
Abstract
Aim:
Precise targeting is essential for adequate treatment of lesions during image-guided therapy. The aim of this study was to compare the performance of two emerging image-guided targeting technologies in a phantom model.
Materials and Methods:
A computer-assisted navigation system and AcuBot were tested using three operators: an interventional radiologist and two endourologists. Fiducials were placed in an anatomic gelatin phantom and targeted by both systems. The images were reconstructed and analyzed using a specialized software package (Amira; Visage Imaging, Carlsbad, CA). Accuracy was assessed by measuring proximity of the tip of the needle to the fiducial on computed-tomography-guided imaging. Accuracy and time to target were quantified and compared.
Results:
The mean distance from the desired target for AcuBot was 1.2 mm (range: 0.39–2.82). The mean distance from the desired target for the navigation system was 5.8 mm (range: 1.8–11.9). The AcuBot was significantly more accurate than the navigation system (p < 0.0001). The mean time from target acquisition to needle placement was 37 seconds (range: 15–75) for the AcuBot and 108 seconds (range: 45–315) for the navigation system (p = 0.001).
Conclusion:
Emerging technologies hold promise for increased accuracy during percutaneous targeted procedures. Both the AcuBot and the computer-assisted navigation system were accurate and efficient in a phantom targeting model. AcuBot was significantly more accurate, faster, and less user dependent than the navigation system. Further studies in animal and clinical studies are warranted to further advance this promising technology.
Introduction
Two emerging technologies that have the potential for increasing the accuracy and efficiency of percutaneous renal targeting are computer-assisted navigation systems and purpose-built robots. The computer-assisted navigation system allows the surgeon to know the alignment of the puncture needle in real time corresponding to a three-dimensional model acquired from preoperative computed tomography (CT) images. After the preoperative imaging is obtained and reconstructed, markers are placed both on the patient's body and the surgical tool to spatially localize the needle in relation to the desired target. This allows the surgeon to execute the needle trajectory based on real-time imaging feedback that displays needle orientation relative to that of the target. 3 AcuBot is a robotic system built in our URobotics laboratory at the Johns Hopkins Medical Institutions, and it can be mounted on a CT scanner. 4,5 Images acquired are processed by the AcuBot system, which then automatically orients and drives the needle tip to the desired target location.
The objective of the current study was to assess these two different systems in an anatomical phantom model and compare their performance with regard to accuracy and efficiency compared with that of the standard CT-guided manual approach.
Materials and Methods
Phantom model
A previously described synthetic torso (Lapman) based on the Visible Human Project of the National Library of Medicine that has the exact shape of a human torso was filled with agar gel. 6 Metallic fiducials (each approximately 2 mm in diameter) were placed in the gel at varying angles and acted as targets. Half of the targets in any given experimental arm were placed underneath ribs and required an oblique angled approach (>20°). A minimum of 12 attempts per arm were performed.
Computer-assisted navigation system
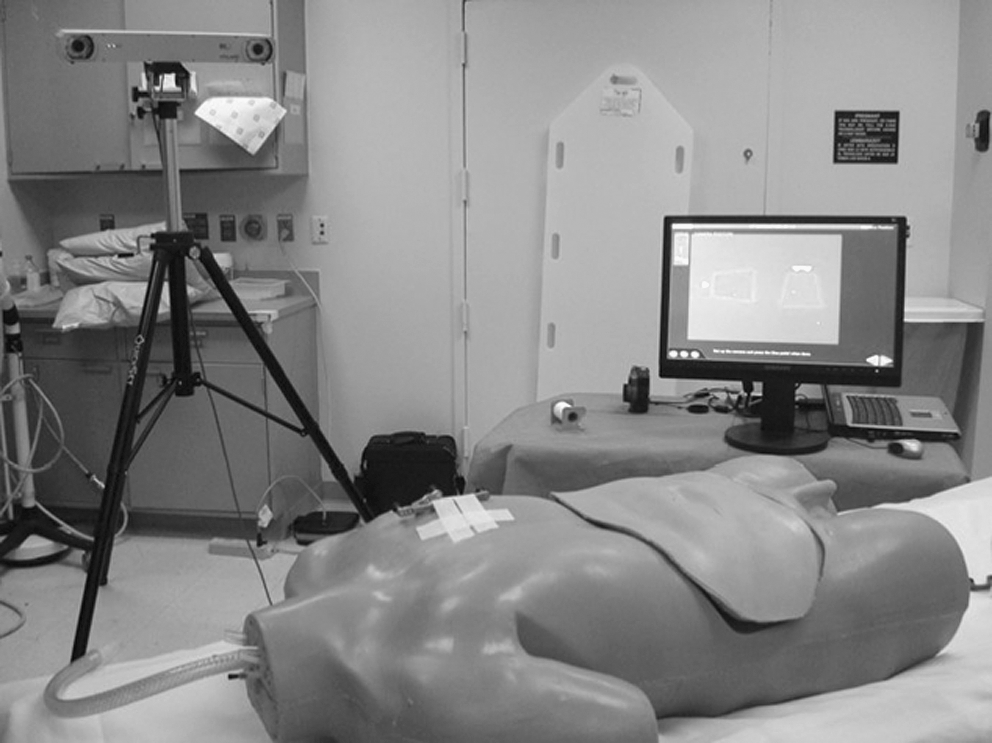
The computer navigation system (Koelis, Grenoble, France) intakes acquired CT images of the phantom model. To spatially localize the targeting needle, a Polaris® infrared camera system (Northern Digital, Inc., Ontario, Canada) is used. A reference marker is placed on Lapman to act as a reference point to which every other marker will be localized via the camera. A marker is also placed on the needle and both are presented to the Polaris camera. After registration, the operator can then guide the needle to the target by looking at a monitor that updates the position in real time (Fig. 1). When the needle tip and target intersect on the monitor, the task is complete. An “attempt” was defined as one cycle consisting of selecting a target and placing the needle in the target. Additional attempts were made by the operator (if they were not satisfied by initial placement) or if the CT scan showed the needle to be >1.5 cm from the target. That distance was chosen arbitrarily as the minimal acceptable distance for adequate targeting.
The AcuBot targeting system mounted on computed tomography scanner.
This navigational system was tested using three operators: one interventional radiologist (J.M.) and two endourologists who routinely perform image-guided procedures (B.M. and M.E.A.). The time to complete an attempt (time from selecting a target to placing the needle) and the number of attempts required per target were recorded. After each attempt, CT images were acquired, reconstructed, and analyzed using a specialized software package (Amira; Visage Imaging, Carlsbad, CA). The distance between the needle tip and center of the target bead was measured and recorded.
AcuBot robotic system
The AcuBot system has been previously described in detail. 5 Briefly, the robot is mounted on the CT scan gantry approximately 0.5 m away from the phantom (Fig. 2). A CT scan is performed and the images are transferred to AcuBot. The images are registered as previously described. Via a touch-screen monitor, the operator can then manipulate reconstructed images, select a target, and instruct AcuBot to orient and drive the needle to that selection. Time and measurements were recorded as described above for the computer-assisted navigation system.

Computer-assisted navigation device with the infrared tracking device in the background.
Manual attempt
The same operators (J.M., B.M., and M.A.) used a free-hand technique to place the needle into the phantom. A scout CT scan was performed and the operators targeted the fiducials using either a “scan and view” mode or CT fluoroscopy according to their preference. After each attempt, a CT scan was performed and the images were saved for analysis. Time to complete a successful attempt, the number of attempts, and the distance between the needle tip and center of the target were recorded and analyzed. The computer-assisted navigation system attempts were performed a few days before the manual attempts. The number of attempts was defined as previously described for the navigation system.
Statistical analysis
Statistical analysis was performed using STATA version 10.0 (STATA Corporation, College Station, TX). Target accuracy and time to needle placement were compared in the three arms using the Student's t-test. All p-values were two-sided, with a p < 0.05 considered statistically significant.
Results
All modalities allowed for eventual accurate targeting of the fiducials. The mean time between target selection and needle placement was fastest for the AcuBot system and slowest for standard manual placement (37 seconds vs. 234 seconds) (Table 1). AcuBot was significantly faster than either the navigation system or manual placement for target acquisition and needle placement (AcuBot vs. Navigation, p < 0.0001). Although slower than AcuBot, the computer-assisted navigation system was significantly faster than that of manual needle placement alone (p < 0.01).
Manual targeting required, on average, 1.9 attempts (range: 1–4 attempts) to achieve adequate accuracy (within 1.5 cm of the fiducial), whereas only 1 attempt was necessary using AcuBot or the navigational system. Overall accuracy and precision were statistically superior for AcuBot compared with the navigational system and manual attempts (p < 0.0001, Table 1). Mean distance between needle tip and target for the robotic system was 1.2 mm (range: 0.39–2.82 mm) with no attempt resulting in a targeting error greater than 2.8 mm. In contrast, the mean distance to target for the navigational system and manual attempts was 5.8 mm (range 1.8–11.8 mm) and 8.4 mm (range 2.2–25.0 mm), respectively. Although there was a trend toward improved accuracy with the navigational system compared with manual targeting, this failed to reach statistical significance (p = 0.21).
Targeting time and accuracy were independent of operator for the AcuBot attempts, whereas variability was observed with the other two modalities. For example, during navigational system attempts, the average distance between the needle and target for one operator was significantly better than the other two operators (4.0 mm vs. 6.8 mm vs. 7.2 mm, p = 0.03). Additionally, the angle of entry needed to reach the target had no impact on overall accuracy for the AcuBot attempts. However, targeting beads placed at oblique angles (>20°) resulted in significantly longer times and lower accuracy than nonoblique attempts for both the navigational system and manual approaches (p = 0.01).
Discussion
Image-guided percutaneous interventions are increasingly used in urology today. From a urologic standpoint, percutaneous renal interventions are becoming more popular for the treatment of both benign and malignant conditions. The popularity of percutaneous renal procedures is in large part due to the increased detection of small renal masses resulting from the wide spread use of cross-sectional imaging modalities leading to an increased use of ablative therapy for this disease entity. 7,8 Although renal tumor ablation can be performed via a variety of techniques, including open and laparoscopic approaches, the percutaneous approach incurs the least morbidity and, in the case of cryoablation, often does not require a general anesthetic. 9 Additionally, percutaneous renal mass ablation has been shown to be more cost effective than laparoscopic ablation. 10
Currently, a major limitation of percutaneous ablative therapies is imprecise targeting owing to freehand needle placement. Generally, ablative probes are placed using real-time ultrasound or under CT-guided fluoroscopy, which can result in significant difference in actual probe placement in relation to the intended target. Masses in difficult locations or those in proximity to other organs can prove to be an even greater challenge to accurately target. From an oncologic perspective, accurate needle placement is of paramount importance for adequate ablation, as an adequate ablation area ensures effective cancer treatment while maximally sparing normal renal parenchyma. 11 This notion is fostered by the higher failure rates both with radio frequency ablation and cryoablation for renal masses compared with that of surgery, which are likely in large part because of inadequate ablation at the time of the initial procedure. 8
In addition to the oncologic implications discussed above, imprecise targeting may lead to multiple, unnecessary probe passes that increase procedure length and patient pain, and may potentially lead to increased complication rates. Computer navigational assistance and robotic systems have the potential to shorten or eliminate the learning curve of percutaneous needle placement and improve accuracy and time of these procedures. The decreased procedural times afforded by these modalities may also offer the potential for significant cost savings. Additionally, the consistent accuracy of the navigational and robotic systems minimizes radiation exposure both to the patient and operator.
The current study demonstrates that the AcuBot system results in quicker and more accurate needle placement than either navigational system or manual approaches. In addition, the robotic system's results seem to be independent of operator or angle of approach, allowing for efficient and accurate needle placement even during challenging cases. Further studies in larger series and in human subjects are needed to confirm such advantages. The application of these computerized systems extends far beyond the field of renal mass treatment. From a urologic standpoint, such systems could aid urologists to obtain percutaneous renal access for the management of urolithiasis and collecting system tumors, which is largely performed by interventional radiologists today. Additionally, these same modalities can be applied to other disease entities such as percutaneous targeting in other systems such as the liver, lung, and brain.
The current study does have several limitations that merit discussion. Most notably, this is an initial study using phantom models and 2-mm fiducial targets. Patient movement (breathing and otherwise) may represent a challenge for these systems.
Further studies are warranted both in animal models and human subjects with actual target lesions to confirm the accuracy of both the navigation and AcuBot systems. Additionally, clinical studies in which lesions are ablated and then followed will be necessary to confirm the theoretical advantages of these modalities for treating renal masses. Our study does confirm the superior accuracy and efficiency of the AcuBot robotic system in a phantom model, thus warranting future studies to further define its potential clinical role.
Conclusion
Emerging technologies hold promise for increased accuracy during percutaneous targeted procedures. Both the AcuBot and the computer-assisted navigation system were accurate and efficient in a phantom targeting model. AcuBot was significantly more accurate, faster, and less user dependent than the navigation system. Further studies in animal and clinical studies are warranted to further advance this promising technology.
Footnotes
Disclosure Statement
No competing financial interests exist.