0.1 vs. 0.1 ± 0.2 g%; p = 0.2), regain of intestinal sounds (11 ± 2 vs. 12 ± 5 hours; p = 0.6), and hospital stay (7 ± 2 vs. 6 ± 1 days; p = 0.1) were not statistically significant. Postoperative complications were seen in two patients and they were classified according to the modified Clavien system. 6 In the RG stenting group, one patient suffered from postoperative hematuria by postoperative day 5, with radiological evidence of blood clots within the renal pelvis. CT scan and angiography did not reveal any potential source for bleeding. A diagnostic percutaneous nephroscopy was made to evacuate the blood clots where it revealed a small spurter at the suture line and it was controlled by electrosurgical cautery. Hematuria ceased afterward and the nephrostomy tube was removed by day 14 (Grade 3b). In the AG stenting group, one patient suffered from prolonged urine leakage from the drain, starting from postoperative day 1. The urethral catheter was left in place to promote drainage of the renal pelvis, where urine leakage continued till day 8 before it ceased spontaneously (Grade 1). The urethral catheter was kept for another 6 days before it was removed by postoperative day 14.
Follow-up was done for both groups, with a mean duration of 30 ± 17 months (range, 7–57 months). The two cases of conversion were excluded from follow-up. Another 6 patients were missed in the follow-up, leaving 39 patients who were the followed up with a response rate of 86% at 3 months (39/45 patients), 86% at 6 months (39/45 patients), 75% at 12 months (33/45 patients), 15% at 24 months (7/45 patients), and 6% at 36 months (3/45 patients). Based on the criteria used to define a pyeloplasty, 38 patients have shown both radiological and clinical improvements, with one case of failure in the RG stenting group, estimating an overall 97% success rate for both groups (95% for the RG stenting group and 100% for the AG stenting group). This patient was an early case of the RG stenting group, who suffered from recurrence of flank pain after the removal of the Double-J stent, with radiological evidence of obstruction at the new ureteropelvic junction. The patient was subjected to percutaneous endopylotomy to manage his state of re-stenosis (Grade 3b).
Discussion
Is it better than RG method? Efficacy of laparoscopic pyeloplasty described with RG stenting is well established in several comparative studies having both objective and subjective outcomes similar to that described for a standard open pyeloplasty. 7 –9 In general, our results for both groups are comparable to other reports of laparoscopic pyeloplasty in the literature, whether with AG 3 –5 or RG stenting. 7 –17 In terms of the effect of AG stenting on the operative time, our results are in accordance with those of Arumainayagam et al. 5 In our view, intraoperative findings found with AG stenting were more important to us than reducing the operative time. During pyeloplasty whether in open or laparoscopic pyeloplasty, RG Double-J stenting is associated with losing the peculiar anatomy of the UPJO because of the drainage of the renal pelvis. This is especially true in situations such as high insertion of the ureter, in which drainage of the renal pelvis would mask the most dependent point of the renal pelvis. A state of high insertion of ureter was identified in five patients (16%) of the AG stenting group, a finding that was never identified in the RG stenting group. One of those five patients identified with high insertion of ureter was recurrent after a previous open repair. In this particular case, we believe that the cause of recurrence was failure to identify the condition of high insertion of the ureter and deal with it in the first place rather than a tight ureteropelvic junction. Thus, it is possible to avoid recurrence in a number of patients that would result from missing a state of high insertion of the ureter. AG stenting have shown a number of advantages. It omits the need for cystoscopy and RG Double-J stent fixation. It allows an easy identification of the renal pelvis and proximal ureter and limits colon dissection. We were able to perform the technique in three patients with secondary UPJO. In our hands, it would be difficult to dissect and find the renal pelvis among the dense adhesions of the previous surgery if it was not distended.
Is it difficult? To the best of our knowledge, AG ureteral stenting is described in detail in only three reports. 3 –5 The first was made by Mandhani et al, 3 who performed laparoscopic pyeloplasty in 23 of 24 patients in the AG stenting group versus 19 of 21 patients in the RG stenting group. The cause of failure in the AG stenting group was related to stent malposition through the suture line, requiring stent repositioning. Although the steps of the procedure were described in detail, only the operative time of stent placement in both groups was mentioned and follow-up was done for 3 months. 3 The second report was made by Chandrasekharam 4 in children (mean age, 1.5 years), where AG stenting was achieved in 14 of 17 (82%) patients versus 24 of 25 children in the RG group. The cause of failure in AG stenting in the three patients was related to inability to cross the ureterovesical junction. Although pyeloureteral drainage was achieved in both groups by 3 months, the author did not recommend AG stenting in children because of its technical failures. 4 More recently, Arumainayagam et al 5 reported AG stenting in 45 patients, with two cases of stent malposition. In their report, the impact of type of stenting and surgeon experience was statistically analyzed, where it was significantly shorter for AG stenting (185 vs. 245 minutes with a p-value of <0.0001) and independent on surgeon's experience. 5 So far, we have not encountered any technical problems in AG Double-J stent fixation in our patients. The safety profile in both groups is acceptable and conversion rate is comparable in both groups. Even the case of conversion reported in the AG stenting group was related to instrumental malfunction rather than a failure of the technique. Long-term follow-up has been assessed in our patients, with a mean duration of 30 ± 17 months in both groups, showing an overall 97% success rate for both groups, which is comparable to those of open or other reports of laparoscopic dismembered pyeloplasty. 7 –17
We realize the limitations of this study. The impact of AG stenting on operative time in our study group is baised by the nonrandomized pattern of this study, and the relatively small number of study group, and thus we cannot exclude the learning curve effect. On the other hand, this study provides intraoperative findings and a long-term outcome that have never been reported in any of the previous reports of AG stenting.
Conclusions
AG ureteral stenting is technically feasible and safe and maintains the anatomy of the renal pelvis for better dissection, especially in patients with high ureteral insertion and secondary UPJO. Radiological and clinical follow-up have yielded satisfactory long-term results in both groups.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
A video demonstrating this technique is available online at