
Abstract
Purpose:
Recently, it has been demonstrated that ureteral obstruction is associated with increased cyclooxygenase (COX)-2 expression and that selective COX-2 inhibitors provide potent analgesia with fewer side effects in patients with ureteral stones. Moreover, selective COX-2 inhibitors have been shown to decrease in vitro contractility of the human ureter. We aimed at evaluating the effects of the selective COX-2 inhibitor NS-398 on human ureteral smooth muscle contractility and compare its potency with that of nonselective COX inhibitors, COX-1 inhibitors, and other COX-2 inhibitors.
Materials and Methods:
Ureteral samples were obtained from human adult subjects undergoing radical nephrectomy. After isolating the upper ureteral strips, we analyzed the contractile responses of the ureteral strips to high potassium (KCl 35 mM) and Bay K 8644 and the relaxation responses of a nonspecific COX inhibitor (indomethacin), a COX-1 inhibitor (SC-560), and a COX-2 inhibitor (NS-398 and celecoxib) to KCl and Bay K 8644-induced contraction by measuring isometric tension.
Results:
NS-398 produced dose-dependent (10−9–10−5 M) relaxation of KCl (35 mM)-precontracted strips of the ureter, whereas indomethacin (10−8–10−5 M) and SC-560 (10−9–10−5 M) did not. Both tonic and phasic contraction of Bay K 8644 (methyl-1,4-dihydro-2,6-dimethyl-3-nitro-4-2(trifluoromethylphenyl)pyridine-5-carboxylate) (1 μM) were significantly inhibited by NS-398 (10−5 M). Another selective COX-2 inhibitor, celecoxib, did not show potent inhibitory effects as strong as those of NS-398.
Conclusions:
We concluded that NS-398 reduces tonic or phasic contraction by inhibiting the action of voltage-dependent calcium channels. NS-398 has dual inhibitory effects with COX-2 inhibition on ureteral spasms due to renal or ureteral colic.
Introduction
Prostanoids (prostaglandins [PGs], thromboxanes, and prostacyclins) mediate contractility, pressure, and pain during ureteral obstruction. 3,4 Cyclooxygenase (COX) synthesizes prostanoids from arachidonate and exists in two isoforms: COX-1 (a constitutive form) and COX-2 (an inducible form). 5 COX-1 and -2 enzymes have been identified in the ureter and the urothelium. 6
Nonsteroidal antiinflammatory drugs (NSAIDs) have been used to block COX to reduce inflammation as well as to act as analgesic agents. Nonselective COX inhibitors, such as indomethacin, ketorolac, and ibuprofen, have been successfully used to treat pain associated with ureteral obstruction. 7,8 However, side effects have been demonstrated in the gastrointestinal tract and kidney, where disruption of the production of PGs reduces cytoprotective mucus formation, which, in turn, leads to gastric ulceration, renal insufficiency, and platelet dysfunction. 9 –12 Selective COX-2 inhibitors have been shown to provide potent analgesia with fewer toxic side effects. 13,14 Recently, it has been demonstrated that ureteral obstruction is associated with increased COX-2 expression 15 and selective COX-2 inhibitors decrease in vitro contractility of the human ureter. 16 Especially, among selective COX-2 inhibitors, NS-398 has been shown to inhibit spontaneous mammalian ureteral contractions in a fashion similar to that of indomethacin. 16
The purpose of this study was to evaluate the effects of NS-398 on human ureteral smooth muscle contractility and to compare its potency with nonselective COX inhibitors, COX-1 inhibitors, and other COX-2 inhibitors.
Materials and Methods
Tissue preparation
With institutional review board approval, 56 upper ureteral strips were obtained from seven human adult subjects undergoing radical nephrectomy due to renal cell carcinoma.
Isolation and preparation of the human ureters
Fresh upper ureteral tissues were immediately placed in 100% oxygen-saturated HEPES-buffered physiological salt solution (NaCl 140 mM, KCl 5 mM, CaCl2 2 mM, MgCl2 1 mM, glucose 11 mM, HEPES 5 mM; pH 7.4) and transported to the laboratory as soon as possible. Four longitudinal strips and four transverse strips of the upper portion of the ureter were cut and trimmed to 0.1 × 0.2 × 0.6 cm. The strips were attached to a wire-connected force transducer (52-9545; Edinburgh, Harvard, United Kingdom) to record isometric tension, and the force was recorded and saved in a personal computer through a force signal transducer and amplifier (PowerLab 4SP; AD Instruments, Lexington, Australia). The solution in the bath was bubbled with mixed gas (95% O2 and 5% CO2), maintained at 37°C, and exchanged at 30-min intervals. Resting tension was adjusted to 0.2 g for 60 minutes during the equilibration period.
Force measurement of the human ureteral strips
Contractile responses of the ureteral strips
Concentration-dependent contractile responses were observed using contractile agents including KCl (35 mM), phenylephrine (10−9–10−4 M), and Bay K 8644 (voltage-dependent calcium channel agonist, 10−6–10−5 M).
Relaxation responses of the ureteral strips
Relaxation responses induced by indomethacin (nonspecific COX inhibitor; 10−8–10−4 M), SC-560 (COX-1 inhibitor; 10−9–10−5 M), and NS-398 (10−9–10−5 M) were then recorded in the ureteral strips in which tone was elicited with KCl (35 mM) after 5 minutes. To examine the involvement of calcium influx through voltage-dependent calcium channels, the ureteral strips were precontracted using the calcium channel opener Bay K 8644 (10−6–10−5 M); and subsequent responses to indomethacin, SC-560, and NS-398 were then observed. Additionally, to clarify the effects of NS-398 related to COX-2 inhibition, we investigated the effects of celecoxib (another selective COX-2 inhibitor) on the contractile response using both KCl and Bay K 8644.
All cumulative applications of each one of the contractiles and/or relaxing agents were performed for at least eight strips, and the reproducibility of the results was confirmed.
Drugs
Celecoxib was purchased from Cayman Chemicals (Ann Arbor, MI), and all other chemicals were purchased from Sigma (St. Louis, MO).
Statistical analysis
All data are expressed as means ± standard error of the means, where n represents the number of strips or cells. Student's t-test and repeated measures analysis of variance were used for the analysis, and p-values of 0.05 or lower were considered statistically significant. The values of relaxation responses were given as a percent ratio of the level of tension at maximal relaxation to the level of maximal contraction by the contractile agent.
Results
Contractile responses of the ureteral strips
In the high-K+ solution (KCl 35 mM), the ureteral strips induced a biphasic contractile response consisting of an initial slow increase in tone associated with phasic contractions that disappeared as the slow contraction reached a plateau. Tonic contraction was more prominent than phasic contraction (n = 8; Fig. 1). In response to phenylephrine (10−9–10−4 M) and Bay K 8644 (1 μM) treatment, the ureteral strips generated significant tonic and phasic contractions. No difference in contraction between the longitudinal and transverse strips was observed.
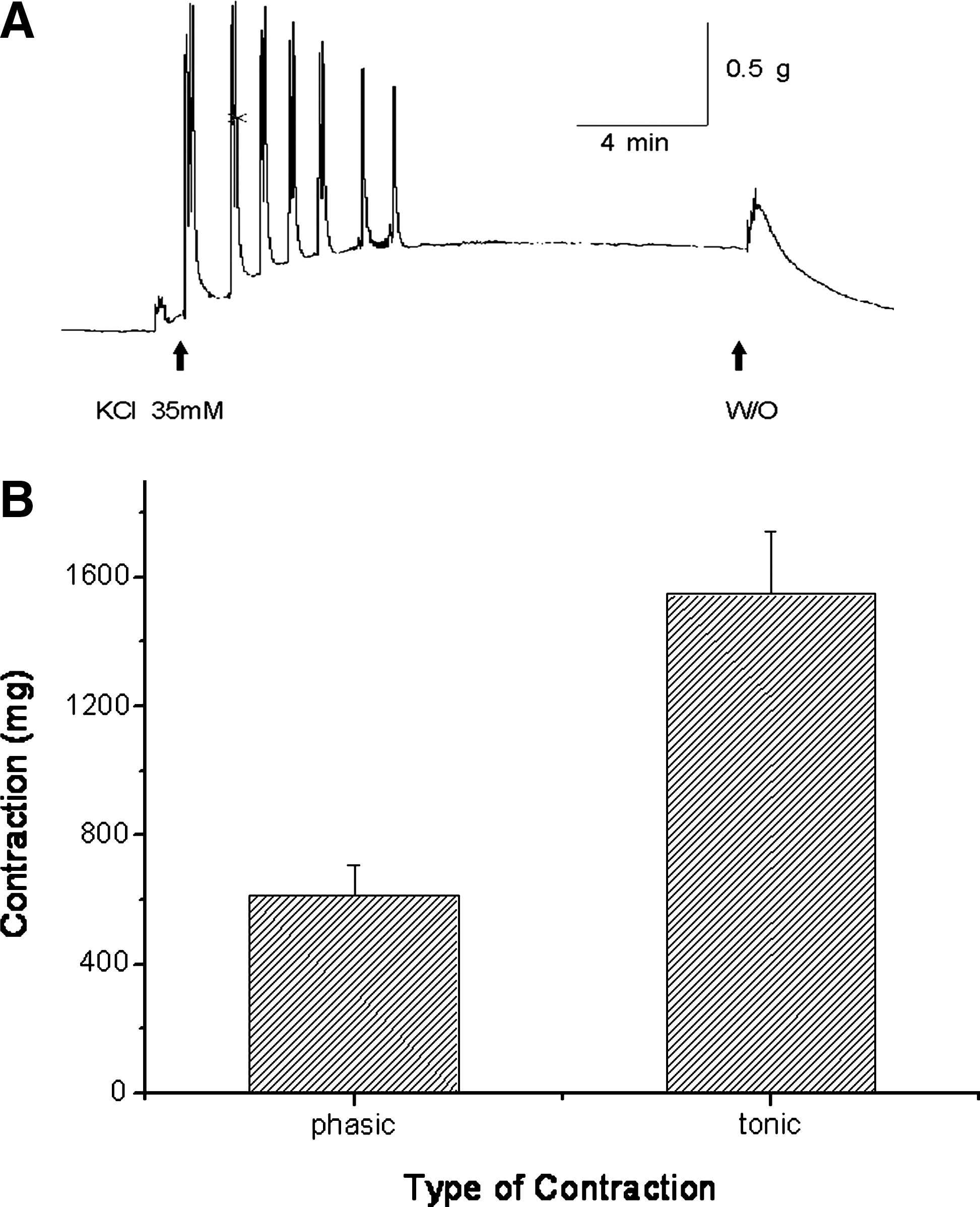
Typical tracing of the effects of KCl (35 mM) treatment on the contractions of a longitudinal ureteral strip. (
Relaxation responses of the ureteral strips
Although the ureteral strips were not significantly relaxed by indomethacin or SC-560 under the KCl-precontracted state, they were with NS-398 (n = 8, p < 0.05; Figs. 2 and 3). Moreover, NS-398 significantly decreased Bay K 8644-induced tonic and phasic contractions, whereas indomethacin and SC-560 did not (n = 12, p < 0.05; Fig. 4). At the highest concentration of NS-398 (10−5 M), the response to the Bay K 8644 was almost abolished (Fig. 5). Another selective COX-2 inhibitor, celecoxib, did not show as potent inhibitory effects on ureter contraction as did NS-398 (data not shown).

Comparison of the effects of various cyclooxygenase (COX) inhibitors when tone was elicited with KCl (35 mM). After 5 minutes of KCl pretreatment, the COX inhibitors were applied in a dose-dependent manner (10−9M–10−5 M, 3 minutes at each concentration, respectively). (
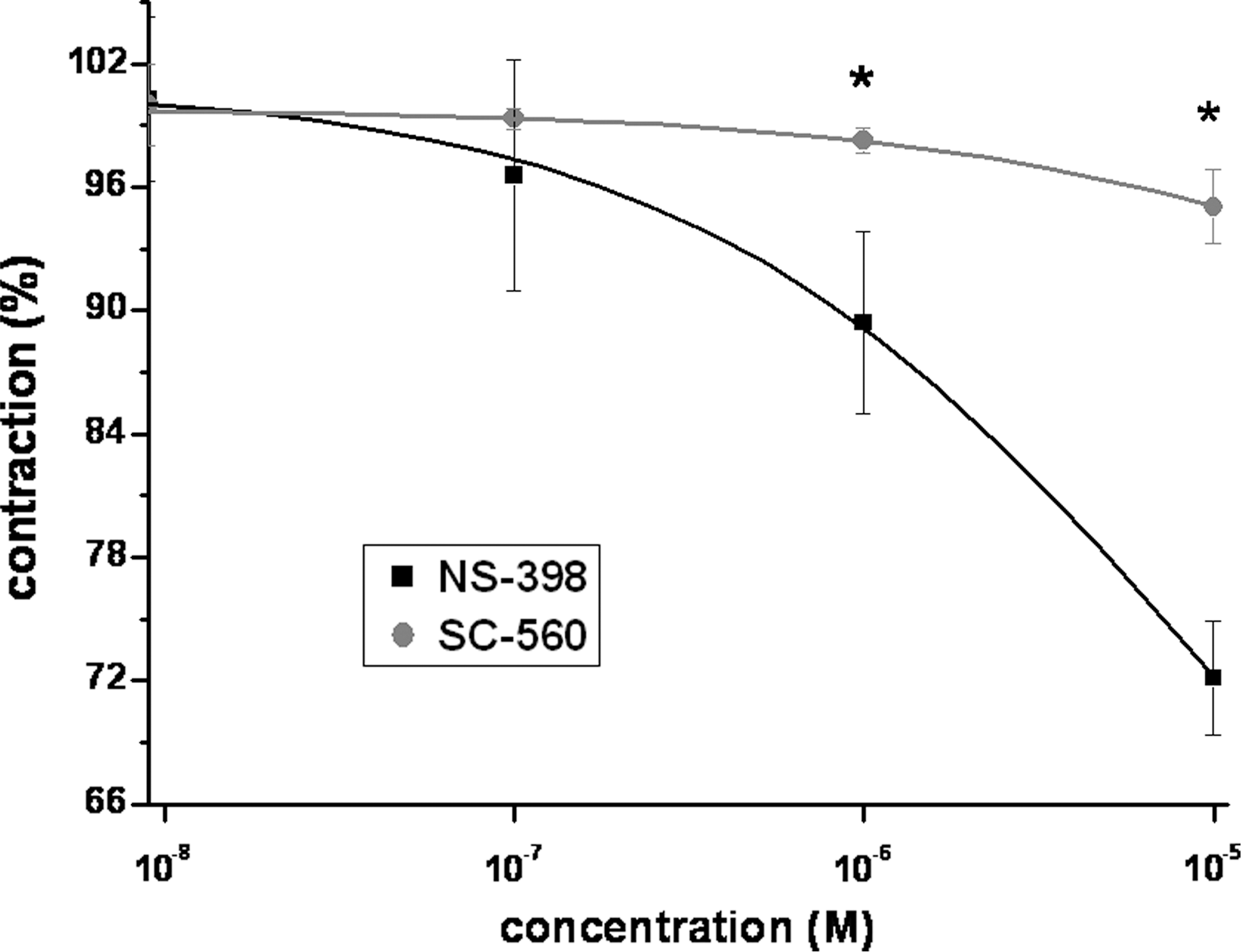
Comparison of the relaxation potencies of NS-398 and SC-560 to KCl-induced contractions. The ureteral strips were significantly relaxed by NS-398 in concentrations of >10−6 M under a KCl precontracted state but were not relaxed by SC-560 (n = 8, *p < 0.05).

Comparison of the relaxation effects of NS-398, indomethacin, and SC-560 to Bay K 8644-induced contraction. The ureteral strips were significantly relaxed by NS-398 in concentrations of >10−8 M but were not relaxed by indomethacin or SC-560 (n = 12, *p < 0.05).
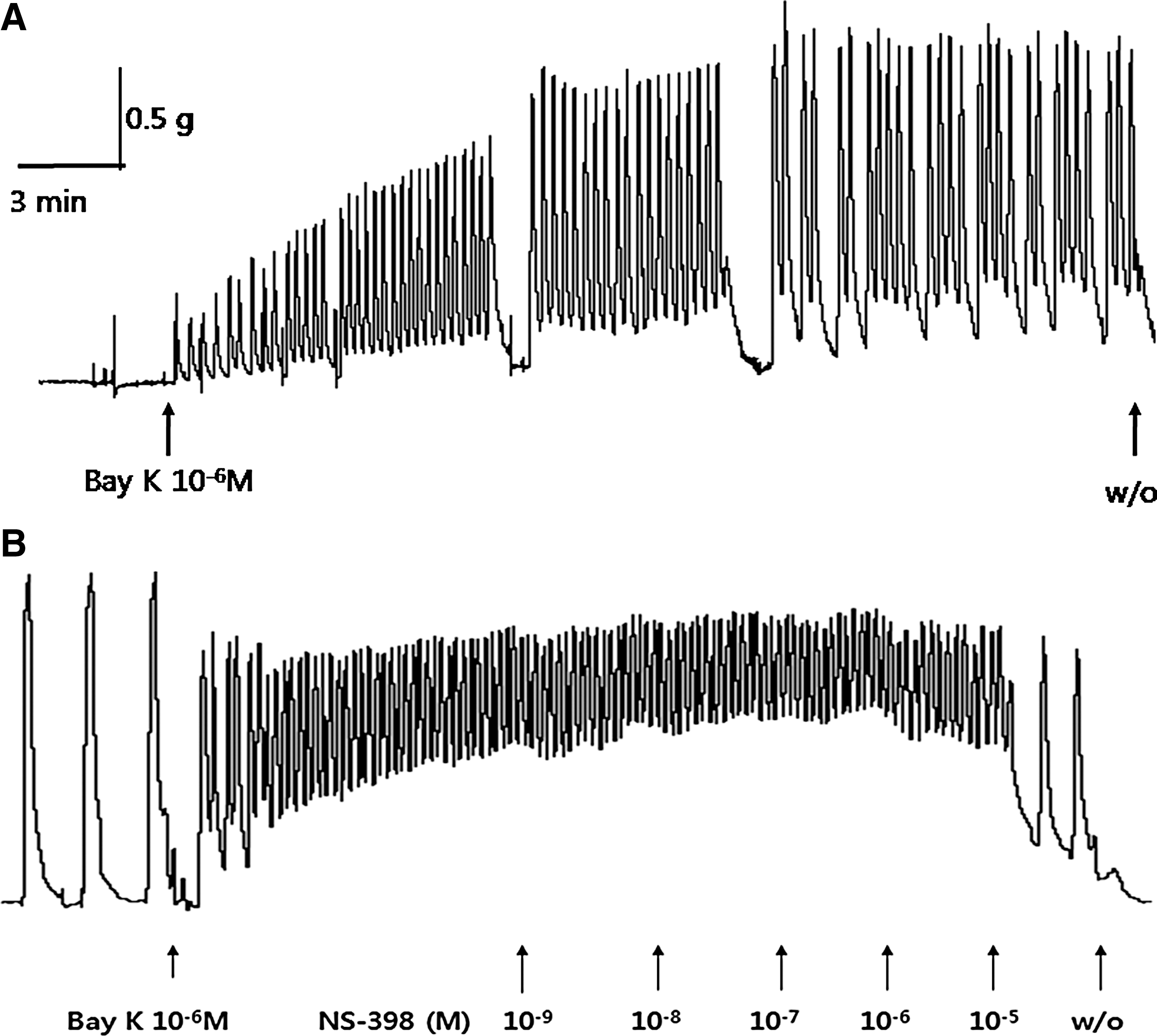
The effects of NS-398 on tonic and phasic contractions by Bay K 8644. Dose-dependent application (10−9–10−5M) of NS-398 (
Discussion
PGs play a role in many different biological processes, including hemostasis, modulation of kidney and gastric functions, and inflammation and maintenance of smooth muscle contractility. NSAIDs have been used to block COX to reduce inflammation as well as to act as analgesic agents. NSAIDs also are commonly used for the management of renal colic. Ureteral contractility originates in the renal pelvis from electrical activity at pacemaker sites and distally propagates, creating peristalsis and urine propulsion. During obstruction, increased intraluminal pressure and volume induce a transient increase in peristaltic wave amplitude and frequency and increased renal back pressure. Hypercontractility and stretching significantly amplify pain. 17
COX-1 is normally expressed in many tissues and organs and plays an important role in maintaining physiologic functions. COX-2 can be induced by various stimuli, including nerve stimulation, stretching of the muscle, mucosal injuries, and inflammatory mediators involving the ureter. 18 Recently, a number of inhibitors relatively selective for COX-1 or COX-2 have been discovered, each of them demonstrating differing degrees of potency in their ability to inhibit COX activity. Of these, NS-398 has been demonstrated to selectively inhibit COX-2 activity, causing an irreversible structural transformation of the enzyme. 19,20 NS-398 has also been demonstrated to be less toxic compared with standard NSAIDs, inducing little gastric damage in rats. 20,21
Our results confirm that NS-398 inhibited ureteral contractility in vitro more effectively than did the nonspecific COX inhibitor indomethacin or the COX-1 inhibitor SC-560. This fact suggests that NS-398 has a unique inhibitory mechanism independent of PG synthesis inhibition. Since NS-398 also inhibited Bay K 8644-induced contraction, NS-398 might affect ureteral contractility via inhibition of voltage-dependent calcium channels.
It has been reported that several NSAID mechanisms other than prostanoid synthesis inhibition may account for the decrease of agonist-induced contractions, including inhibition of calcium channels or extracellular calcium influx. 22,23 Perez et al 23 suggested that some of the NSAIDs assayed induce smooth muscle relaxation related to the inhibition of extracellular calcium influx on KCl-induced contraction of isolated rat uteri and that Bay K 8644 does not revert the inhibitory effect of NSAIDs. In our study, NS-398 showed a potent inhibitory effect on voltage-dependent calcium channels that indomethacin and SC-560 did not. Moreover, when we carried out the experiment using another selective COX-2 inhibitor that has been clinically approved, celecoxib, we did not find potent inhibitory action of ureteral smooth muscle contraction elicited by KCl or Bay K 8644. Meanwhile, in contrast to our results, Zhang et al 24 reported that celecoxib does inhibit L-type calcium channels in pheochromocytoma cells via a COX-2 independent pathway, but NS-398 failed to inhibit voltage-gated calcium channel currents. Therefore, we postulated that the action of NS-398 on voltage-dependent calcium channels depends on tissue selectivity, and further studies are needed to investigate in which tissues these inhibitory effects to the calcium channels can be found.
Antagonism of L-type calcium channels is well known to reduce ureteral contractions and may be used to treat ureteral stones. 25 Sahin et al 26 demonstrated that both endogenous PG synthesis and calcium influx from the extracellular space are responsible for the spontaneous rhythmic activity of the ureter. Calcium channel blockers have been used to reduce ureteral tone in patients with ureteral stones. 27 Since NS-398 has dual potent inhibitory effects on human ureteral contractility via both blocking voltage-dependent calcium channels and COX-2 inhibition, it may be an attractive candidate in the treatment of renal colic with stone and various other ureteral obstructive disorders.
The limitations for the clinical application of NS-398 are cardiovascular problems and the fact that NS-398 was an experimental compound, until now. The cardiovascular complications are associated with the use for prolonged periods of time. 28 −30 Although their use in renal colic lasts only a few days, further in vivo studies are needed to investigate potential clinical use and safety, with regard to both the cardiovascular system and other possible toxicities.
Conclusion
NS-398 showed proper action in reducing tonic or phasic contractions by inhibition of voltage-dependent calcium channels in addition to COX-2 inhibition. NS-398 may be useful in the management of spasms caused by renal or ureteral colic than do current treatments.
Footnotes
Acknowledgments
This work was supported by a grant of the Korea Healthcare Technology R&D Project, Ministry of Health, Welfare & Family Affairs, Republic of Korea (A085138).
Disclosure Statement
No competing financial interests exist.