
Abstract
Objective:
The objective of this study was to evaluate the efficacy of TachoSil® (Nycomed UK, Oxford, Buckinghamshire, UK), a hemostatic sponge, to seal major collecting system injuries (in addition to providing an adjunct to hemostasis) after partial nephrectomy in a porcine chronic survival model.
Materials and Methods:
Laparoscopic upper-pole partial nephrectomies were performed in 10 farm pigs (>40 kg). After hilar clamping, an energyless incision was made at a point halfway between the hilum and the upper pole of the kidney and the collecting system was opened widely. TachoSil was applied to cover the defect; 15 to 20 minutes after the application of TachoSil, the hilar clamp was removed, hemostasis confirmed, and the pig survived. Assessment was made for hematoma and urinoma. Four weeks postoperatively, the pigs were euthanized. Ex-vivo retrograde studies were performed to assess collecting system leak. Weight, blood pressure, estimated blood loss, the weight of the partial and completion nephrectomy specimen, presence/absence of urinary leak on retrograde study, histopathologic findings, and complications were recorded.
Results:
All pigs survived. Mean warm ischemia time was 18 minutes, mean blood loss was 90 mL, and mean resected weight was 13.7 g. There was no evidence of leak on retrograde study. Histologically, nonspecific changes were noted in all specimens, which included dystrophic calcification, scarring, and areas of fibrosis at the partial nephrectomy surgical margin.
Conclusion:
TachoSil seals the collecting system after partial nephrectomy on a porcine chronic survival model, in addition to providing an adjunct to hemostasis. More studies, including human trials, are warranted to evaluate this observation further.
Introduction
There is a lack of consensus regarding the optimal method of hemostatic control during laparoscopic partial nephrectomy (LPN). Further, one of the challenges of LPN is the repair of a collecting system injury. Although suture repair works effectively in many cases, it requires precision suturing against the ticking clock of warm ischemia.
Tissue sealants are substances that bind tissues together and serve as a barrier to leakage through polymerization. These compounds have been used to effect hemostasis and for tissue coverage to prevent urine leakage. The most common sealants in clinical practice today are fibrin sealants, cyanoacrylates, polyethylene glycol polymers, and collagen-based adhesives.
TachoSil® (Nycomed UK, Oxford, Buckinghamshire, UK) is a hemostatic sponge, approved for use in open surgery. It consists of a collagen patch, coated with fibrinogen and thrombin coagulation factors (Fig. 1). We had evaluated its use during LPN in an earlier study with an acute porcine model 1 and developed a mechanism for introducing the sponge into the laparoscopic field. Unlike other liquid sealants such as FloSeal® (Baxter, Deerfield, IL), TachoSil is a sponge that molds itself to amalgamate with the cut surface of any bleeding organ. We hypothesized that the use of TachoSil could help repair collecting system injuries in addition to providing an adjunct to hemostasis in a porcine chronic survival model and thereby determined if it provides efficient and effective control of bleeding as well as urinary leakage after LPN.

TachoSil packing and appearance.
Materials and Methods
The protocol was designed as a nonrandomized, nonblinded test of the study hypothesis, using 12 juvenile pigs, with each animal serving as its own control. The protocol was approved by the Animal Research Ethics Committee of the Faculty of Health Sciences, and the study was supervised by an independent veterinarian.
The following parameters were recorded: Body mass, blood pressure (by arterial cannulation) during the procedure, intraoperative blood loss (suction at operative site measured), the mass, dimensions, and histology of the partial nephrectomy specimen, warm ischemia time, and TachoSil application time. Full blood count, serum urea, creatinine, sodium, potassium, chloride, and bilirubin at surgery (day 0) and on days 1, 3, 5, 7, and 28 after surgery. Any complications in the 4 weeks postoperatively. Mass of the kidneys, radiological imaging to assess the integrity of the renal collecting system, and histopathological examination of the kidneys removed at termination of the study on day 28.
Each pig was anesthetized using ketamine 20 mg/kg by intramuscular (IM) injection and insertion of an intravenous (IV) cannula in the ear with administration of physiologic saline, thiopentone 3 to 5 mg/kg, and pancuronium 0.3 mg/kg IV. The animal was intubated and ventilated with 40% oxygen and 1% halothane. Antibiotic prophylaxis was provided in the form of amoxicillin 20 mg/kg IV at operation and 20 mg/kg 12-hourly IM for 5 days. Analgesia consisted of buprenorphine 0.3 mg IM preoperatively and twice daily postoperatively for 3 days.
Pneumoperitoneum was achieved through a Veress needle inserted in the umbilicus. After achievement of 12 mm Hg intraperitoneal pressure, the Veress needle was withdrawn, and a 12-mm laparoscopic port (VersaSTEP; Covidien, Norwalk, CT) was inserted at this same location for the 30° laparoscopic camera. Under visual control, three additional 5-mm VersaSTEP ports were inserted to complement the camera port.
The pig was then placed in a modified right lateral position (about 45° of inclination). Using sharp dissection, the ascending colon was reflected medially, exposing the right kidney. The renal pedicle was dissected free, keeping the kidney in its normal position in the retroperitoneum. Warm ischemia was created using a vascular sling to occlude the renal artery and vein en masse. An energyless upper-pole partial nephrectomy was performed with endoscopic scissors. The right kidney was incised at a point halfway between the hilum and the upper pole of the kidney; the renal parenchyma in this area was removed, and the collecting system was opened widely. TachoSil was applied to cover the defect for a period of 10 to 15 minutes, after which the vascular occlusion sling was removed and hemostasis confirmed (Fig. 2). The 10- to 15-minute time interval was based on our earlier experience, because no other reported work with TachoSil has been carried out in this setting. An Endocatch® (Covidien) bag was used to retrieve the partial nephrectomy specimen. The ports were removed under direct vision, and fascial closure was carried out for the 12-mm port, whereas all 5-mm ports were closed with skin approximation using absorbable sutures. No surgical drains were placed.

TachoSil applied to kidney after partial nephrectomy.
The animals were housed in pairs in pens in the animal research facility. They were visited twice daily by one of the researchers and continually monitored by the full-time animal facility staff for any signs of distress, agitation or debilitation (e.g., failure to eat and drink or move about normally), or abdominal distention.
At 4 weeks postoperatively, each animal was sedated with ketamine 20 mg/kg IM and euthanized by IV injection of sodium pentobarbitone 200 mg/mL. Laparotomy was performed to excise both kidneys with the ureters, after which ex-vivo retrograde studies were performed to assess collecting system leakage. A 5F catheter was placed into the ureter, radiological contrast medium tinted with methylene blue was injected at pressure up to 60 cm water, and an X-ray was taken. The kidneys were then bivalved and placed in formalin for histopathologic examination.
Statistical analysis was performed using Instat® (GraphPad Software, La Jolla, CA) software with Student's t-test for parametric data and Spearman's rank test for correlation analysis. A two-tailed p-value of <0.05 was accepted as statistically significant. All data are shown as mean ± standard deviation and range.
Results
The mean systolic and diastolic blood pressures at the start and end of the procedure were not significantly different (Table 1). The mass of the kidney removed during heminephrectomy, the renal ischemia time, the TachoSil application time, and the measured blood loss are shown in Table 1. TachoSil had to be applied twice in two pigs to ensure hemostasis.
Parameters Studied During the Laparoscopic Partial Nephrectomy Procedure (Day 0) and at Termination (Day 28)
Significantly different from day 0.
Significantly different from right kidney.
Two animals died during induction of anesthesia, one presumably because of an anaphylactic reaction to IV injection of amoxicillin and the other because of failure to achieve endotracheal intubation. All 10 animals that underwent LPN survived until termination on day 28.
The mean body mass of the pigs was significantly greater at day 28 compared with day 0, and the mean mass of the left kidney was significantly greater than that of the right kidney. However, the mean mass of the right partial nephrectomy specimen on day 0 plus the mass of the right kidney on day 28 was not significantly different from the mass of the left kidney on day 28 (Table 1).
The mean hemoglobin level increased significantly on day 1 compared with day 0, but returned to the baseline level by day 5, and on day 28 it was again significantly higher than on day 0 (Fig. 3).
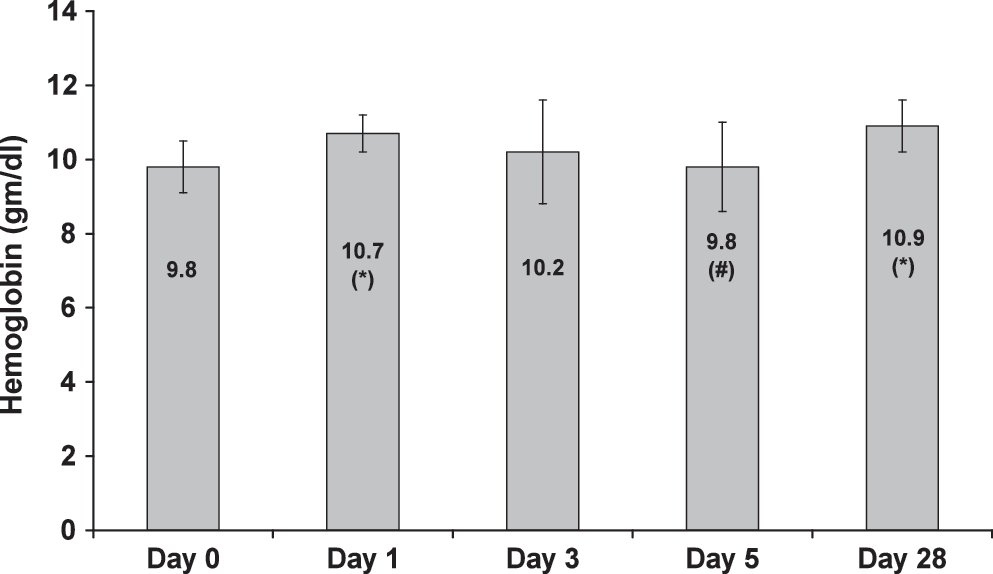
Hemoglobin at the start of the procedure (day 0) and at days 1, 3, 5, and 28 after the procedure. *Significantly different from day 0. #Significantly different from day 28.
The mean serum urea increased significantly on day 1, but returned to baseline level on day 3. On day 28 it was significantly higher compared with day 5, but not compared with day 0 or 3.
The mean serum creatinine was significantly higher on days 1 and 3 compared with day 0, but on day 5 it was not significantly different from the level on day 0. On day 28 it was significantly higher compared with days 0 and 5, but not significantly different from the level on days 1 and 3 (Fig. 4).

Serum creatinine at the start of the procedure (day 0) and at days 1, 3, 5, and 28 after the procedure. *Significantly different from day 0. #Significantly different from day 5. @Significantly different from day 1.
There was no statistically significant correlation between warm ischemic time and serum urea or creatinine levels, or between the mass of renal tissue removed and urea or creatinine levels (Spearman's rank correlation test).
The mean white cell count, serum sodium, chloride, potassium, and bilirubin did not vary with statistical significance during the study period.
In six pigs there were small amounts of free peritoneal fluid found at postmortem examination. Fluid urea and creatinine did not differ significantly from serum levels.
During the ex-vivo retrograde pyelogram studies, there was no visible leakage of methylene blue from any kidney. Radiological imaging showed pyelotubular backflow of contrast in most kidneys, but no leak (Fig. 5); however, an area of subcapsular extravasation was seen in one of the right kidneys.

Retrograde pyelogram at high pressure showing pyelotubular backflow of contrast. Note the smaller right kidney with absent upper-pole calix.
Histologically, all left kidneys and the lower poles of the right kidneys consisted of normal renal tissue. At the right partial nephrectomy surgical margin, there was scar formation in all specimens, with histological features of interstitial fibrosis, focal areas of necrosis or infarction, and dystrophic calcification. One kidney was reported as containing an upper-pole cyst with clear fluid and fibrinous exudate.
Discussion
Although LPN is now generally considered to provide excellent disease control in the management of small volume renal tumors with much less morbidity than its open counterpart, its main limitation remains the difficulty of achieving adequate hemostatic control easily. Largely, hilar clamping and specimen excision followed by suture closure of the defect is the accepted method of choice. However, a number of animal studies have been carried out with various products to evaluate their efficacy for hemostasis and/or collecting system sealing in this setting.
Wilhelm et al 2 performed LPNs on five pigs without hilar clamping and using pledgeted parenchymal compression sutures for hemostasis. The technique proved adequate for removal of small exophytic tumors, but additional hemostatic clips were necessary to control bleeding on the cut surface of the kidney. Ogan et al 3 performed LPN on 10 porcine renal units using a diode laser but found that adjunctive hemostatic clips were needed in 30% of the cases. McDougall et al 4 reported successful LPN in nine pigs using a plastic cable tie for transient parenchymal occlusion followed by use of an argon-beam coagulator to help effect hemostasis.
Ramakumar et al 5 used FocalSeal-L (a water-soluble polyethylene glycol polymer that, after applying to tissue, requires a light source to activate) to effect sealing after hilar clamping and LPN in the porcine setting. Although there was no evidence of urinary leak or hydrogel separation from the renal parenchyma, they commented that the added step of photoactivation made the polymer difficult to use.
Several studies have confirmed that fibrin glue can seal small collecting system injuries. Patel et al 6 showed that the combined use of fibrin glue and Gelfoam is an effective means to obtain hemostasis and seal collecting system injuries up to 10 mm at physiologic pressures and up to 50 cm water in the acute setting. However, no survival studies were reported by this group after their initial experiment. Marcovich et al 7 created large (7.5-cm) cystotomies in a porcine model and repaired them with either fibrin glue or a cyanoacrylate adhesive. Four of the six pigs treated with fibrin glue had significant urinary leaks, and three of these pigs died. Although this study was performed using a cystotomy model, it suggests that large defects may not be adequately repaired with fibrin glue alone.
Bernie et al 8 evaluated hydrogel tissue sealants (CoSeal® and Tisseel®; Baxter, Deerfield, IL) in porcine LPN with 3-day short-term acute and 6-week chronic survival arms. Their conclusion was that CoSeal was not as effective as fibrin glue in adhering to the cut renal surface and sealing the collecting system during LPN. Further, both acute and chronic kidneys repaired with CoSeal had significantly more bowel adhesions at the surgical site.
Desai et al 9 concluded in their study that although GMHS material (FloSeal) was safe and effective in obtaining hemostasis after hand-assisted partial nephrectomy without hilar clamping in the porcine model, the technique should be used with caution in renal tumors extending deep into the collecting system, as its efficacy in the closure of large collecting system defects remains unclear. L'Esperance et al 10 in their 1-week survival study after open partial nephrectomy showed that Tisseel alone was not adequate for either hemostasis or management of major collecting system injury.
Johnston and associates 11 performed a comparative study of seven agents in an open surgery hypertensive porcine model. Shallow and deep resections were performed to approximate various clinical situations. The authors found that Tisseel and FloSeal worked well for small resections, but larger resections required a sutured bolster for hemostasis.
In our study, the blood loss during the partial nephrectomy ranged from 50 to 200 mL (mean, 95 mL). The increase in hemoglobin on day 1 was possibly due to hemoconcentration, because the animals were kept nil by mouth and not much IV fluid was given during the procedure. Importantly, the hemoglobin did not decrease, confirming that there was no continued bleeding after the procedure.
The significant increase of serum urea on day 1 and of creatinine on days 1 and 3 is probably due to the loss of renal tissue and to some degree of postischemic impairment of renal function. By day 5 the urea level had returned to baseline, although the creatinine on day 5 remained slightly elevated (8% increase) above baseline level. At day 28 the serum creatinine (but not urea) was significantly higher than at baseline (38% increase), most probably due to the increase in body (muscle) mass of the animals. The fact that on day 28 the mass of the heminephrectomy tissue plus the right kidney mass was not significantly different from the left kidney mass proves that the right kidneys continued to grow normally.
The postoperative absence of any complications and the radiological and histological findings on day 28 show that TachoSil was effective in achieving hemostasis as well as sealing of the caliceal system after upper-pole LPN in this animal model.
We acknowledge that our study has many limitations. Only right-sided upper-pole nephrectomies were performed, because of their relative ease and need for standardization on protocol. The porcine kidney may not be an ideal model, because the blood supply is somewhat different from the adult human kidney, and therefore, direct extrapolation of results to the human patient is not advisable.
Sealants are effective and safe topical agents to control bleeding during nephron-sparing surgery. They should not be viewed as an alternative, but as complementary agents to be used to improve surgical outcomes. Further prospective studies are necessary to validate their role in relation to other hemostatic support techniques. 12
Conclusion
TachoSil appears to help seal collecting system injuries as well as to provide an adjunct to hemostasis in the porcine model. However, we would recommend further large animal studies prior to proceeding to human application in this setting, especially because the porcine kidney is not an ideal model to quantify its efficacy.
Footnotes
Acknowledgments
The authors thank Ms. Mary Austin (Laboratory Animal Technologist, Head of the Animal Research Facility at the Faculty of Health Sciences, Tygerberg), Mr. Johan van Rensburg (Supervisory Clinical Technologists in Critical Care, Department of Anaesthesiology, Tygerberg Hospital), Ms. Isobel Henning (Marcus Medical, Cape Town, Republic of South Africa), Mr. Alwin Deale (Covidien), and Ms. Sabina du Plessis (Medhold, Cape Town, Republic of South Africa). The purchase and housing of the experimental animals, theater fees, drugs, disposables, and laboratory tests were funded by the manufacturer of TachoSil (Nycomed UK, Oxford, Buckinghamshire, UK).
Disclosure Statement
No competing financial interests exist.