
Abstract
Purpose:
To describe our technical details of laparoendoscopic single-site (LESS) nephroureterectomy with bladder cuff excision for the management of upper urinary tract transitional-cell carcinoma (TCC) based on oncologic principles.
Patients and Methods:
Two patients underwent LESS nephroureterectomy for upper urinary tract TCC. In both cases, we used a homemade single-port device that consisted of a wound retractor and a surgical glove. Using the flexible laparoscopic instruments, nephrectomy was performed using procedures similar to those of conventional laparoscopic nephrectomy. Bladder cuff excision was performed laparoscopically using the same procedure with open technique.
Results:
All procedures were completed successfully without conversion to conventional laparoscopic or open surgery and without additional extraumbilical trocars or incisions. LESS nephreoureterectomy with bladder cuff excision was performed in 385 and 285 minutes with estimated blood loss of 100 and 350 mL, respectively. Both patients were discharged on postoperative day 3 without perioperative complications.
Conclusions:
LESS nephroureterectomy with bladder cuff excision for upper urinary tract TCC is a minimally invasive technique that may reproduce the open surgical technique and adhere to oncologic principles.
Introduction
The standard treatment for patients with upper urinary tract transitional-cell carcinoma (TCC) is nephroureterectomy with bladder cuff excision. Since it was first introduced by Clayman and associates 1 in 1991, laparoscopic nephroureterectomy results in decreased postoperative pain, shorter hospital stay, more rapid convalescence, and improved cosmesis compared with open surgery. These advantages are the fundamentals of scarless surgery, and the experience and use of laparoendoscopic single-site (LESS) surgery continues to expand among urologists. 2 –4 Preliminary results in LESS nephroureterectomy demonstrate that the techniques are feasible with advanced skills and optimal instrumentation. 3 –5 The proper technique for distal ureterectomy is still an area of controversy, however.
We describe a technique for LESS nephroureterectomy with bladder cuff excision for upper urinary tract TCC that may reproduce the open surgical technique and adhere to oncologic principles.
Patients and Methods
Two patients, a 68-year-old man (body mass index [BMI] of 20.69 kg/m2) and a 56-year-old woman (BMI of 21.4 kg/m2) with a diagnosis of TCC of the left renal pelvis underwent transperitoneal LESS nephroureterectomy. The surgical decisions were made after obtaining informed consent from the patients and Institutional Review Board approval from the ethical committee of the hospital.
Operative technique
The patients were anesthetized generally, and then placed in a flank position with the affected side elevated 70 degrees. A 4-cm umbilical skin incision was made and extended down to the peritoneum. We constructed a homemade single-port device according to the previously described technique. 6 First, a medium-sized Alexis wound retractor (Applied Medical, Rancho Santa Margarita, CA) was inserted through the incision, thus stretching the fascia enough to allow laparoscopic instruments to pass into the abdomen. A single-port device was made by attaching a size 6 1/2 surgical glove to the opening of the port, and then securing four trocars to the fingers of the glove using rubber bands. The glove was fixed to the outer ring of the wound retractor followed by insufflation of the peritoneum with 14 mm Hg CO2 (Fig. 1). Possible instability was prevented by folding the lower end of the glove with Alexis wound retractor together several times to reduce the distance between the trocar and the incision.
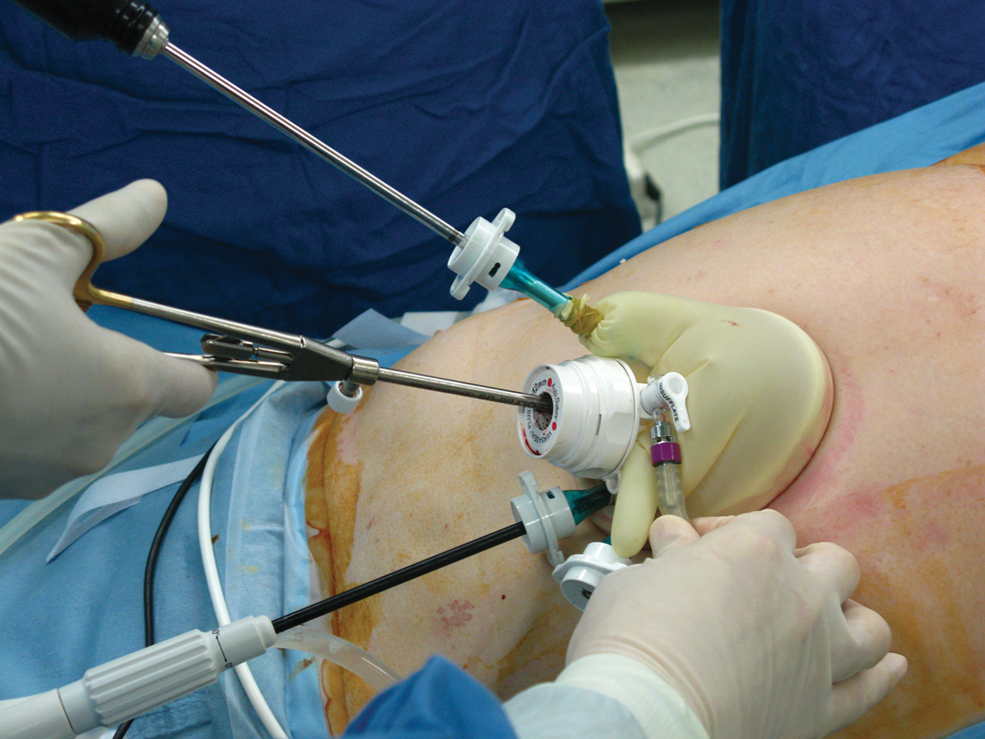
Homemade single-port device used in laparoendoscopic single-site nephroureterectomy.
Using flexible laparoscopic instruments (Covidien, Norwalk, CT, and CambridgeEndo, Framingham, MA), the LESS nephrectomy was performed in the same process as conventional laparoscopic nephrectomy. After the incision of the line of Toldt was made, we proceeded with the dissection medially until the hilum was exposed. The renal artery was first ligated with titanium clips, and then the renal vein was transected using Hem-o-lok clips or an endovascular stapler. After complete freeing of the kidney, the distal ureter was clipped without transection and dissected as low as possible until reaching the level of bifurcation of the common iliac artery.
After the nephrectomy was completed, we changed the position of the patients to a supine position with a 30-degree Trendelenburg decline and the affected side elevated slightly to perform the distal ureterectomy. After the ureter was retracted, the ureter was dissected caudally until the detrusor muscle fibers at the ureterovesical junction were reached, and then clipped 1 cm above the ureterovesical junction. Two stay stitches were placed in the bladder cuff just at the edges of the dissected detrusor muscle using a 3-0 polyglactin suture.
The intramural distal ureter was fully mobilized, the bladder was opened, and the ipsilateral ureteral orifice was taken out, including a 1-cm bladder cuff using flexible laparoscopic endoshears. The bladder opening was exposed by pulling the stay stitches and thereafter closed using a conventional rigid needle driver and dissector in one layer with 2-0 polyglactin interrupted sutures prepared with a Hem-o-lok clip and LapraTy clip at the terminal end (Fig. 2). After the suture was passed, additional Hem-o-lok and LapraTy clips were used to secure the suture.
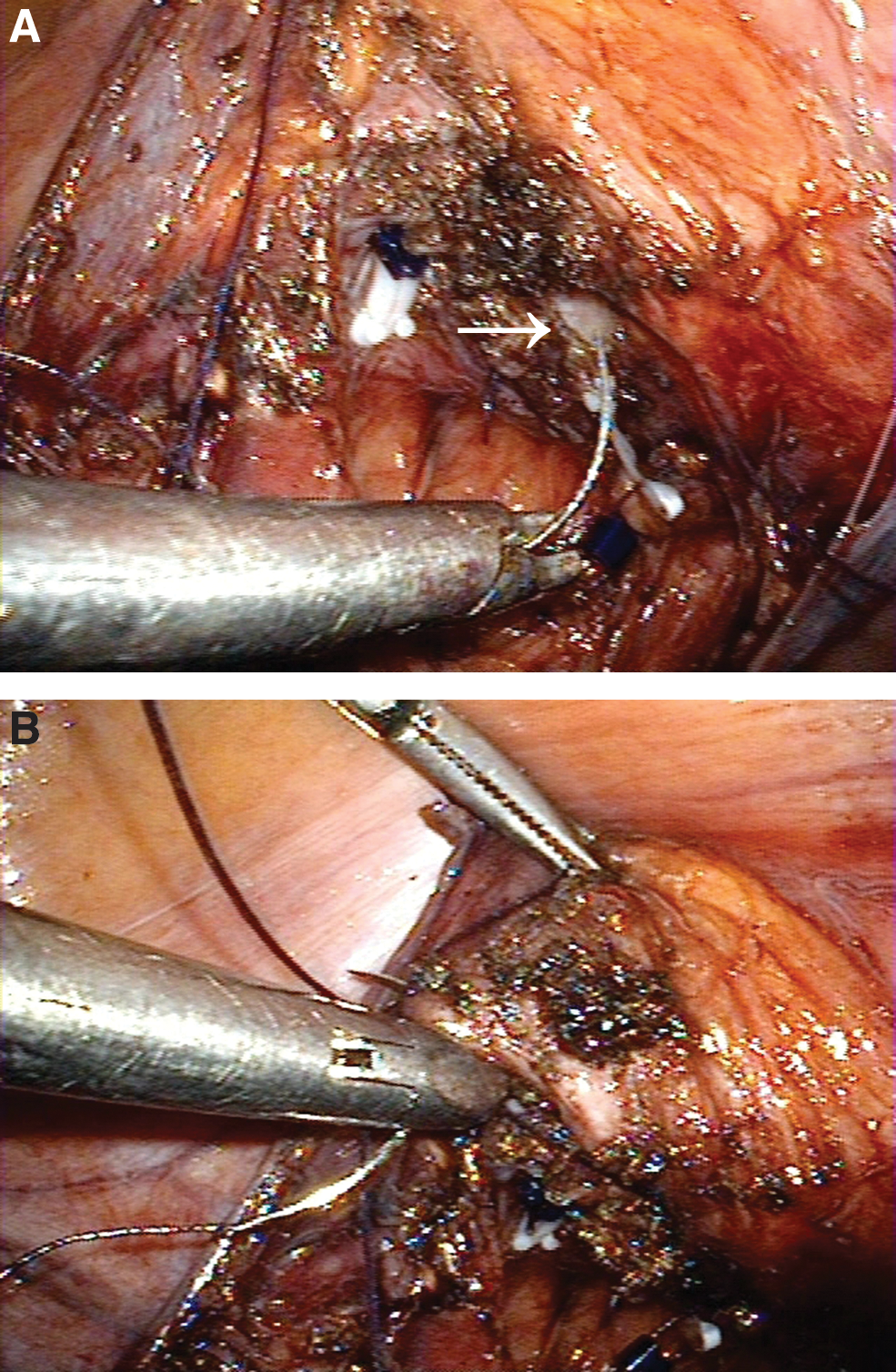
The opened bladder (
Urinary leakage was examined and then excluded after filling the bladder with 200 mL saline. The specimen was entrapped within the laparoscopic bag and retrieved through the umbilical incision without morcellation (Fig. 3). The incision was closed with a subcuticular absorbable suture (Fig. 4).
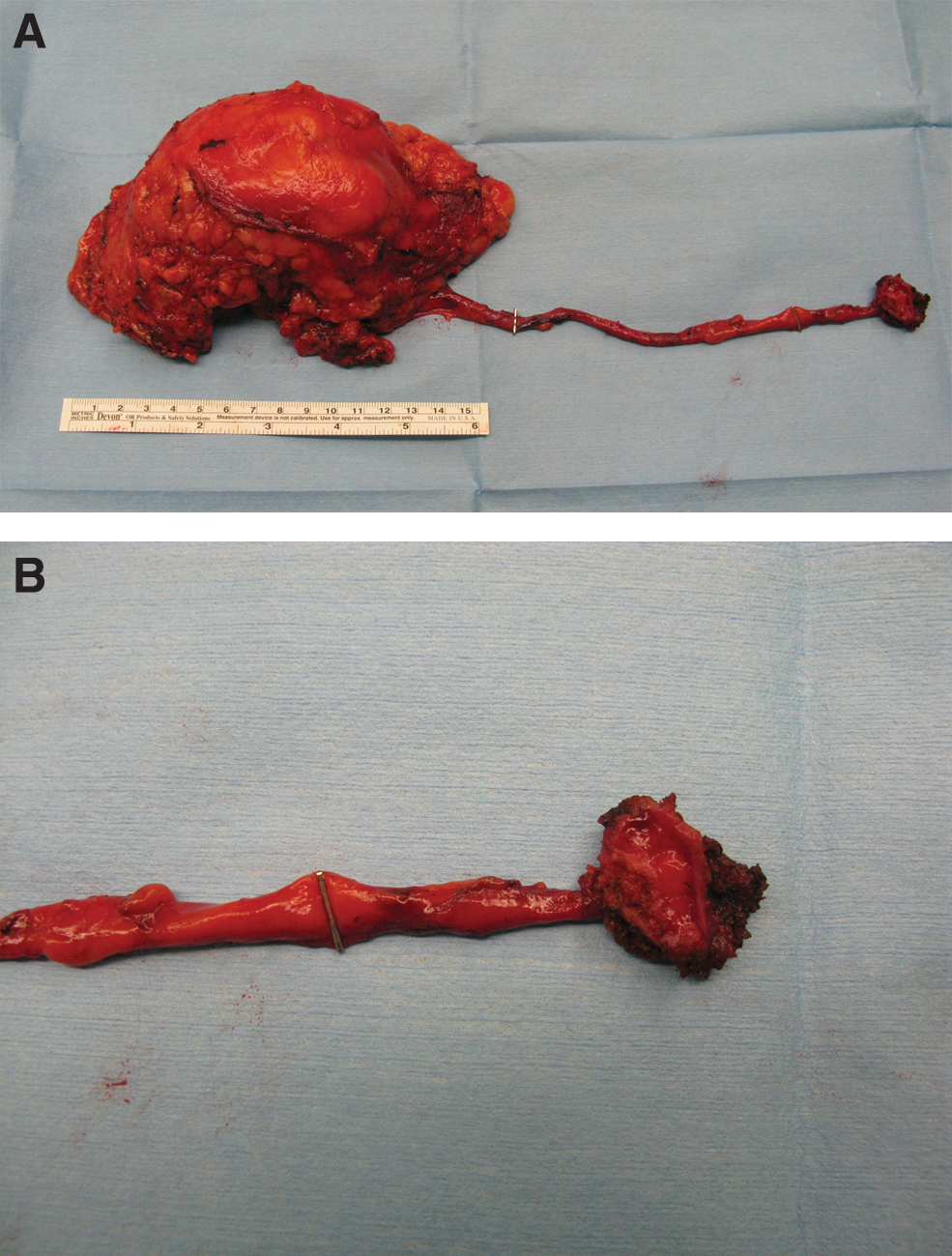
The removed specimen (

Postoperative view of the wound.
Results
Both LESS nephroureterectomies were completed successfully without additional extraumbilical trocars or conversion to conventional laparoscopic or open surgery. Table 1 shows the perioperative data of the patients.
Perioperative Data of the Patients
VAS = visual analog scale.
The 56-year-old woman had a 1.5-cm left renal pelvic enhancing mass. The total operative time was 385 minutes (time for nephrectomy, 145 min; time for bladder cuff excision, 240 min); estimated blood loss was 100 ml, and postoperative hospital stay was 3 days. Cystography performed 3 days after surgery showed no urine leakage; after cystography, the urethral Foley catheter was removed. Histopathologic examination revealed pT1 and grade 3 TCC with a negative surgical margin at the distal edge of the bladder cuff.
The 68-year-old man had a 4.0-cm left renal pelvic mass with multiple small para-aortic lymph nodes. LESS nephroureterectomy with bladder cuff excision and para-aortic lymph node dissection (Fig. 5) was performed in 285 minutes (time for nephrectomy, 175 min; time for bladder cuff excision, 110 min) with estimated blood loss of 350 mL. In this case, the time for nephrectomy was longer than the first case because of the para-aortic lymph node dissection. The urethral Foley catheter was removed on postoperative day 7 after cystography confirmed absence of urine leakage. Histopathologic examination revealed a negative margin pT3 and grade 3 TCC with no lymph node metastasis in eight lymph nodes retrieved.
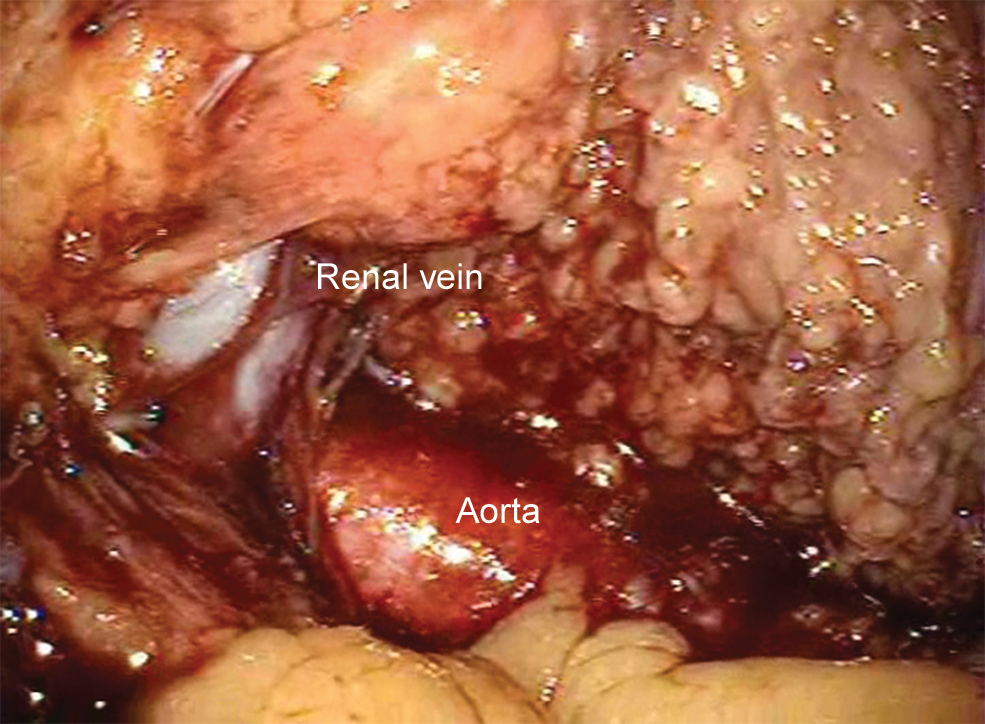
Intraoperative view after lymph node dissection.
Discussion
During the past several decades, minimally invasive surgery, including conventional laparoscopic surgery or LESS, has been used increasingly in the management of various urologic diseases. The goal of conventional laparoscopic surgery or LESS is to reproduce open surgical techniques in a minimally invasive manner. Because LESS is a novel technique, however, there are few literary reports about its application in malignancy.
There have been several reports that mention LESS nephroureterectomy for upper urinary tract TCC. 3 –5 They only reported, however, the lists and surgical outcomes of the various LESS procedures they performed 3,4 or their procedure for the distal ureter is either not well described or done in an open fashion, which maintains the advantages of our study. To our knowledge, this is the first published report concerning the technical details of LESS nephroureterectomy with bladder cuff excision for the management of upper urinary tract TCC. These preliminary data demonstrate that LESS nephroureterectomy with bladder cuff excision is feasible, safe, and based on the same oncologic principles as open surgical technique.
The principle of surgical treatment for upper urinary tract TCC is nephroureterectomy with en bloc excision of bladder cuff. Standard oncologic protocol necessitates resection of a 1-cm bladder cuff around the ipsilateral ureteral orifice to excise and completely remove the distal intravesical ureter. There are still concerns, however, regarding the optimal technique of bladder cuff excision. In an attempt to adhere to these oncologic principles, a variety of techniques have been used when performing distal ureterectomy and bladder cuff excision, including cystoscopic resection of the ureteral orifice (pluck technique), 7 cystoscopic detachment and ligation technique, 8 laparoscopic stapling of the bladder cuff, 9 and standard open technique.
Each technique has unique advantages and disadvantages. 10,11 From an oncologic point of view, however, the open technique remains one of the most reliable and sound procedures. The advantages of the open technique are its familiarity to surgeons and adherence to the oncologic principles of managing upper urinary tract TCC. The risk of tumor extravasation is minimized, direct visual confirmation of a resected ureteral orifice decreases the likelihood of incomplete removal of the distal ureter, and the bladder opening can be adequately closed. In this regard, we concluded that our technique for LESS nephroureterectomy with bladder cuff excision essentially parallels the advantages of standard open techniques.
Conclusion
We described our surgical details for LESS nephroureterectomy with bladder cuff excision for the management of upper urinary tract TCC through a single umbilical incision. We concluded that LESS nephroureterectomy is a minimally invasive technique that may reproduce the open surgical technique and adhere to the same oncologic principles of open surgical technique.
Footnotes
Disclosure Statement
No competing financial interests exist.