
Abstract
Purpose:
Laparoscopy-assisted radical nephrectomy and vena caval thrombectomy (LARN-VCT) is reported to be an alternative to open surgery for renal-cell carcinoma (RCC). We describe our experience and review the current literature evaluating the feasibility and safety of LARN-VCT.
Patients and Methods:
We retrospectively reviewed the medical records of all patients who underwent laparoscopic radical nephrectomy for RCC at our institution between June 2004 and May 2009, and selected those who underwent LARN-VCT. We analyzed patients' clinical, radiographic, intraoperative, pathologic, and postoperative parameters. For the literature review, we performed a MEDLINE search to identify publications that focused on laparoscopic radical nephrectomy with VCT.
Results:
LARN-VCT was completed in six of seven patients; elective conversion in one patient to open surgery occurred because of disease progression. Five of the six patients with RCC had no evidence of disease recurrence at a median follow-up of 16 months. The literature review revealed case reports and small series demonstrating the technical feasibility and safety of LARN-VCT in selected patients.
Conclusions:
LARN-VCT is a technically feasible approach in carefully selected patients with right-sided level II to III tumor thrombus. Optimal patient selection, extensive laparoscopic experience, and multidisciplinary support are critical elements for the safe application of this approach. Fluid and volume resuscitation must be thoughtfully considered given the transition from laparoscopy to open cross clamping of the vena cava. The worldwide literature on LARN-VCT is still limited and additional data are needed.
Introduction
Renal vein and inferior vena cava (IVC) thrombi are present in 4% to 10% of all renal tumors. 8,9 When present, these pose a unique challenge in maximizing cancer control and minimizing patient morbidity. An open approach is the standard of care in managing these tumors. However, as surgical technology continues to evolve, the focus may shift toward a minimally invasive approach, as has been the trend for kidney cancer. Many long-term studies have established the efficacy, safety, and tolerability profiles of LRN. 10,11 Currently, open surgery is indicated for patients with vena caval (level II–III) tumor thrombus involvement. However, some treatment centers have expanded their indications for a laparoscopic hybrid approach to include such cases. The international experience with this approach remains limited, however. In this report, we present the results of our series and a literature review, hoping to provide guidelines that would optimize patient selection for laparoscopy-assisted radical nephrectomy and vena caval thrombectomy (LARN-VCT).
Patients and Methods
With Institutional Review Board approval, we retrospectively reviewed the medical records of all patients who underwent LRN for renal-cell carcinoma (RCC) at the M.D. Anderson Cancer Center from June 2004 to May 2009, and selected those who had undergone LARN-VCT. We compared multiple intraoperative parameters, including age, body mass index (BMI), clinical tumor stage classification, preoperative imaging findings, estimated blood loss, operative time (defined as time from initial incision to time of closure of last incision), length of hospital stay, surgical margin status, and follow-up time and status. All patients undergoing LARN-VCT had tumor thrombus classified as level II or higher, according to the Mayo classification. 12
Laparoscopy-assisted radical nephrectomy and vena caval thrombectomy
Patients were positioned in a 60° modified lateral decubitus position with the table slightly flexed. A standard conventional LRN was performed using a four- or five-port approach as previously described, 10,13 but it was modified so that the renal vein was not ligated and minimally manipulated. Briefly, after mobilization of the colon and duodenum, the fibrofatty tissue immediately lateral to the IVC was gently retracted laterally and dissection proceeded parallel to the IVC in a cephalad direction toward the hilum. The renal artery was identified, carefully skeletonized, and controlled using locking clips or an endovascular stapler. The kidney was then carefully freed of its attachments to avoid disrupting the thrombus. The ureter was divided; the adrenal gland was dissected medially, separating it from the IVC; the adrenal vein was ligated. The LigaSure vessel sealing system (LigaSure V; Valleylab, Boulder, CO) was used to perform these maneuvers and to mobilize the renal and adrenal attachments. At this point of the LARN-VCT, the kidney was largely freed and remained attached only by the unmanipulated renal vein. All maneuvers were performed with minimal handling of the kidney.
Before surgical dissection and after the aforementioned maneuvers, intraoperative ultrasonography (IOUS) was performed using a four-way deflectable laparoscopic probe (B-K Medical, Herlev, Denmark) operating at 5 to 10 MHz to ensure that the tumor thrombus was not fractured, to confirm the location of its most cephalad extension, and to evaluate its adherence to the IVC, inferior extension in the IVC, or extension into the contralateral renal vein.
After laparoscopic mobilization of the kidney and ligation and division of the renal artery, a subcostal incision was made in a manner that would give the most direct access to the IVC by placing the laparoscope directly over the IVC and aiming it up toward the anterior abdominal wall. The incision was made without regard to the location of the ports. At this point, the kidney was attached only by its renal vein. Circumferential mobilization and skeletonization of the IVC proximal to the cephalad extension of the tumor thrombus was performed with assistance of an experienced vascular surgeon. For the one level III case and selective level II cases, entire mobilization of the liver was performed to allow suprahepatic, subdiaphragmatic control of the IVC. Caution was given to identify all lumbar and tributaries to the IVC. IVC and venous clamping was performed with a Satinsky or similar clamp, Rummel clamp, or Cosgrove flexible clamp (Cardinal Health, Dublin, OH). The Cosgrove and Rummel clamps may be passed via one of the port sites to maximize the working space. One was placed proximal to the cephalad border of the tumor thrombus. Another clamp was placed on the IVC caudal to the right renal vein and another was secured on left renal vein. If necessary, a Pringle maneuver was also performed. Cavotomy was then performed with a knife and the tumor thrombus was extracted. In one case where the tumor thrombus was densely adherent to the caval wall, it was removed with partial IVC wall excision and patch graft. The cavotomy was closed with two running 4-0 Prolene in a simple fashion. IOUS was also used throughout the open portions of the procedure to monitor the thrombus, identify its termination, and ensure distal caval control.
To assess perioperative and postoperative morbidity, we utilized the Eastern Cooperative Oncology Group (ECOG) performance status scale, American Society of Anesthesiologists physical status scale, and Charlson comorbidity index. 14 –17 Each measure has been validated separately as a tool for predicting long-term outcomes. 16,17
Literature review
For the literature review, we performed a MEDLINE search in March 2009 using the keywords such as RCC, kidney cancer, laparoscopy, IVC, tumor thrombus, and additional relevant keywords to identify publications focusing on LRN with management of IVC tumor thrombi. We selected only studies that included patients with level II or higher tumor thrombi, as management of renal vein (level 0) and short (level I) tumor thrombi is well described. This yielded a total of five publications that included both case reports and retrospective series. We then analyzed the data and present the relevant parameters in Table 2.
Results
Of the 203 patients who underwent LRN at our center between June 2004 and May 2009, 7 underwent LARN-VCT. We retrospectively reviewed and analyzed these patients' data. Preoperative imaging identified IVC tumor thrombi in all patients, except for one. In this patient, both a thin-slice spiral computed tomography scan and magnetic resonance angiogram failed to definitively show a tumor thrombus. At the time of surgery, IOUS revealed wispy, mobile strands of tissue within the IVC emanating from the renal vein. The patient underwent LARN-VCT as described above, and the entire intracaval tumor was resected. Postoperative chest imaging showed what was missed on preoperative chest imaging: the tumor had embolized at initial presentation, before surgery, and in retrospect, the residual wispy tumor thrombus tissue was too thin and mobile to be reliably identified on the preoperative abdominal imaging studies. Thus, we performed the first LARN-VCT incidentally. This provided the impetus for additional exploration in selected patients. Representative cases demonstrating imaging and intraoperative and postoperative findings are shown in Figures 1 to 3.
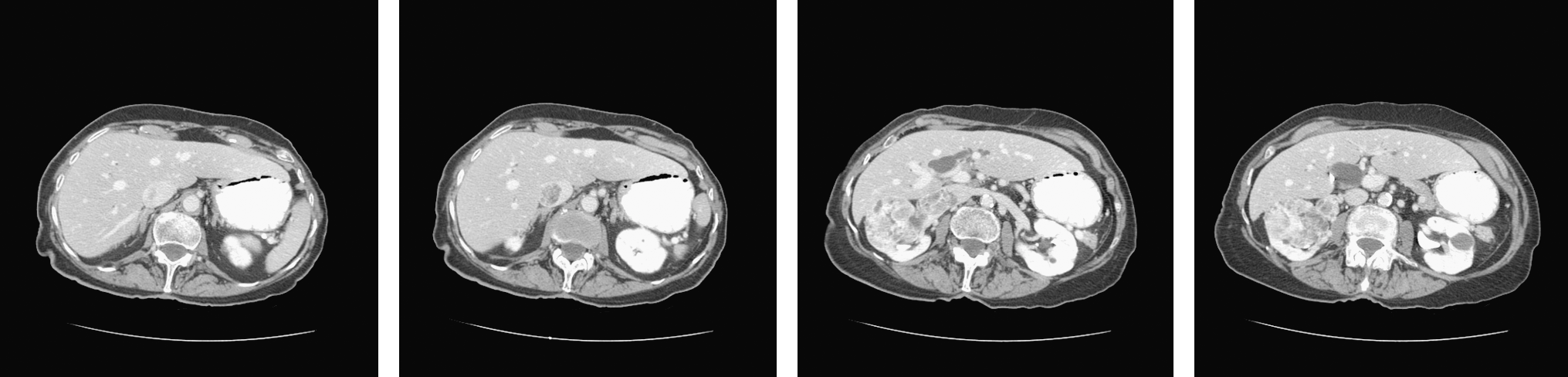
Computed tomography scans of an 89-year-old patient with renal-cell carcinoma and level III IVC tumor thrombus, extending to approximately 2 cm below the convergence of the hepatic veins. IVC = inferior vena cava.
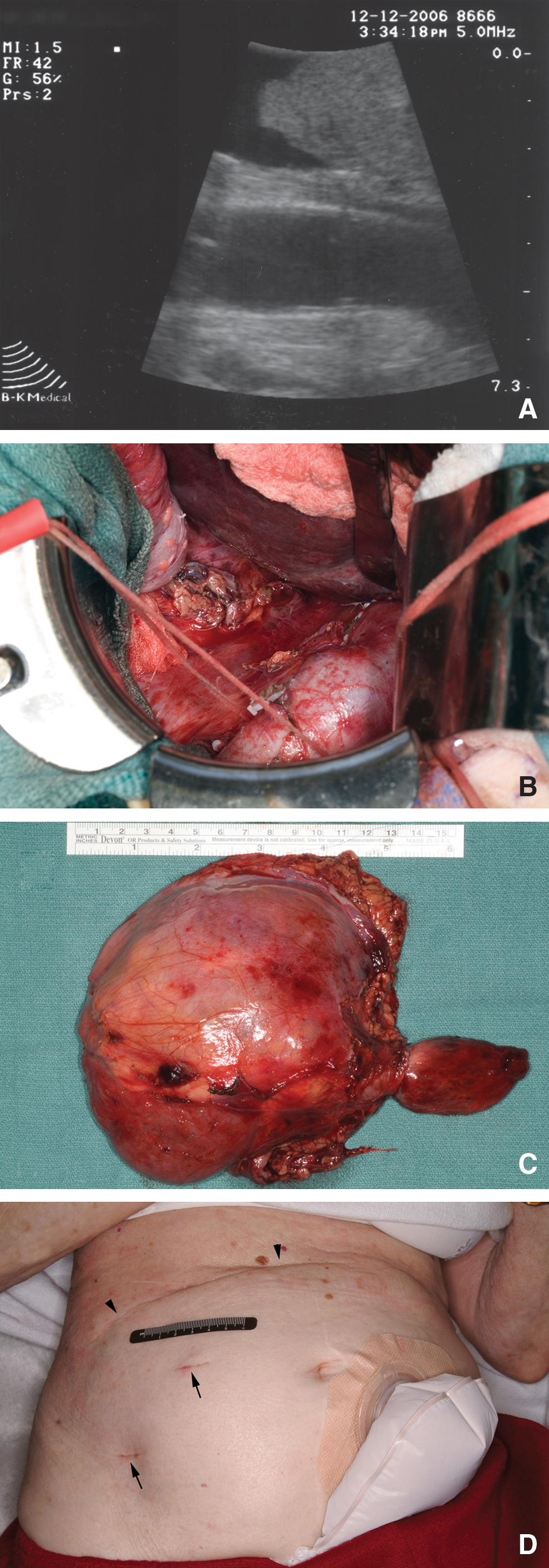
Intraoperative photographs from patient shown in Figure 1. (

(
Patient demographics and intraoperative, pathologic, and postoperative parameters are shown in Table 1. The median age and BMI was 66 years (range 54–89 years) and 30.5 (range 18.6–37.8), respectively. The median tumor size was 9.1 cm (range 5.7–12.8 cm), and all tumors were on the right side. The median incision used for IVC thrombectomy was 12 cm. Most patients in this series had multiple comorbidities, placing them in the high-risk category for surgical intervention. The median American Society of Anesthesiologists score was 3 (range 2–4). Three of seven patients had an ECOG score of 2. The median weighted index of comorbidity and the combined condition and age-related scores were 5 (range 2–8) and 7 (range 4–10), respectively.
The three numbers represent weighted index of comorbidity, combined condition and age-related score, and estimated 10-year survival, respectively.
Primary lung cancer metastasized to the kidney.
Electively converted to open surgery because of significant progression of disease and invasion of vena caval wall.
ASA = American Society of Anesthesiologists; ATN = acute tubular necrosis; BMI = body mass index; BPH = benign prostatic hyperplasia; CAD = coronary artery disease; CHF = congestive heart failure; COPD = chronic obstructive pulmonary disease; DM = diabetes mellitus; EBL = estimated blood loss; GERD = gastroesophageal reflux disease; HTN = hypertension; LOS = length of hospital stay; NSTEMI = non-ST segment elevation myocardial infarction; OA = osteoarthritis; OR = operating room; PS = performance status (Eastern Cooperative Oncology Group classification).
Perioperative data are also shown in Table 1. Median operative time was 240 minutes (range 159–330 minutes), with a median estimated blood loss of 600 mL (range 400–4850 mL). Patients with larger (>8 cm) primary tumors had significantly higher blood loss. In one patient, LARN-VCT was converted to open surgery because of significant tumor progression and invasion of the caval wall (Table 1). Pathologic evaluation revealed primary RCC in six of the seven patients and primary lung cancer with metastasis to the kidney in the remaining patient. All surgical margins were negative. For the four patients without complications, the median length of hospital stay was 5 days; however, for those with complications, the hospital stay was 17 days. The primary complications were related to fluid management. Our first patient developed postoperative acute tubular necrosis, likely secondary to inadequate intraoperative volume resuscitation (see Discussion section). In the other two patients, the complications likely were related to intraoperative over-resuscitation. Follow-up times ranged from 3 to 42 months (median 16). No patients were lost to follow-up. Five of the six patients with primary RCC had no evidence of disease at the time of analysis. Of the two patients with disease progression, the patient with RCC eventually died of the disease; the other patient, with primary lung cancer, began chemotherapy for recurrent lung cancer.
Table 2 summarizes the results of a literature review. The initiative to further expand minimally invasive surgical procedures began with animal studies. In 2002, Fergany and colleagues 18 reported the first successful porcine survival study demonstrating the technical feasibility of a purely laparoscopic approach for tumor thrombectomy. Clinical data have mostly focused on patients with level I tumor thrombi. For instance, Sundaram and colleagues 19 reported the first human case of hand-assisted nephrectomy for RCC with level I tumor thrombus. Dissection of the kidney and control of major vessels was accomplished with manual assistance; IOUS was used for thrombus demarcation. The hand-assisted port incision was extended to 11 cm to facilitate specimen extraction. Even though the patient later died of a myocardial infarction, this study by Sundaram and colleagues 19 demonstrated the technical maneuvers and challenges involved in this procedure. Shortly thereafter, Varkarakis and colleagues 20 retrospectively reviewed and published the preliminary results of their experience with LARN-VCT. In their study, four carefully selected patients with RCC and level I tumor thrombus underwent LARN-VCT. Unlike the technique employed by Sundaram and colleagues, 19 Varkarakis and colleagues 20 elected to mobilize the kidney and major vessels, including the IVC, laparoscopically. IOUS was used for thrombus demarcation. Modified flank incisions, ranging from 8 to 12 cm, were made for specimen extraction. No intraoperative or postoperative complications were reported. All patients were doing well at 6-month follow-up. The authors concluded that additional studies were needed to validate the advantages of this laparoscopic hybrid approach over the traditional approach.
Includes all patients and all outcomes, including complications and conversions.
NA = not available; RCC = renal-cell carcinoma; OR = operating room; LOS = length of stay; MI = Myocardial infarction; BMI = body mass index; ASA = American Society of Anesthesiology; EBL = estimated blood loss.
In 2006, Romero and colleagues 13 reported the first successful case of a purely laparoscopic approach for level II IVC thrombus. They attributed their success to careful patient selection as well as to their extensive experience performing laparoscopic renal surgeries. However, others have pointed out that this approach is unnecessary given the need for a large incision to facilitate specimen removal as well as for precise vascular control to prevent catastrophic outcomes. 20 Disanto and colleagues, 21 on the other hand, demonstrated the feasibility of retroperitoneal LARN-VCT. Their approach involved laparoscopic mobilization of the kidney and major vessels. Open surgery was then performed to facilitate safe cavotomy and thrombus extraction. Advantages with this approach included no need to mobilize the liver, duodenum, or colon and quick access to the vena cava. However, patients with a level II or higher thrombus may not be best served by a retroperitoneal approach given its limited access to the vena cava, contralateral renal vein, and other vascular structures.
Recently, Martin and colleagues 22 reported their 7-year experience with LRN for patients with renal vein and vena caval thrombus. In their study, a total of 14 patients were retrospectively identified from 2000 to 2007. Among these patients, 4 had IVC involvement. Their approach was similar to that of Sundaram and colleagues' 19 in which manual assistance with a Gelport was utilized to facilitate thrombus milking. A combination of tactile sensation and early ligation of the renal artery allowed for retraction of the thrombus, rendering IOUS unnecessary according to these authors. No intraoperative complications were reported. The authors concluded that this approach is feasible and safe in carefully selected patients.
Discussion
In this study, we add to our initial experience with LARN-VCT, and show that it is a technically feasible approach in carefully selected patients, with satisfactory outcomes in most patients. We found that patients can experience complications related to intraoperative fluid management, which reinforces the need to focus on overall patient volume rather than just fluid resuscitation. Typically, the anesthesia team restricts fluid as would be expected during laparoscopy; in these cases, however, during vena caval cross clamping, there is a significant reduction of preload. 23 Thus, with inadequate volume resuscitation before vena caval cross clamping, there can be a dramatic reduction of preload leading to prerenal azotemia. Overzealous administration of fluids can likewise be problematic. The optimal course would seem to be to provide adequate fluid resuscitation but focusing on volume expansion with colloids or blood products before vena caval cross clamping.
As with any new procedure, careful patient selection is key to optimizing the outcomes. Although our patient series is too small for statistical analysis, we observed that patients with smaller (generally <8 cm) right-sided tumors, BMI <30, and an ECOG score <2 seem to be the ideal candidates for this approach, as patients with most of these criteria were the ones not experiencing any complications. Patient 7 had a 10.5 cm tumor but had all other favorable criteria. Thus, patients who do not meet most of these criteria may not have optimal outcomes, and for them the best method may be open surgery. Cases with higher BMI can be more difficult, and those with a poor performance status preoperatively are likely to recover more slowly with any approach, although arguably these types of patients may have the most to gain from a minimally invasive approach. Further advances in technology or technique may be able to overcome these barriers.
Our approach involved laparoscopic mobilization of the kidney and ligation of the artery, followed by a subcostal incision created for cross clamping of the vena cava and left renal vein, cavotomy, thrombectomy, en bloc intact specimen extraction, and caval repair using traditional techniques. The size of the incision needed for these vascular maneuvers was minimal, since all mobilization was performed laparoscopically. This combination allowed for safer vascular control than what is possible with a pure laparoscopic approach, yet it shortens recovery time by minimizing the incision. A pure laparoscopic approach is not needed given the considerable size of these tumors and the need for an incision for complete specimen extraction. Given the known severe consequences of massive hemorrhage and air and tumor thrombus embolism with inadequate IVC control, we believe that open IVC thrombectomy allows for the best vascular control possible, using currently available instruments. This report is limited by the retrospective nature of the study and by a small patient cohort, although it represents about a third of the currently published total experience (Table 2).
As mentioned, because of the small number of patients and high selectivity, a direct comparison of our study patients to a contemporary cohort of open patients is not feasible at this time. However, in a retrospective study by Kaplan et al 24 evaluating surgical outcomes of 11 patients who had undergone open radical nephrectomy with IVC thrombectomy for level I to III tumor thrombus, they reported a mean operative time of 3.6 hours (range 1.5–5.5 hours), mean length of hospital stay of 14 days (range 4–48 days), mean blood transfusion of 4.5 units (range 3–9 units), a 9% mortality, and a 27% complication rate. In a more recent 2005 retrospective study by Parekh et al 25 evaluating 49 patients with mostly level I to III RCC tumor thrombus, similar perioperative outcomes were also reported (median blood loss 950 mL, mean blood transfusion 6 units, median length of stay 6 days, mortality 8%, and complication rate 45%). Our current data compare favorably with these reports.
Patient selection is exceedingly important to ensure successful outcomes. Tumors larger than 8 cm are much more difficult to manage with LARN-VCT, as safe mobilization of the kidney is difficult and there is a lack of adequate working space during the open portion of the case. Other equally important factors include the surgeon's laparoscopic experience as well as his/her experience with vascular dissection, the assistance of a vascular surgeon, and a skilled anesthesia team anticipating the potential physiologic changes. IOUS provides effective monitoring of the tumor thrombus during both the laparoscopic and open portions of the procedure, while avoiding needless handling of the renal vein and IVC before cross clamping.
Conclusions
LARN-VCT is a technically feasible approach in carefully selected patients with right-sided level II to III tumor thrombus. Optimal patient selection, extensive laparoscopic experience, and multidisciplinary support are critical for the safe application of this approach. This includes patients with right-sided tumors <8 cm, BMI <30, and an ECOG score <2. Volume resuscitation must be thoughtfully considered given the transition from laparoscopy to cross clamping of the IVC. The overall international experience with this procedure is still very limited. With further technical advances and more experience, LARN-VCT can improve the perioperative and long-term outcomes of patients with locally advanced RCC.
Footnotes
Disclosure Statement
No competing financial interests exist.