
Abstract
MRI is an imaging modality that is used in the evaluation and treatment of renal cancer. Although less frequently used than CT, MRI is useful in several aspects of renal cancer evaluation and may have some advantages. MRI has shown promising results for renal cancer staging (especially determination of vascular invasion by tumor), in differentiating malignant from benign complex cystic renal lesions, and in the treatment and follow-up of minimally invasive ablative therapies for renal cancer. In addition, new research shows promise for novel applications of MRI. Herein we review the evolving of MRI in renal cancer imaging.
Introduction
Of all solid renal lesions, the overwhelming majority are malignant (>80%). Smaller solid lesions have a greater chance of being benign (i.e., oncocytoma, angiomyolipoma, and other benign solid lesions), with benign lesions comprising up to 25% of solid renal lesions under 4 cm in some series. 5 Although historically RCC was diagnosed based on clinical symptoms (e.g., flank pain, palpable mass, and hematuria), with the increased used of cross-sectional imaging such as CT and MRI, the majority of these neoplasms (up to 80%) are now discovered incidentally. 6,7 Traditionally, CT has been the imaging modality of choice in the work-up of RCC, with its fast acquisition time, excellent anatomic detail, and the ability to perform complex three-dimensional reconstructions of renal tumor and vascular anatomy. 6 However, in recent years, MRI has gained popularity as a useful imaging modality for various aspects of the evaluation and treatment of RCC. MRI offers several advantages over CT, including no ionizing radiation, as well as less nephrotoxic contrast material. 6,8 Herein we review the most recent literature regarding the evolving role of MRI in the imaging of RCC.
MRI Appearance of RCC
As with CT, contrast enhancement of the renal lesion in question is the most important imaging feature in the MRI evaluation of RCC. 6,8 The MR signal is dependent on tissue and tumor characteristics, patient size, and the characteristics of the MR system used (i.e., gain setting, pulse sequence, and coils). 8 Most lesions will have a signal intensity less than that of the renal cortex on T1-weighted images. Quantitative assessment of gadolinium contrast enhancement is commonly used to determine the characteristics of the lesion in question and to differentiate solid from cystic lesions. A 15% increase in signal intensity on postcontrast enhanced images provides high sensitivity (100%) and specificity (94%) in distinguishing cystic from solid renal lesions. 6,8,9 In addition, subjective enhancement has been shown to be effective in the MR diagnosis of RCC, but smaller or hypovascular lesions may be difficult to differentiate using subjective techniques alone. 9 It is also important to note that among solid enhancing renal lesions, neither MRI nor CT can reliably differentiate RCC from common benign renal lesions such as oncytoma. 6 With few exceptions, however, MRI and CT can distinguish angiomyolipoma from other solid renal lesions because these tumors (angiomyolipomas) typically contain fat that is visible on imaging studies. 8
Several studies have attempted to use MRI to distinguish between various subtypes of RCC. Based on intracellular lipid content, some investigators have theorized that clear cell RCC, the most common RCC subtype, may demonstrate loss of signal intensity on opposed phase images. 10 Papillary RCCs have a lower signal intensity compared with normal cortex because of hemosiderin deposition as well as a more homogeneous appearance. 11,12 A more recent study, using dynamic contrast-enhanced MR imaging, was able to distinguish clear cell RCC from papillary RCC with 93% sensitivity and 96% specificity. 13 Although the possibility of making these distinctions using imaging alone is interesting, it is unclear whether pretreatment knowledge of RCC subtype is clinically useful.
Staging of RCC
The most commonly used staging system for the evaluation of RCC is the TNM staging system, developed by the American Joint Committee on Cancer. 8,14 Staging criteria in this system include tumor size, confinement to the kidney, extension into perinephric and/or renal sinus fat, extension into the adrenal gland, violation of Gerota's fascia, invasion of the major vessels (i.e., renal vein and/or vena cava by either tumor or thrombus), nodal spread, and distant metastatic spread. In a study of 40 patients who underwent surgery for RCC, Ergen et al 14 demonstrated that agreement between MRI and surgical pathology was good for assessment of T-staging (κ > 0.7), good for M-staging (κ > 0.65), excellent for venous involvement (κ > 0.9), but poor for evaluation of nodal spread (κ > 0.13).
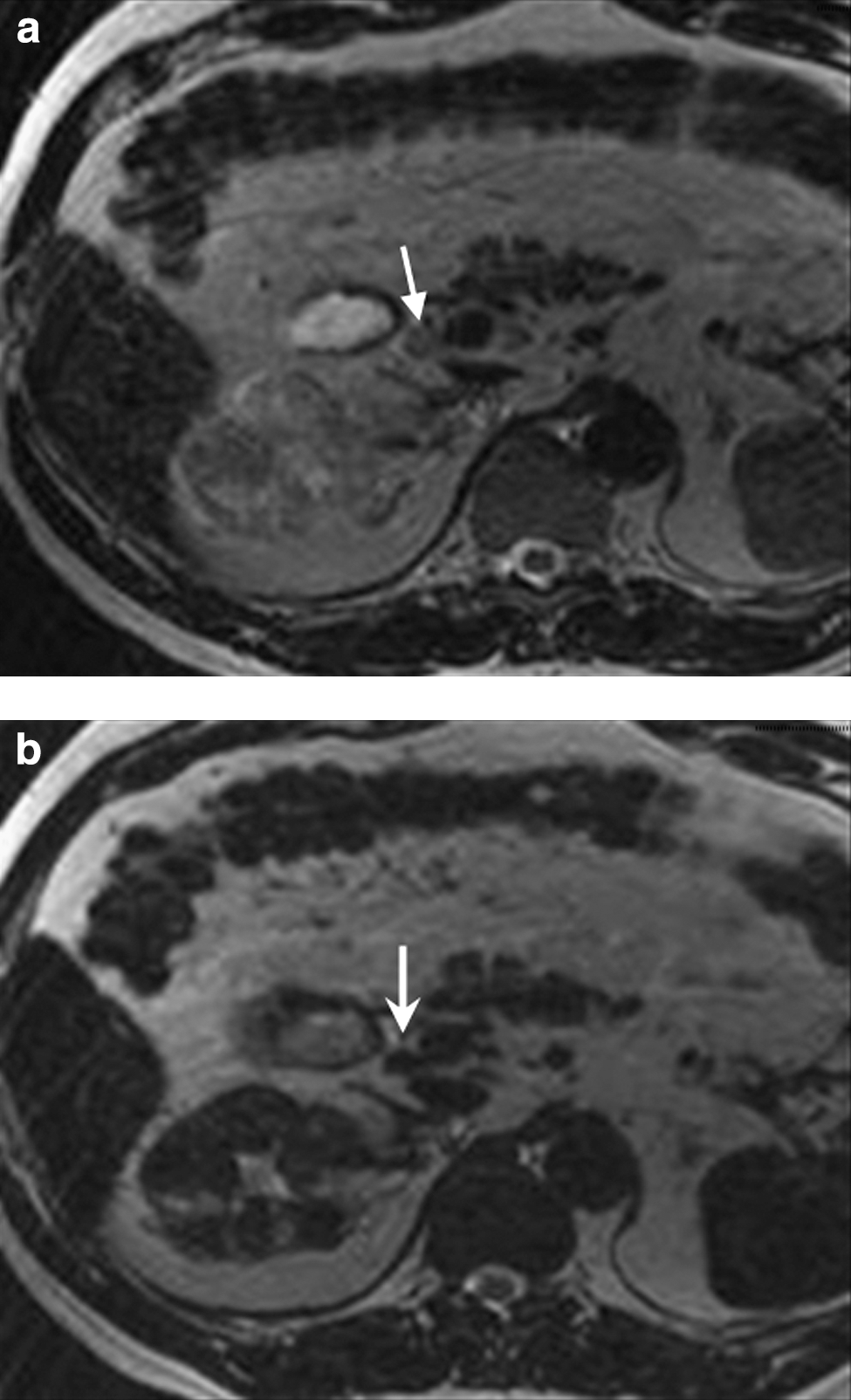
A recent study using MRI with a novel contrast agent, lymphotropic ultrasmall iron oxide particles, examined the sensitivity and specificity for detection of nodal metastases in RCC. Known as lymphotropic nanoparticle-enhanced MRI (LNMRI), this technique has been successfully applied to nodal imaging of other genitourinary cancers, with increased sensitivity and specificity compared with standard contrast-enhanced CT or MRI. 15 Within lymph nodes, these particles are engulfed by macrophages, resulting in changes in magnetic properties when imaged by MR. 15 Guimaraes et al 16 demonstrated that in patients who underwent radical nephrectomy with lymphadenectomy for RCC, LNMRI demonstrated 100% sensitivity and 95.7% specificity for detection of malignant nodal spread. Although further studies are necessary to confirm theses results, LNMRI remains a promising technology for assessing nodes in RCC. Figure 1a and b demonstrates pre- and postcontrast images of an LNMRI study demonstrating malignant lymph node infiltration.
(
MRI has been most useful in determining the presence and extent of vascular invasion from RCC. 17 –19 The ability to accurately assess the degree of vascular invasion is of particular importance in surgical planning, as the presence and location of the tumor thrombus determines the surgical approach in many cases—thrombus above the liver requires mobilization of the liver, whereas extension into the right atrium may require cardiopulmonary bypass with hypothermic arrest. Figure 2 demonstrates a left renal tumor (straight arrow) with renal vein extension (bent arrow). As described above, Ergen et al 14 demonstrated the excellent ability of MRI to determine the presence and extent of vena cava involvement for RCC. In a comparison of MRI and CT for patients with suspected tumor thrombus, Hallscheidt et al 18 showed equivalent results of the two modalities in assessment of tumor thrombus presence and location. Aslam Sohaib et al 17 reported on 12 patients with RCC and vena caval thrombus—MRI detected the extent and nature of the vena caval thrombus with a sensitivity of 100% and specificity of 89%. Another study used MRI measurements of inferior vena cava diameter and renal vein ostium diameter to determine a cutoff value with 90% sensitivity for prediction of vascular wall invasion by tumor. 19 MR has also been used to differentiate bland thrombi from tumor thrombi, with gadolinium enhancement indicating presence of tumor, and lack of enhancement suggesting bland thrombus. 20
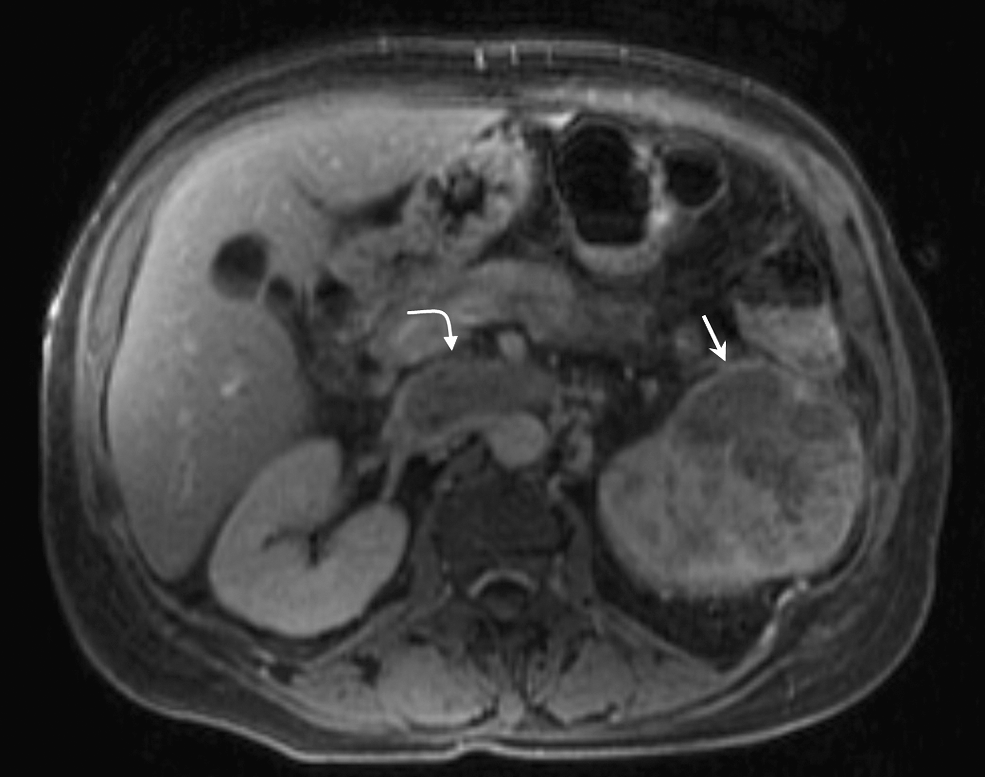
MRI showing left renal lesion (straight arrow) and renal vein invasion (curved arrow).
Cystic Renal Lesions
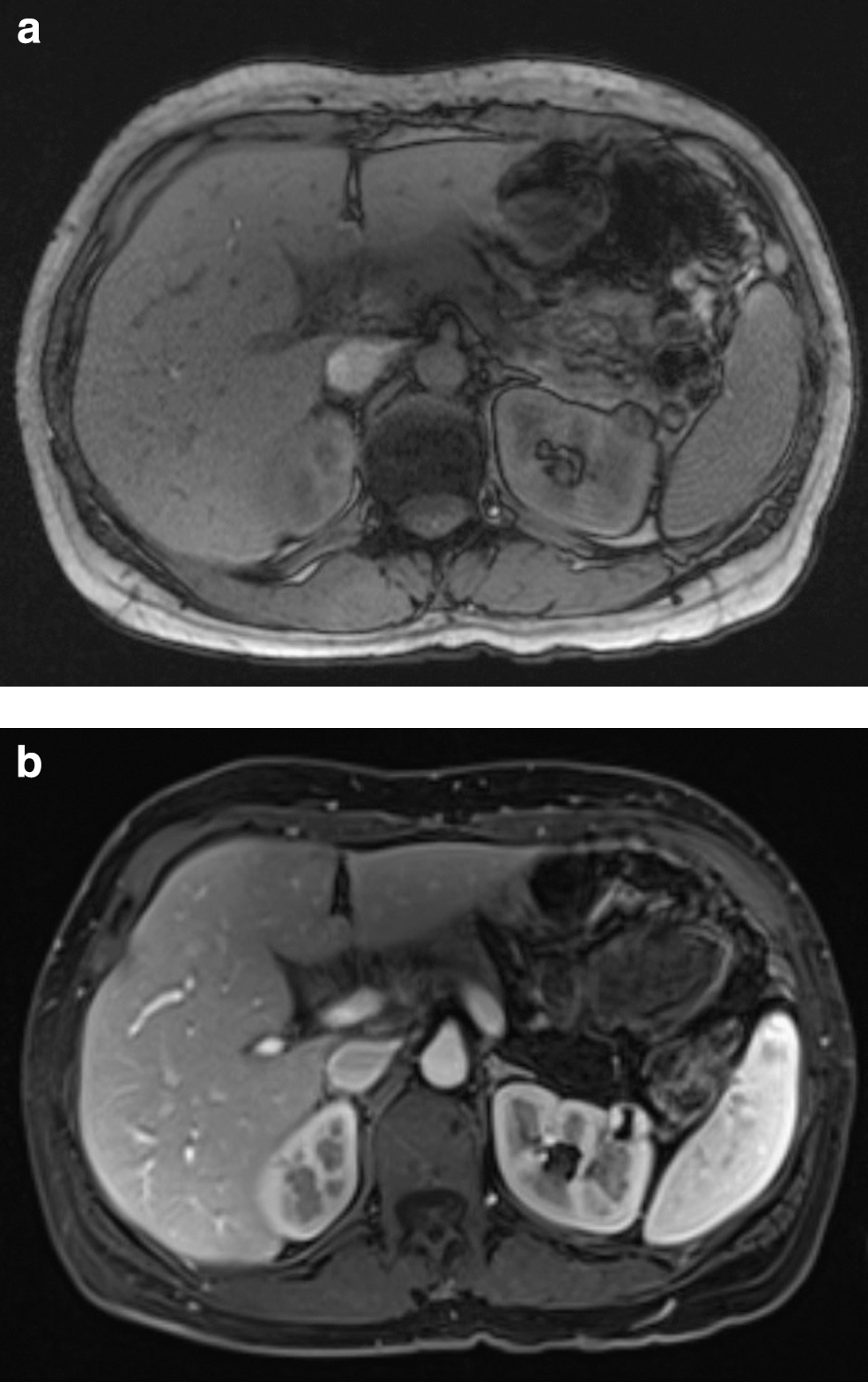
The Bosniak classification of renal cysts, first introduced in 1986, is a CT-based system used by radiologists and urologists to determine the malignant potential of cystic lesions of the kidney. Briefly, the Bosniak system classifies cysts ranging from benign simple cysts (Bosniak I) to malignant cystic RCC (Bosniak IV). 21 The most clinically challenging cystic lesions, however, are Bosniak IIF and Bosniak III complex cysts—those which are too complex to consider uniformly benign, but which require follow-up. Up to 50% of Bosniak III cysts may be malignant. 22 Like RCC, CT has been the historic study of choice to evaluate renal cysts. 21,23 One recent study compared MRI with CT in the evaluation of 69 cystic renal lesions. 21 They reported similar findings in the majority of cases, but MRI upgraded classification of seven lesions (II to IIF in two cases, IIF to III in three cases, and III to IV in three cases). Upgrading was a result of the enhanced detection of the number of internal septa and increased detection of abnormal septal and/or wall thickness by MRI. 21 In this single study, it appears that MRI may have increased sensitivity for cyst complexity, but the clinical and pathological relevance of this finding is unknown. Figure panels 3a and 3b are MRI images of a left anterior thick-walled renal cyst pre- and postcontrast administration.
(
Percutaneous Ablative Therapy
Recently, ablative therapies such as radiofrequency ablation (RFA) and cryoablation have gained widespread acceptance in the treatment of small enhancing renal masses and for treatment of renal lesions in patients who may be medically unfit for more invasive surgical procedures. For smaller tumors (i.e., <4 cm), 5-year oncological outcomes appear favorable, though the efficacy of ablative treatment for larger tumors and the durability of results over the longer term is yet to be determined. 24 –26
RFA and cryoablation have been performed using both laparoscopic and percutaneous image-guided techniques. In percutaneous procedures, MRI and CT have both been used successfully, without a clear oncologic advantage of one modality over the other. 24,25,27 However, there are several theoretical advantages of MRI over CT for percutaneous ablative procedures other than lack of ionizing radiation: MRI's high soft tissue contrast, true multiplanar imaging, and the ability to assess for ablation outcomes without the need for additional intravenous contrast. After RFA, the ablation cavity becomes T2 hypointense compared with the isointense or hyperintense RCC signal previously seen, and the region is generally isointense to hyperintense on T1 sequences. In patients treated with RFA, most will develop a hyperintense rim, or peritumor halo, whereas incompletely treated areas remain hyperintense on T2 sequences, and would appear as T1 enhancing lesions if gadolinium was administered. 28 –30 With respect to cryoablation, MRI reveals the iceball with a high degree of precision because ice has a very short T2 relaxation time. This results in a quick, distinct delineation between ablated and nonablated tissues, and guidance to the operator regarding the completeness of the ablation and in this respect may provide advantages over CT-guided cryoablation. 31
MRI has also been useful in the follow-up of patients who have undergone percutaneous ablative therapies. RFA and cryoablation appear to have similar MRI appearances postablation. 29,32 Specifically, contrast enhancement is eliminated in the ablation zone. Within the first month after ablation, it is not uncommon to see rim enhancement of the recently treated renal mass—this is a typically benign postprocedure change and should be distinguished from nodular enhancement, which should raise suspicion for recurrent tumor. 29,32
Assessment of Response to Antiangiogenic Therapies
Recently, a technique called MRI arterial-spin labeling (ASL) has been used in animal models and humans to assess the response of RCC to antiangiogenic therapies, which are the mainstay of treatment for advanced or metastatic RCC. ASL uses nuclear spins of endogenous water in blood, which are used to quantify flow. In one study, mouse RCC xenografts were examined and blood flow before and after treatment with sorafenib was successfully quantified. 33 In humans, ASL demonstrated a decrease in blood flow (which was strongly correlated with change in tumor size) in 10 patients treated with the tyrosine kinase inhibitor PTK787/ZK 222584, suggesting that MRI ASL may be useful as an early predictor of clinical response to antiangiogenic therapies. 34 Further studies are necessary to confirm the validity of this technique.
Adverse Reactions: Nephrogenic Systemic Fibrosis
The adverse reaction known as nephrogenic systemic fibrosis (NSF) deserves mention. First described by Grobner, 35 NSF is a systemic nephrogenic fibrosing dermopathy that can occur in patients with renal insufficiency who are given intravenous gadolinium. NSF can be progressive and even fatal in severe cases, and there is no specific treatment for this condition. The Food and Drug Administration recommends that caution be used when considering gadolinium administration to patients with severe renal compromise (glomerular filtration rate <15 mL/min). 6,35
Conclusions
MRI is a useful imaging modality in several aspects of the evaluation and treatment of RCC. Its most established use is in the assessment of vascular spread of RCC to the renal vein and vena cava. MRI can successfully differentiate cystic from solid renal lesions, and also is accurate in determining the complexity of renal cysts. It has been used successfully to guide and follow percutaneous thermal ablative procedures. Promising preliminary results have been shown with new techniques such as LNMRI and ASL. As these and other technologies continue to evolve, MRI will remain an important tool in the assessment and treatment of patients with RCC.
Footnotes
Disclosure Statement
Brian Eisner is a speaker for Boston Scientific, a consultant for The Ravine Group and Perc Sys. Michael Kurtz and Mukesh Harisinghani have no disclosures to report.