
Abstract
Introduction:
Stenting is the best approach to manage ureteral extrinsic compression and depends on intraluminal patency, which is mainly determined by cross-sectional stability. We evaluated the resistance to extrinsic compression of the Silhouette® Scaffold Device and its ability to simultaneously maintain intraluminal flow.
Materials and Methods:
Four 8 F Silhouette stents of different lengths were evaluated for radial compression and intraluminal flow by an MTS Micro Bionix Testing System using Testworks II software. Compression was exerted in 0.2 mm increment cycles until a maximum load cell of 5 N was reached. The Young's modulus, E, was calculated from each trial using engineering stress. Flow rates were compared with the 10.2 F Cook Amplatz. Analysis of variance was used to detect differences between Scaffold stents, and Student's t-test for differences between baseline flow rates. A level of significance of p < 0.05 was used.
Results:
Cross-sectional area and E did not differ throughout different length Scaffold stents (average 28,856 ± 2592; 95% confidence interval 27,447, 30,265; p = 0.426). The inner lumen of the 10.2 F Cook Amplatz was larger by 0.125 mm. Baseline flow rate of the Cook Amplatz was significantly higher than that of the Silhouette Scaffold (1.089 vs. 0.660 mL/second, p = 0.001), but the drop in the flow rate was four times faster for the Amplatz.
Conclusion:
The resistance of 8 F Silhouette Scaffold Device is extremely higher than that of previously tested stents, and it is uniform along the shaft and does not vary with length. The Cook Amplatz 10.2 F stent has higher flow at baseline and 2 mm compression, but its flow rate drops four times faster than the Silhouette Scaffold.
Introduction
Ureteral obstruction is related to several different advanced pelvic malignancies and is believed to contribute to patient suffering and negatively impacts quality of life. 1
Urinary drainage in this setting was first described by Gibbons et al 2 in 1976. Whether or not to perform urinary drainage should be an individualized decision 1 and can be executed percutaneously with the use of a nephrostomy tube or through endoscopic transurethral retrograde placement of a ureteral stent. Controversy still exists on which approach renders the best benefit, but many elect stenting as the procedure of choice based on the advantages of decreased morbidity, better patient tolerance, minimally invasive nature, and avoidance of external urinary appliances. 3,4 In addition, percutaneous access to the renal pelvis may be challenging in obstructed nondilated collecting systems. 5
When stent placement is selected, the most important endpoint is satisfactory maintenance of urinary flow. Authors have diverged about the exact mechanism of urine passage whether it be through the stent 6 or around it. 7 However, in the context of extrinsic compression, intraluminal flow is believed to be predominant. 8 As such, intraluminal patency is the corner stone to assure successful urinary drainage and may ultimately be most dependent on the stent cross-sectional stability. 9
Resistance to extrinsic compression forces has previously been reported on several different commercially available Double-J stents, but little has been reported on the effects of increasing obstruction on intraluminal flow. 10 –12
We performed an in vitro study to evaluate the ability of a coil-reinforced ureteral stent (Silhouette® Scaffold Device; Applied Medical, Rancho San Mirage, CA) to maintain intraluminal flow under increasing extrinsic mechanical compression. We compared flow rates with the 10.2 F Cook Amplatz stent.
Materials and Methods
Four ureteral coil-reinforced Double-J stents of the same diameter (8 F) but different lengths (22, 24, 26, and 28 cm) were tested (Silhouette Scaffold Device) for radial compression and intraluminal flow. An MTS Micro Bionix Testing System and Testworks II software, 5 N load cell, vibration isolation table, and socket set screws with rounded caps were used for measurements (Fig. 1). Radial compression was exerted in 0.2 mm increments up to the maximum load cell of 5 N. Cycles of compression with a 100-second hold time in between were repeated for each stent in three different segments (proximal, mid, and distal).

MTS compression setup.
The Young's modulus, E, which is the proportionality constant of stress to strain, was calculated for each trial under compression. E represents the stiffness of the stent. Engineering stress was used for all calculations. Simultaneous flow data using physiologic saline at room temperature were recorded as well. Flow data were recorded during compression cycles for 20 seconds. The saline bag was hung approximately 48 inches above the stent level, and a 14-gauge needle was used to couple the saline tubing to the stent (Fig. 2). Saline was collected in a recipient and its weight measured with a digital scale; 1 g is equivalent to 1 mL of fluid, during each compression cycle, as previously described by Hendlin et al. 11 Flow rates were compared with the 10.2 F, 30 cm Cook Amplatz ureteral stent.

Tubing connection to assess intraluminal flow.
Cross-sectional area of the stents was calculated using multiple measurements from the outer diameter, and wall thickness of each stent taken with a digital caliper.
Statistical analysis was performed using analysis of variance to detect differences between Scaffold stents. Student's t-test was used to assess differences between baseline flow rates. A level of significance of p < 0.05 was used.
Results
Cross-sectional area did not differ among Scaffold stents of different lengths (average 3.69 × 10−6 mm2, range 3.54 × 10−6 to 3.95 × 10−6; p > 0.05). The inner lumen of the 10.2 F Cook Amplatz stent was larger than that of the Scaffold by 0.125 mm.
Intraluminal flow data of the Applied Scaffold showed little variability throughout the compression cycles. No linear correlation was found and no differences between stents were shown (p = 0.426). Table 1 summarizes the E values (Young's modulus) for the four different-sized Scaffold stents.
Scaffold Stent Lengths and Young's Modulus (E)
Baseline flow rate of the Cook Amplatz was significantly higher than that of the Silhouette Scaffold (1.089 vs. 0.660 mL/second, p = 0.001). As compression progressed, the drop in flow rate was over four times faster for the Amplatz than the Silhouette. However, even after 2 mm compression, the powered trendline for the intraluminal flow demonstrated superior flow with the Amplatz stent. Equivalence in flow was reached (0.599 vs. 0.612 mL/second, p > 0.05) after 1 mm compression at 5 N for the Silhouette and 2 mm compression at 4.3 N for the Cook Amplatz (Fig. 3). Compression beyond 1 mm was not possible with the Silhouette as it reached the maximum load cell capacity of 5 N, but reverse calculation allows for an estimate of 14.5 N to reach a 2 mm compression.
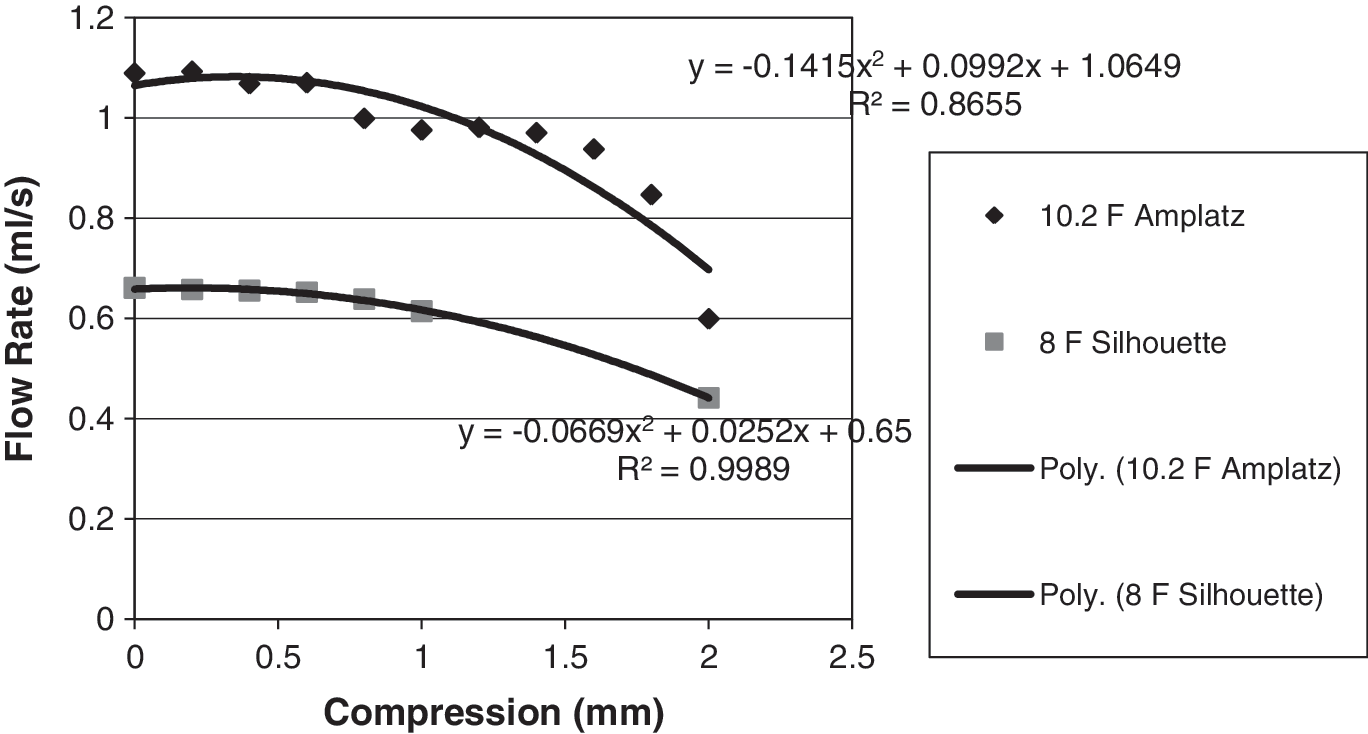
Inner lumen flow rate.
Discussion
When managing ureteral obstruction caused by extrinsic compression from advanced pelvic malignant diseases, stenting is a common first-line approach. 4 The maintenance of its patency is crucial for success, but high early failure rates have been reported and reach up to 58%. 1,8,13 Factors related to stent failure have been described and include stent encrustation and luminal obstruction caused by debris and mucus. 8 Also, since open flow dynamics predominates in this setting, failure to maintain cross-sectional stability leads to a decrease in urine flow. Hendlin et al 11 confirmed this theory when analyzing the 10.2 F Cook Amplatz stent. Despite its larger luminal width, the 10.2 F Cook Amplatz stent was the most susceptible to extrinsic compression in this series, unable to maintain its radial diameter and therefore its inner flow, which decreased at a rate of 5 mL/second/mm in a linear fashion.
Alternatives to overcome this problem have been attempted and include placement of tandem Double-J stents, 14 metal mesh stents, 15 and, more recently, coil-reinforced ureteral stents. 9 Parallel tandem Double-J stents are believed to allow for urine drainage between the two stents and to offer more resistance to kinking without worsening irritative symptoms compared with a single Double-J. However, ureteral narrowing may not allow for placement of two stents simultaneously. 13
Metal mesh stents may offer the advantages of greater resistance to compression compared with regular stents 12 but usually require balloon dilation before its placement. 1 A second major concern on follow-up is the risk of intraluminal obstruction caused by reactive hyperplasia. 4 Hardness of material was reported to be a more important feature than luminal diameter in the maintenance of flow through the stent. 9,13,16 The coil-reinforced Applied Silhouette 4.6 F stent has been previously shown to offer a resistance to outside compression at least twice that of previously tested non-coil-reinforced stents while maintaining flexibility of the durometer similar to other stents. 9 Our study demonstrates that the current 8 F Applied Silhouette Scaffold Device maintains its intraluminal flow under increasing compression cycles, being able to resist higher compression forces compared with the 4.6 F version (28,856 ± 2592 kPa vs. 105 ± 11 kPa, respectively). When compared with 10.2 F stents, its outside diameter is smaller (2.667 mm vs. 3.327 mm), whereas the inside diameter is claimed to be equivalent (1.930 mm in both). In our study, however, we found the Amplatz to be larger by 0.125 mm. This might explain why its baseline flow is significantly higher than that of the Silhouette Scaffold Device. Similarly, the Amplatz 10.2 F stent maintained a superior intraluminal flow at maximal compression.
On the other hand, the drop in the flow rate of the 10.2 F Cook Amplatz was shown to be four times higher than that of the 8 F Silhouette under continuous and increasing extrinsic compression. This study suggests the need for a 10 F coil-reinforced stent that not only provides resistance to extrinsic compression, but also matches the maximal flow characteristics of a traditional larger-caliber ureteral stent.
Conclusion
The 8 F Silhouette Scaffold Device proved capable of maintaining intraluminal flow despite increasing extrinsic compression. The Cook Amplatz 10.2 F stent has a higher flow at baseline and at 2 mm compression, but its flow rate drops four times faster than that of the Silhouette Scaffold. As such, development of a larger-caliber coil-reinforced ureteral stent may be warranted.
Footnotes
Acknowledgments
We thank and acknowledge the help of our nursery team at the Stone Disease Clinic at the University of Minnesota.
Disclosure Statement
No competing financial interests exist.