
Abstract
Purpose:
Deviceless hand-assisted laparoscopic living donor nephrectomy is an alternative surgical technique that relies on the classic laparoscopic approach, supported by insertion of the surgeon's hand during kidney recovery without the need to use any device because of the sealing effect of the particular wall incision.
Patients and Methods:
From 2006 to 2008, deviceless hand-assisted laparoscopic living donor nephrectomy was performed in 25 patients (M/F = 7/18; mean age = 53 years; range = 30–68). One right nephrectomy was performed. We made a lateral paramedian incision. No sealing device is required in our technique because the pneumoperitoneum is maintained by the sealing effect of two complexes: the peritoneum/deep rectus abdominis muscle fascia and muscle itself/lateral edge of the double fascial incision. These structures clench around the surgeon's wrist, preventing leakage of CO2. After dissection, the kidney is removed through the hand port without an endobag.
Results:
Mean surgical time was 105 minutes (range = 60–150), estimated blood loss was 50 to 200 mL, and mean warm ischemia time was 3.5 minutes (range = 2–11). Mean hospital stay was 4 days (range = 3–6). One uncontrollable hemorrhage due to a renal vein lesion required conversion to open surgery. As to graft function, recipient serum creatinine on day 7 ranged from 0.8 to 2.6 mg/dL.
Conclusions:
The ability to better control bleeding by manual compression, as well as the advantages related to decreased donor morbidity, shorter hospital stay, cost saving, and excellent graft function, make this deviceless technique a good option for kidney recovery.
Introduction
Patients and Methods
Donor characteristics
We retrospectively analyzed data on 25 consecutive deviceless HA-LDN performed in renal donors (18 women and 7 men, with a mean age of 53 years, range 30–68 years), from April 2006 to December 2008 (Table 1). Donor body mass index ranged from 22 to 35 kg/m2 (mean = 28.5). Preoperative serum creatinine was 0.7 to 1.5 mg/dL (mean = 1.1). Left nephrectomy was performed in 24 of 25 cases.
A three-dimensional abdominal angio-computed tomography scan was performed, to evaluate the renal vascular anatomy and for preoperative work-up.
In all the procedures, the harmonic scalpel UltraCision© (Ethicon Endo-Surgery, Cincinnati, OH) was used for dissection and coagulation of the vessels and perirenal structures.
Surgical technique
A transperitoneal approach was used for deviceless HA-LDN in all cases. After general anesthesia, patients were placed in flank position and secured to the operating table at the level of the shoulders and thighs. All the procedures were performed by the same right-handed surgeon (F.P.S.).
Incision and trocar placement
Left renal procedures
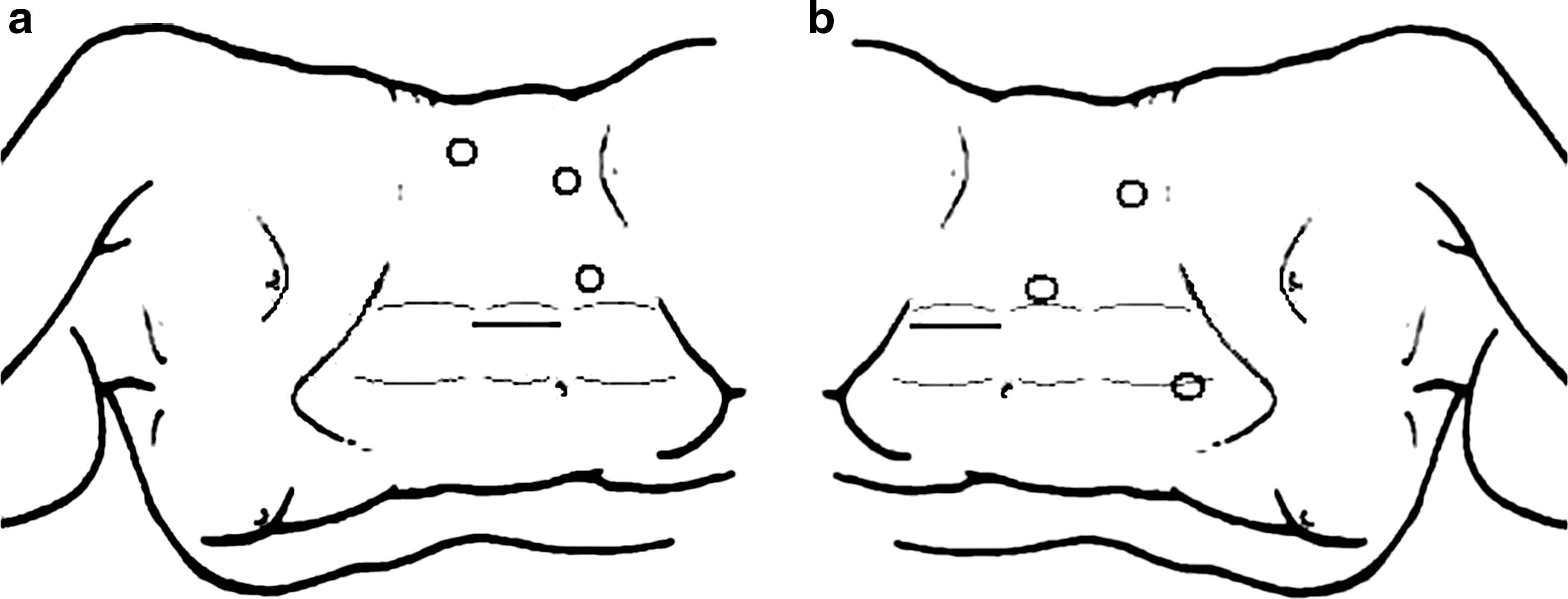
The hand-access port is placed in the left hemi-abdomen, along the left midclavicular line (Fig. 1a). A lateral paramedian vertical incision is made along the junction between the middle and superior third of the rectus abdominis muscle sheath. The skin incision must be the same size as the surgeon's wrist, ∼7 to 8 cm. The anterior rectus sheath is exposed and incised, and the edge grasped and lifted sideways. The lateral aspect of the muscle is reached and bluntly dissected from the inner aspect of its sheath up to the median third of the posterior aspect. Segmental blood vessels encountered during the dissection at the fibrous intersections are coagulated and sectioned. No important nerve structures are sacrificed.
(
Once the external half of rectus abdominis muscle is completely free, it is easy to retract it medially. The posterior rectus muscle sheath and adherent parietal peritoneum are picked up and vertically cut, 1 cm smaller than the skin incision (Fig. 2). In this way, muscle-sparing of the abdominal wall muscles is ensured, and the surgeon's left hand can be inserted inside the abdominal cavity without using any device, and indeed usually even without gel (Fig. 3).

Once the external half of rectus abdominis muscle is completely free, it is easy to retract medially (under Goulet retractor). The posterior rectus muscle sheath and adherent parietal peritoneum are picked up and vertically cut, 1 cm smaller than the skin incision.

The surgeon's hand can be inserted into the abdominal cavity without using any device.
The first 10-mm trocar, for the camera, is inserted underneath the transverse umbilical line along the left midclavicular line. After abdominal inflation, a second 10-mm trocar, for the dissecting instrument, is placed under direct vision at the level of the anterior axillary line, 2 cm above the iliac crest. An additional 10-mm trocar, the assistant port, can be inserted in the flank area for the rectractor or irrigator–aspirator cannula.
Right renal procedures
The hand access port is placed in the right lower quadrant, again performing a 7- to 8-cm lateral paramedian vertical incision along the midclavicular line, at the level of the junction between the middle and inferior third of the rectus abdominis muscle sheath (Fig. 1b). The camera port is inserted above the transverse umbilical line just lateral to the midclavicular line. The dissecting port is placed at the level of the anterior axillary line, 2 cm beneath the costal arch. The assistant port, serving to push the liver up, is inserted at the midline, immediately beneath the xyphoid process, under vision, laterally to the falciform ligament.
Nephrectomy
Left nephrectomy
Dissection is begun by dividing the left lateral peritoneal reflection along the avascular line of Toldt from the splenic flexure to the pelvic brim. The spleno-diaphragmatic and colo-renal ligaments are divided and the left colon is mobilized medially into the retroperitoneal space. Dissection proceeds along the plane between Gerota's fascia and the descending colonic mesentery until the left gonadal vein is reached.
The ureter is identified where it crosses the gonadal vein and is isolated 2 cm below the common iliac artery junction. The gonadal vein is divided inferiorly to the point where it crosses the ureter and then dissected upward to the renal vein. This is bluntly freed from the surrounding connective and lymphatic tissue up to the adrenal vein, identified in front of the gonadal vein. At this point, it is possible to clip and section both the adrenal and gonadal veins, allowing the renal vein to be freed and circumferentially mobilized in front of the aorta. The length of the renal vein is then evaluated, and if it is too short, further mobilization is done medially up to the cava. With the vein displaced cephalically, the renal artery can be located and palpated. A lumbar vein originating from the posterior aspect of the renal vein, medially and posteriorly to the gonadal vein entrance, has to be clipped and divided, remembering that it may be single or multiple, depending on the level of confluence of the three originating branches. After sectioning the lumbar vein, the origin of the main branch of the renal artery is exposed. The proximal part can be dissected up to its origin from the aorta. Before isolating the distal part of the renal artery, it is advisable to free the upper pole of the left kidney up to the superior margin of the left renal artery. Lymphatic and neural tissue of the renal hilum and adrenal attachments with the renal artery have to be divided, taking care not to injure upper pole arteries, which can be confused with the adrenal artery originating from the main branch of the renal artery. With the kidney rotated medially, all the posterior attachments, including ganglionic tissue along the posterior aspect of the renal artery and renal vein, can be divided.
After vascular preparation, the ureter can be sectioned immediately below the junction of the iliac vessels, closing the distal edge with a clip and leaving the proximal edge free to control the persistence of diuresis.
Vessel ligation and organ retrieval
To reduce the warm ischemia time (WIT) during vascular clamping maneuvers, the access sites of the Endo-GIA and clip applier are checked. While the assistant holds the lower pole of the kidney to one side using a retractor through the third port, the operator's inserted hand can lift the renal vein, facilitating clamping of the renal artery by applying Hem-o-Lok® clips and immediately sectioning it with scissors. The renal vein is then easily clipped and sectioned with a linear vascular stapler Endo-GIA (35 mm). The kidney is immediately and easily removed by hand through the incision (Fig. 4). A careful check for hemostasis concludes the operation. A small drain is left in place for 24 hours.

The kidney is immediately and easily removed by hand through the incision without an endobag.
Right nephrectomy
Dissection begins by dividing the peritoneum from the right colic groove along the line of Toldt up to the right colonic flexure, at the top, and the internal inguinal ring, at the bottom. The right colon is mobilized medially into the retroperitoneal space. Dissection proceeds along the plane between Gerota's fascia and the ascending colonic mesentery up to the right gonadal vein.
The ureter is identified where it crosses the gonadal vein and isolated up to 2 cm below the vessel junction. To obtain a better control of the upper kidney pole, the coronal ligament is incised and the liver lifted with a retractor positioned through the assistant trocar. The inferior vena cava preparation begins with sectioning of the gonadal vein, inferiorly where it crosses the ureter and superiorly where it enters the cava. This latter is bluntly freed from the surrounding connective and lymphatic tissue up to the right renal vein. Once it has been completely isolated, it is generally long enough to retrieve without using a caval patch. With the vein displaced cephalically, the renal artery can be located and bluntly isolated. With the kidney rotated medially, all the posterior attachments, including the ganglionic tissue along the posterior aspect of the renal artery and renal vein, are divided.
After vascular preparation, the ureter is sectioned immediately below the junction of the iliac vessels. The kidney, completely freed from its perirenal fat, is retrieved in the same way as described above for the left side.
Intraoperative systemic donor treatment
Intraoperatively, donors receive ample intravenous hydration with crystalloids, and before vessel clamping, 250 mL of 20% mannitol solution (to maintain optimal renal perfusion and assure a brisk diuresis both during organ recovery and after revascularization) and 2500 UI of heparin are given. Immediately after renal recovery, an adequate quantity of protamine sulfate is administered to antagonize the heparin effect.
Results
Operative data
Operative time ranged from 60 to 150 minutes (mean = 105 minutes). Estimated blood loss was 50 to 200 mL (mean = 100 mL); no patient needed a transfusion. WIT ranged from 2 minutes to a maximum of 11 minutes (mean = 3.5 minutes), the latter in two patients with a double renal artery. In one case, a renal vein lesion occurred at the outlet of the adrenal vein, requiring conversion to open surgery (Table 2).
Postoperative period
Mean hospital stay was 4 days (range = 3–6). No case of infection was observed, and no death occurred as a consequence of the procedure. Postoperative serum creatinine, which was measured at a median of 3 weeks after nephrectomy, was 0.7 to 1.6 mg/dL. Mean follow-up is now 18 months, ranging from 6 to 37 months.
Immediate diuresis after renal reperfusion was observed in all recipients and serum creatinine on day 7 ranged from 0.8 to 2.6 mg/dL (mean = 1.5), demonstrating excellent graft function.
Discussion
Open donor nephrectomy has declined in the past 15 years because of the development of laparoscopic procedures, even if it is still claimed to be the gold standard for graft recovery. 6 Laparoscopic donor nephrectomy can be performed using a variety of techniques: hand-assisted, pure laparoscopic, and robotic methods. A hand-assisted technique is particularly useful when a skin incision is necessary to remove an intact surgical specimen, as in the case of a live donor. Placement of the surgeon's hand in the operative field enables superior retraction, blunt dissection, and enhanced vascular control. If bleeding occurs, manual pressure can be easily applied, as in open surgery. When necessary, laparotomic sponges may also be introduced through the hand-port for temporary hemostasis. A slightly greater opening of the hand-port can be used for open conversion when laparoscopy fails. 7
Today, many authors consider HA-LDN as the method of choice for living donor kidney recovery because it combines the advantages of minimally invasive surgery with the security and ease of manual dissection, a short learning curve, and a reduced incidence of intraoperative complications. 3
The pneumoperitoneum is maintained by choosing a particular hand-port, in which the sealing effect is guaranteed by the muscle and fascia structures that clench around the surgeon's wrist. For placement of the hand-port, both the patient's anatomy and the surgeon's preferences play a major role in the decision as to which hand-port site must be chosen. It should be located far from the operative field to allow the hand to flex at the wrist and reach the whole surgical field.
In our technique, the sealant effect is due to both the posterior fascia of rectus abdominis muscle and corresponding adherent peritoneum, incised 1 cm smaller than the skin incision, and the contraction of the rectus abdominis muscle itself against the rigid external fascia edge of the incision. These coordinated actions cause the structures to tighten around the surgeon's wrist, provoking a sealing effect.
Before being tested in donor nephrectomy, the deviceless hand-assisted procedure was initially experimented in the removal of adrenal masses larger than 8 cm in several radical nephrectomies and nephroureterectomies, and nowadays, the devices are very rarely used during hand-assisted laparoscopic procedures in our unit. Between 2005 and 2006, we performed 32 hand-assisted laparoscopic procedures without using any device: Table 3 reports in detail our initial experience. Overall, the conversion rate due to bleeding was 6%. On the basis of this initial encouraging experience, in which the feasibility of the procedure was corroborated by low complication and conversion rates, a decision to enroll donor nephrectomy was taken.
There are possible drawbacks of this technique. An occasional gas leak due to too wide an incision has been observed but quickly resolved by tightening the hand port using a Backhaus clamp. In one case the surgeon suffered slight transient finger numbness at the end of a long procedure, because of prolonged forearm compression. No wound or deep tissue infection caused by contamination with the gowned forearm was ever observed. In all cases there was no need to remove the hand before graft removal, and if a small sponge was needed, it was introduced in the surgical field through a trocar port.
An advantage of the lateral paramedian incision is that it not only provides easy hand access to the kidney but also allows a safe closure of the fascia planes because the rectus abdominis muscle can act as a buttress between the posterior and anterior fascia, reducing the risk of an incisional hernia (Fig. 5).

Scar appearance at 3 months after surgery.
Feasibility and reproducibility are important issues when a new surgical technique is introduced. In this series, a wide range of patient's body habitus and BMI have been operated without encountering limitations for this procedure. However, even if technical difficulties were not observed, in consideration of the particular nature of a donor nephrectomy, we suggest that the surgeon should always become acquainted with any change in this procedure in other settings such as adrenalectomy or nephrectomy.
Several reports have confirmed the advantages of HA-LDN compared with open surgery for the donor. In line with this emerging evidence, in 2004 we abandoned, in favor of HA-LDN, the traditional open extrapleural and extraperitoneal approach using a modified flank incision just above the 12th rib. The preference for HA-LDN instead of the classic laparoscopic technique with manual retrieval of the organ without a device through a Pfannensteil incision is attributed to a better retraction and dissection and enhanced vascular control obtained with the manual technique, which results in a decreased technical difficulty, shorter learning curve, and a reduced rate of graft injury, estimated blood loss, and WIT. 8,9
Giving heparin to donor is a controversial issue in renal transplantation. 10 In the absence of clear literature data, we continue to use a low dose of heparin to prevent microthrombi in the graft, especially in case of unexpected prolonged WIT. In a recent survey, Wright et al 11 described that 66% of renal transplant centers with accredited fellowship programs in the United States use heparin and all of them reverse with protamine sulfate. To date, heparin use has not been associated with significant bleeding complications or impaired graft function. 10 However, protamine carries a small risk of thromboembolic stroke, anaphylaxis, and fatal pulmonary hypertension; these complications occur in cases of diabetes, multiple drug allergies, and prior protamine exposure, which are usually not candidates for living donor nephrectomy.
The self-locking mechanism has made the Hem-o-lok clips popular in many laparoscopic procedures including living donor nephrectomy. However, in the latter procedure, three deaths have been reported and in 2006 this led the manufacturer to contraindicate the Hem-o-lok clips for this use. 12,13 Despite this alert, Hem-o-lok clips are still widely used in living donor nephrectomy in many countries including the United States. A recent multi-institutional review 14 showed that when applied correctly, these clips are safe, effective, and reliable for use in all types of laparoscopic nephrectomies, including living donor procedures. The instructions for use recommend placement of two clips and maintenance of a 1- to 2-mm cuff of vessel but without subjecting the renal artery to too much tension that may result, after cutting, in a shorter-than expected vascular cuff. 15,16 In our experience, the hand-assisted technique allows the placement of two clips straightening the vascular axis without excessive and dangerous stretching.
A meta-analysis by Nanidis et al 17 comparing laparoscopic versus open live donor nephrectomy showed that open surgery had shorter operative and WITs, whereas laparoscopic nephrectomy was associated with reduced operative blood loss and analgesia, shorter hospital stay, and a faster return to work.
Although laparoscopic nephrectomy showed prolonged operative and WITs, this did not translate into an increase in recipient complications or the rate of graft dysfunction. These findings were similar when both non-hand-assisted laparoscopy and hand-assisted laparoscopic procedures were compared with open nephrectomy by subgroup analysis. Another important issue in laparoscopic surgery is the learning curve. It has been shown that with experience, the operative time is reduced, 18 –22 as is WIT 21,23 and blood loss. 22
Recently, Kokkinos et al 24 compared HA-LDN with the classic laparoscopic technique in a meta-analytical study. They showed that HA-LDN offered a quicker method of kidney recovery, as reflected by shorter operating and WITs, while preserving the donor's safety and good renal graft quality. Estimated blood loss was also an important parameter that favored HA-LDN. Subgroup analysis between hand-assisted procedures in which the hand was inserted from the beginning of the operation, 25 –30 rather than at a later stage, 31 –33 showed that intraoperative complications were decreased in the former subgroup, albeit not statistically significantly.
Advanced age and obesity, as well as renal vessel multiplicity, are not considered contraindications for HA-LDN.
Several hand-assisted devices, now commercially available, have been produced to assist this approach with a mean cost of about 500€. In fact, an important advantage of our deviceless technique is its cost-effectiveness, because the final percentage saving is as high as about 69.5% when compared with standard HA-LDN, whereas it is ∼60.5% when compared with the pure laparoscopic technique, which does not employ a hand device but requires twice as many trocars, as well as an endobag, at a further cost of about 150€ (Table 4).
dHALDN = deviceless hand-assisted laparoscopic living donor nephrectomy; Y = yes; N = no.
In conclusion, the innovative technique described in this study combines the traditional benefits of hand-assisted laparoscopy: placement of the surgeon's hand in the operative field allowing for superior retraction, blunt dissection, and enhanced vascular control, with a drastic reduction of the costs but without compromising the graft function.
At the time of organ removal, the surgeon's hand and donor kidney can be rapidly extracted through the incision with no risk of trauma. Moreover, by not using an endobag, we avoided the risk of parenchymal or renal pelvis laceration, as described with the use of this device.
Therefore, the opportunity to decrease the laparoscopy learning curve, the tactile feedback, the ability to better control bleeding by manual compression, the ability to retract tissues, as well as the advantages related to decreased donor morbidity, shorter hospital stay, cost saving, and excellent graft function quality for the recipient, make this deviceless laparoscopic technique a good option for kidney recovery for transplantation.
Footnotes
Disclosure Statement
No competing financial interests exist.