
Abstract
Introduction:
The immediate (1–5 hours) response to percutaneous renal access (PERC) in pigs is vasoconstriction in the treated kidney. The present study determined the longer-term (72 hours) consequences of this surgical procedure.
Materials and Methods:
Adult female pigs were anesthetized, and bilateral glomerular filtration rate (GFR), effective renal plasma flow (ERPF), urine flow rate, and sodium excretion rate were measured before and 1 hour after sham PERC or unilateral, single-tract PERC using a balloon dilator system. Animals were allowed to regain consciousness and were then anesthetized 72 hours later for final measurements of bilateral renal hemodynamic and excretory function together with renal para-aminohippuric acid (PAH) extraction (a measure of tubular organic anion transport efficiency).
Results:
Bilateral renal hemodynamics were unchanged in the sham-PERC-treated pigs over the 72-hour observation period. In contrast, both GFR and ERPF were reduced by approximately 55% in the PERC-treated kidney within 1 hour of access, and returned to pre-PERC levels within 72 hours. Renal hemodynamics were not significantly altered in the opposite, untreated kidney of the PERC-treated pigs. Renal PAH extraction was decreased in PERC-treated kidneys at 72 hours post-PERC. Both sham-PERC-treated and PERC-treated animals showed similar falls in urine flow rate and sodium excretion rate immediately after treatment and at 72 hours after PERC.
Conclusions:
Renal vasoconstriction characterized the acute response of the treated kidney to unilateral PERC, whereas impaired tubular function (reduced PAH extraction) with near-normal GFR and ERPF characterizes the later (72 hours) response to PERC.
Introduction
Clinical studies have reported that renal function is not compromised several weeks, months, or years after PCNL for most patients, 3 –10 but the immediate effect of PCNL on renal function is less well defined—either no change, 11 –13 or a fall in renal function. 3,12 We have used an in vivo pig model to explore the acute effects of percutaneous renal access (PERC) and have recently reported that unilateral, single-tract PERC results in an immediate, marked, and sustained (5 hours) reduction in renal hemodynamic and excretory function in both the treated and opposite, untreated kidneys. 14 The longer-term consequences of unilateral PERC on bilateral renal function are unknown and are the focus of the present study. We chose to examine bilateral renal function after 72 hours of recovery from unilateral, single-tract PERC surgery, in part because this time interval coincides with the time that urologists may regain percutaneous access to remove any residual stones.
Materials and Methods
Details of the surgical procedures for renal function measurements and PERC have been previously described. 14,15 Thirteen adult female farm pigs weighing ∼70 kg (Hardin Farms, Danville, IN) were used in this study. One kidney of each animal was subjected to either sham PERC (n = 6) or single-tract PERC (n = 8).
General surgery
Swine were anesthetized with an intramuscular injection of ketamine (15–20 mg/kg)/xylazine (2 mg/kg) followed by intubation and the inhalation of isoflurane (1–3%). Catheters were introduced into an ear vein (infusion of saline at 1% body wt. + inulin/para-aminohippuric acid [PAH] at 70 mL/hour), femoral artery (system blood pressure recording + arterial blood sampling), and both ureters (urine collection). Catheters were also placed in both renal veins (renal venous blood sampling) for the calculation of renal PAH extraction on the last day of the experimental protocol (see below).
PERC surgery
A catheter was placed in each ureter cystoscopically. The urinary collecting system of one kidney was filled with saline-diluted contrast agent (Renografin-60), and a single-tract PERC was achieved in the lower pole of the left kidney using a 30F NephroMax balloon dilator system and Amplatz working sheath guided under fluoroscopy. The urinary collecting system was observed and irrigated with saline to evacuate blood clots using a 24F nephroscope. The working sheath was then replaced with an 8F Cope loop nephrostomy tube, which was removed 24 hours later. The PERC surgery, from initial puncture to placement of the Cope loop, was performed in 48 ± 5 minute (range, 30–75 minute).
Sham PERC consisted of a skin incision over the left kidney made lateral to the paraspinous muscles. Contrast agent was injected into the renal collection system via the externalized ureteral catheter. The incision site was closed with silk suture at about the time normally taken to complete PERC.
Renal function measurements
Glomerular filtration rate (GFR) and effective renal plasma flow (ERPF) were estimated using the renal clearances of inulin and para-aminohippuric acid (PAH), respectively. The renal extraction of PAH (EPAH = [PAHarterial − PAHrenal venous]/PAHarterial) was measured and used in the calculation of true renal plasma flow (true renal plasma flow [TRPF] = ERPF/renal PAH extraction [EPAH]). EPAH also provides an estimate of the efficiency of tubular organic anion transport. Urinary sodium excretion rate was calculated as the product of urine flow rate and urinary sodium concentration.
Experimental protocol
Renal function measurements were taken before (∼1 hour after completing general surgery) and 1 hour after PERC surgery. The catheters were then removed, and the animals were given an intravenous injection of Torbutrol (analgesic) and Cefazolin (antibiotic), and allowed to regain consciousness. The animals were maintained on oral antibiotics (Septra suspension in food), and then again anesthetized 72 hours later for general surgery and renal function measurements—including blood sampling from both renal veins, which was achieved by catheters being inserted into both femoral veins and advanced into the renal veins under fluoroscopy.
Statistics
Body weight and baseline cardiovascular functional measurements between the sham-PERC-treated group and the PERC-treated group were compared using two-sample t-tests. Baseline glomerular filtration and renal perfusion values for each kidney were also compared using the two-sample t-tests. Paired t-tests were used to compare renal functional changes at 1 hour and 72 hours after treatment to baseline measures within a group for each kidney separately. Paired t-tests were used to compare renal functional measures at 72 hours between treated and untreated kidneys within each group. In all tests, p < 0.05 was considered to indicate statistical significance, and data are presented as mean ±standard error of the mean.
Results
Pigs of the sham-PERC-treated group had slightly lower body weight than those of the PERC-treated group (59 ± 1 kg vs. 66 ± 1 kg, respectively; p < 0.01).
Renal function
Baseline cardiovascular function was similar in both groups of pigs and overall remained unchanged throughout the 72-hour experimental protocol—blood oxygenation slightly improved at 1 hour after sham PERC (Table 1). Baseline values for glomerular filtration and renal perfusion were similar in each kidney both within and across the sham-PERC-treated and PERC-treated groups. Bilateral renal hemodynamic function at 1 or 72 hours after sham PERC was not significantly different from values measured before sham treatment (Fig. 1). In contrast, unilateral single-tract PERC resulted in an immediate and marked reduction in GFR and ERPF in the treated kidney with no significant change in function in the untreated kidney (Fig. 2). Both GFR and ERPF in the PERC-treated kidney had returned to near-normal levels after 72 hours (Fig. 2), whereas EPAH was impaired (Table 2). As a result, the calculated value for TRPF in the PERC-treated kidney exceeded that in the contralateral, untreated kidney at 72 hours postsurgery in all five pigs (Table 2). This difference, however, did not reach statistical significance (171 ± 78 mL/minute, p = 0.092).
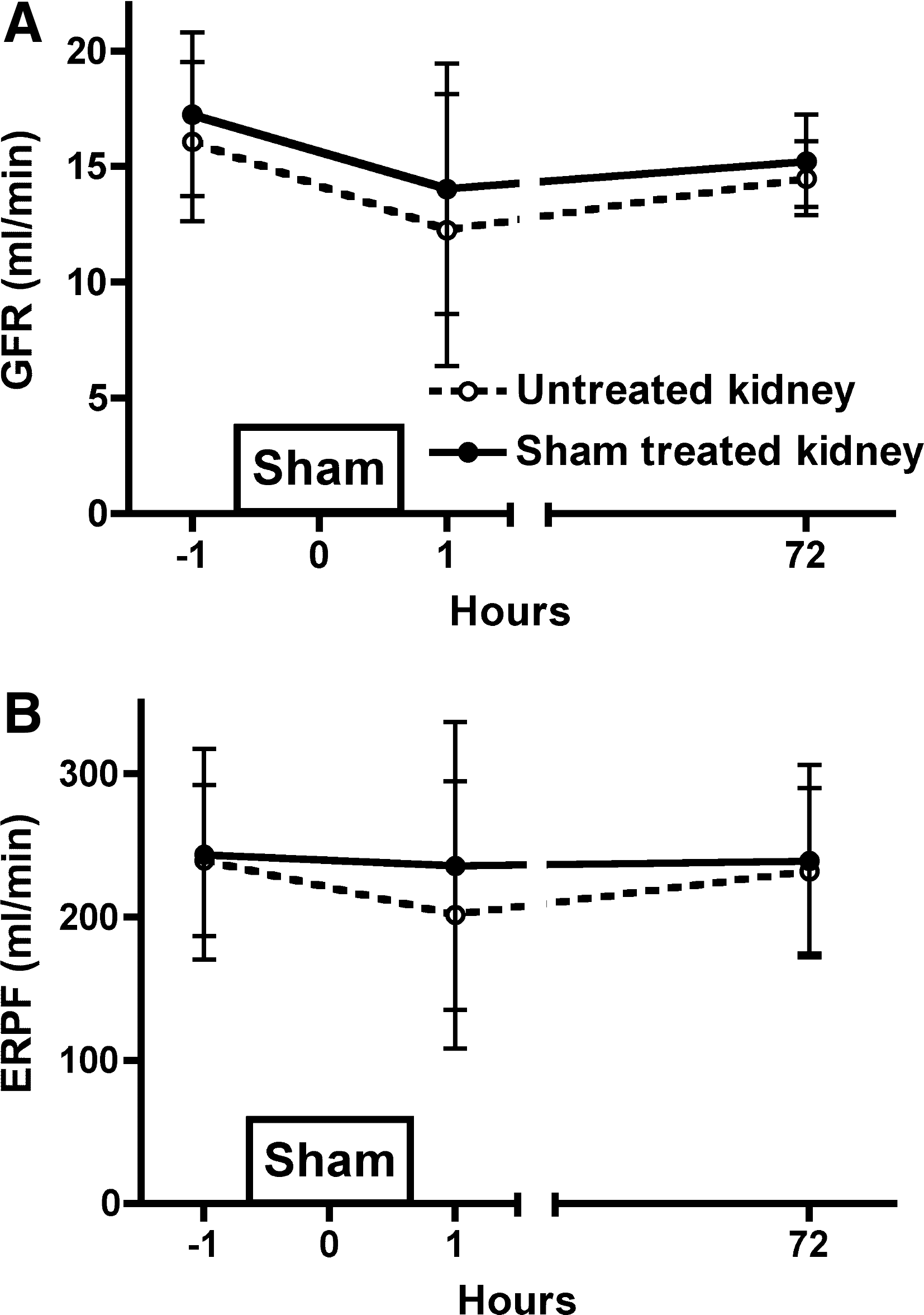
The effect of sham percutaneous renal access (PERC) on bilateral glomerular filtration rate (GFR) (
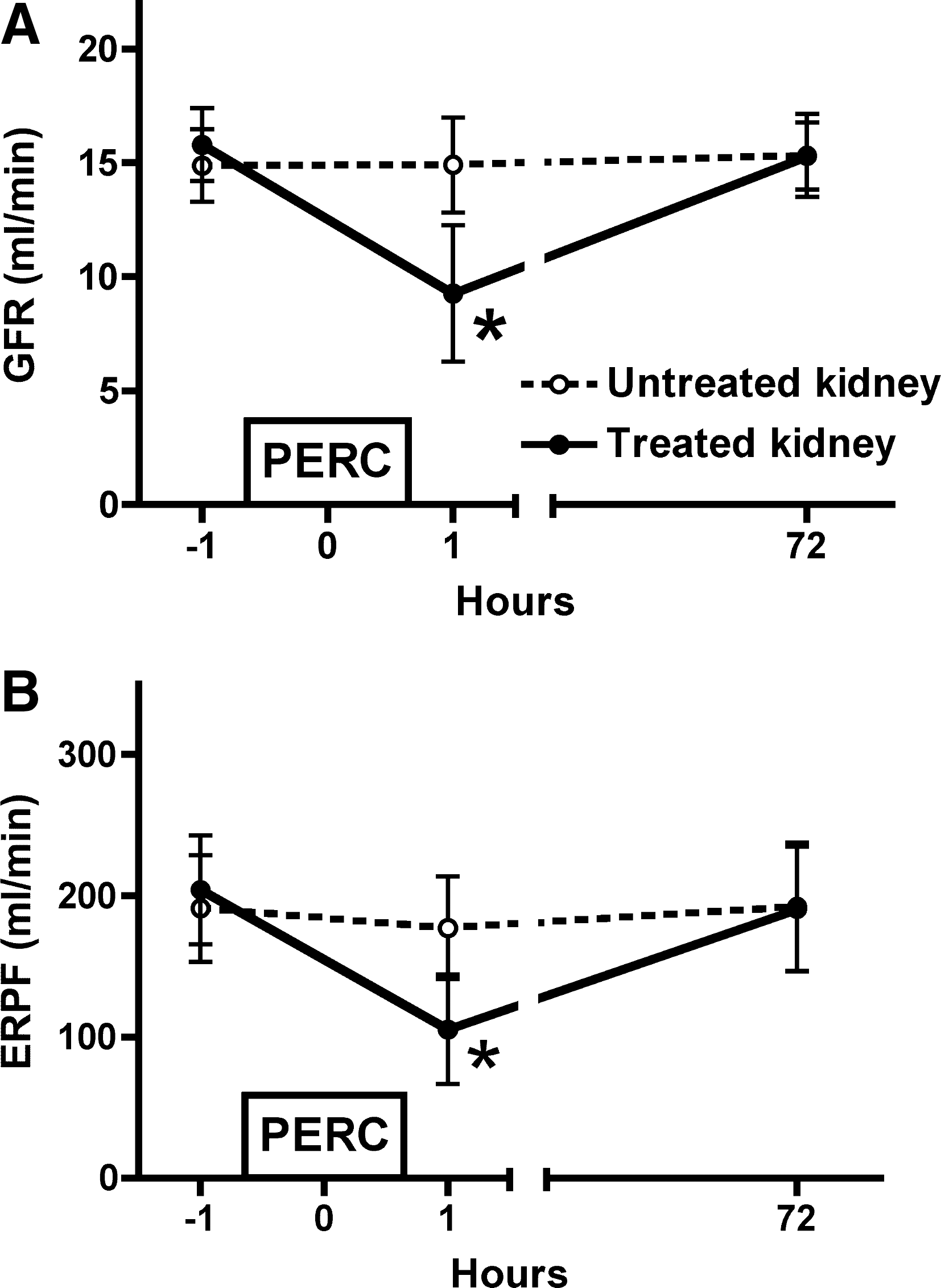
The effect of unilateral PERC on glomerular filtration rate (
p < 0.05 versus the respective baseline value.
PERC = percutaneous renal access; MAP = mean arterial blood pressure; HR = heart rate; SPO2 = arterial blood oxygen saturation; Hct = hematocrit.
p < 0.01 untreated versus PERC-treated kidneys in the PERC-treated group.
EPAH = renal PAH extraction; TRPF = true renal plasma flow.
Rates of urine flow and sodium excretion from both kidneys in the sham-PERC-treated and PERC-treated groups were highly variable and showed similar responses over the course of the experimental protocol—that is, an overall trend to be reduced at 1 hour and 72 hours compared with baseline (pretreatment) values (Figs. 3 and 4).
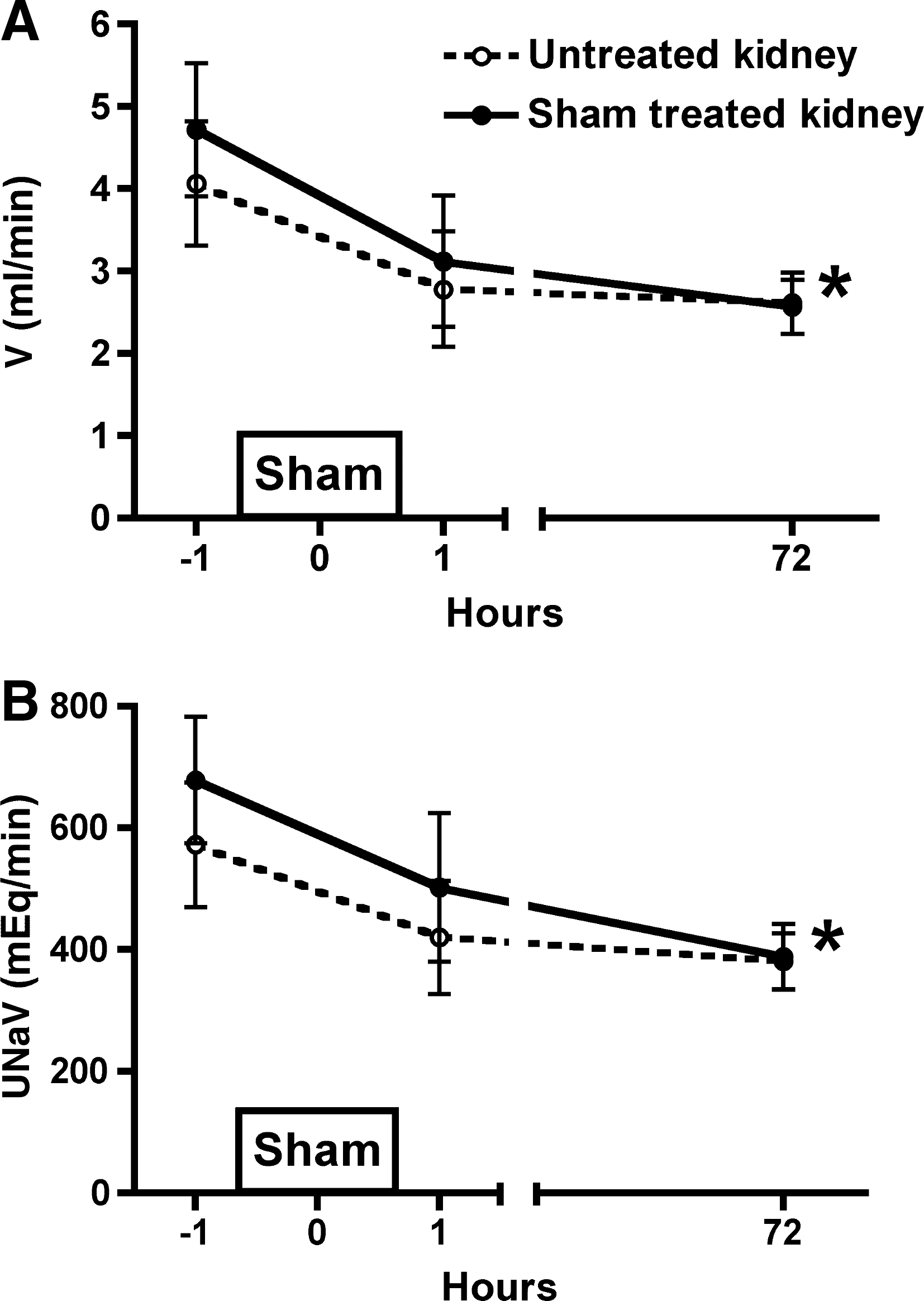
The effect of sham PERC on bilateral urine flow rate (V) (
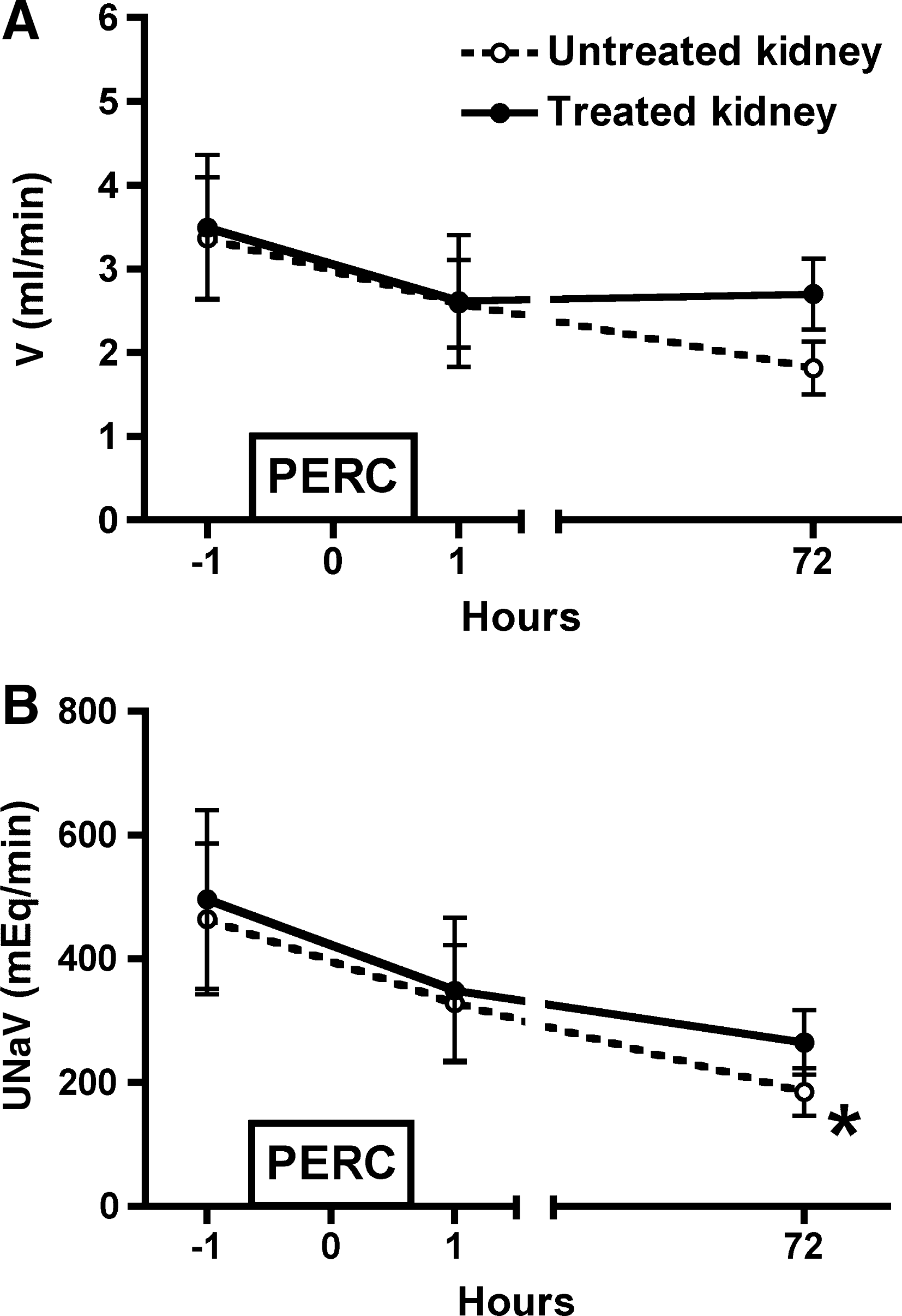
The effect of unilateral PERC on bilateral urine flow rate (
Renal morphology
Visual inspection of the surface of the PERC-treated kidney suggested that the access site could still be patent at 72 hours. This was confirmed ex vivo by inserting a guide wire (0.035" [0.889 mm] diameter) into the surface opening and easily advancing the wire into the urinary collecting system under fluoroscopy (Fig. 5). In addition, measurements made on a serially sectioned PERC-treated kidney indicated that the open tract at the kidney surface had a diameter of ∼1 mm (not shown).
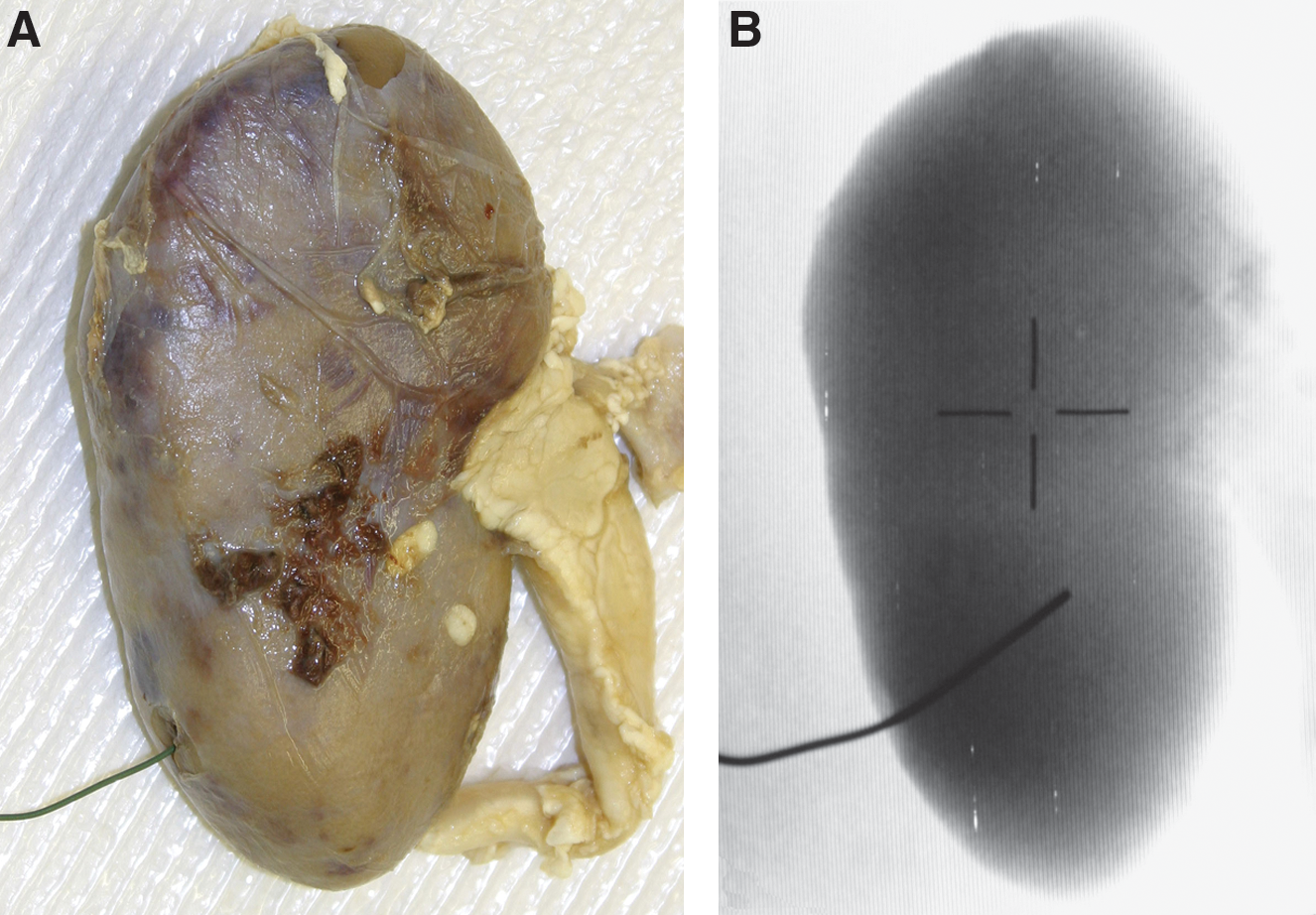
Guide wire (0.035″ [0.889 mm] diameter) inserted into the access tract of a PERC-treated kidney 2 days after removal of the nephrostomy tube (
Discussion
The results confirm our previous observation in pigs that unilateral PERC results in an immediate and marked decrease in hemodynamic function in the surgically treated kidney. 14 We have now expanded these acute findings by demonstrating that glomerular filtration and blood perfusion in the PERC-treated kidney had largely recovered to normal 72 hours after PERC.
GFR and ERPF were estimated using clearance methodologies, which give an integrated picture of whole-kidney hemodynamics and provide no information regarding changes in regional renal perfusion and filtration. Therefore, we cannot exclude the possibility that hemodynamic function remains compromised in some fashion in the percutaneous accessed pole of the kidney at 72 hours, especially since tissue injury is localized to the treated pole of the kidney. 14 Imaging modalities such as PET or MRI would be useful in providing information of spatial and temporal changes in renal filtration and perfusion after PERC. Notwithstanding the limitations of clearance methods for estimating renal function, our results do show that overall renal hemodynamics had recovered from the trauma of single-tract PERC in relatively short time.
Urinary excretion rates were highly variable in both groups of pigs with a trend for both urine flow and sodium excretion rates to be lower in both the treated and contralateral untreated kidneys immediately after sham PERC or PERC surgery. This finding agrees with our prior report of similar acute effects of sham PERC and PERC on urinary excretory function in anesthetized pigs. 14 The present study demonstrated that water and sodium excretion rates remained somewhat reduced 72 hours after sham PERC or PERC surgery. These reductions could reflect the length of anesthesia and surgery and, perhaps, that the short recovery period after the first surgery was insufficient for the pigs to adequately recuperate. Regardless of the factors involved, we found no significant differences in excretory function between PERC and sham PERC pigs.
We have previously shown that the renal extraction of PAH was decreased immediately after PERC and restricted to the treated kidney. 14 This finding implied an acute impairment of renal tubular PAH secretion, which the present study revealed was still depressed after 72 hours. PAH is transported from the blood into the renal tubules via selective organic anion transporters (OATs) located on basolateral and apical proximal tubule membranes. 16 The effect of PERC on the renal elimination of other compounds, such as drugs, that are also transported by OATs remains to be determined, as is the case for other tubular transport systems (e.g., organic cationic transporters and ATP-binding cassette [ABC] transporters) that may be impaired by PERC. However, the impairment in EPAH (an estimate of OAT efficiency) was localized to the PERC-treated kidney and presumably reflects some aspect of the injury and trauma to the renal tubules after surgery. The clinical implication of this finding is that the PERC-treated kidney has a reduced ability to handle drugs that depend on OATs for elimination for at least 72 hours after the surgical procedure, which perhaps should be considered in postoperative medical therapy. Clearly, further studies are needed to determine how long this tubular impairment lasts and its impact on the renal excretion of drugs.
ERPF was determined by measuring the renal clearance of PAH and provides an approximation of TRPF with the assumption that all of the PAH is removed from the blood in one passage through the kidney. However, a small percentage of the blood delivered to the kidney will perfuse some medullary structures, the renal capsule, and parts of the renal hilus without circulating through vessels that perfuse the renal tubules. PAH in this blood is therefore not available for tubular secretion and returns to the systemic circulation. Therefore, the renal clearance of PAH must be appropriately corrected by the fractional removal of PAH from the arterial blood (i.e., EPAH), to obtain TRPF. Such calculations indicated that TRPF of the PERC-treated kidney tended to be ∼60% greater than that of the opposite, untreated kidney or sham-PERC-treated kidneys at 72 hours postsurgery. Although this increase in TRPF did not reach a level of statistical significance, there is the suggestion that the kidney could be in a state of hyper-perfusion a few days after PERC. Direct measurements of regional renal perfusion rates will more clearly establish whether this is indeed the case, and also if such an elevated perfusion is focal to the site of injury or more global in nature.
We have previously observed acute bilateral reductions in renal hemodynamic function in both pigs and a human patient after unilateral, single-tract PERC. 14,17 Although the present study demonstrated a significant acute impairment in renal function only in the instrumented kidney, inspection of individual responses to unilateral PERC revealed that ERPF of the untreated kidney was reduced on average 37% (range, 17–62%) in six animals immediately after PERC surgery, and increased (7% and 64%) in two animals. Therefore, the majority of pigs showed bilateral renal vasoconstriction immediately after unilateral PERC surgery—in agreement with our previous report 14 —which recovered to near-normal values by 72 hours postoperative.
We also demonstrated ex vivo that the access tract remained patent 48 hours after removing the nephrostomy tube, and extended from the renal surface all the way to the urinary collecting space. Inspection of serial sections from a PERC-treated kidney also revealed that the collapsed but open channel was about 1 mm in diameter at the renal surface. We did not attempt to perform a second PERC—as would be the case if a patient had residual stones. However, we presume that such second-look procedures would again reduce renal hemodynamic function to some degree.
In summary, whereas renal vasoconstriction characterizes the acute (hours) response to PERC, tubular dysfunction (as reflected by the lower renal extraction of PAH) and near-normal renal perfusion appears to characterize the later (72-hour) response to PERC.
Footnotes
Acknowledgments
This study was supported in part by a grant from Boston Scientific Co. The authors are grateful to William Fat-Anthony, Kelli R. Wind, Cynthia D. Johnson, and Philip M. Blomgren for their expertise and assistance in the completion of this project.
Disclosure Statement
James E. Lingeman is a consultant, advisor, meeting participant and lecturer for Boston Scientific Co.