
Abstract
Introduction:
Contemporary cryoablation technology utilizes the Joule–Thomson effect, defined as a change in temperature that results from expansion of a nonideal gas through an orifice or other restriction. We evaluated the effect of initial gas tank pressures on freezing dynamics in a single-probe model and in a multiprobe model using contemporary cryoablation technology.
Materials and Methods:
Cryoablation trials were performed in a standardized system of transparent gelatin molds at 25°C. Two sets of trials were performed. The first trial evaluated temperature and ice ball size for a given tank pressure when a single needle was deployed. The second trial recorded ice ball temperatures for each probe when multiple probes were fired simultaneously.
Results:
Trial 1: The rate of temperature change is directly related to the initial pressure of the gas being released, and the group with the highest starting pressures reached the lowest mean temperature and had the largest mean ice ball size (p < 0.01). Trail 2: Multiple-probe ablation did not affect the rate of temperature change or final temperature compared with firing a single probe (p > 0.7).
Conclusions:
In accordance with the Joule–Thomson effect, higher initial gas pressures used for cryoablation in a transparent gel model demonstrate statistically significant lower temperatures, faster decreases in temperature, and formation of larger ice balls than lower gas pressures do. With contemporary technology, multiple simultaneous cryoprobe deployment does not compromise individual probe efficacy. The use of higher initial tank pressures will theoretically help future cryoprobes be more effective, creating a greater volume of cell necrosis and a smaller indeterminate zone.
Introduction
Current cryoablation technology utilizes the Joule–Thomson effect to achieve very low temperatures that result in focal freezing and destruction of local tissues. The Joule–Thomson effect describes the change in temperature that results from expansion of a gas through an orifice or other restriction. In this case, the drop in temperature results from high-pressure Argon gas passing from the inner chamber to the outer chamber of a cryoprobe, allowing for precise tissue freezing and ablation at the tip of the cryoprobe.
The zone of cryoablation with any given probe extends a defined distance from the cryoprobe. As such, to ablate larger lesions, multiple cryoprobes are often required. 9 Contemporary technology allows the surgeon to simultaneously activate multiple probes, and even to activate multiple asynchronous sets of cryoablation probes to effectively treat larger tumors or multiple lesions simultaneously.
Our goals in the current study were threefold. First, we wished to confirm that the principle of the Joule–Thompson effect that a greater drop in pressure results in a greater drop in temperature can be realized in a gel model. Second, we wished to evaluate contemporary cryoablation technology regarding the ability to deliver consistent results under different conditions (simultaneous firing of multiple probes negatively impacts the function of each individual probe). Third, we wished to evaluate the ability to enhance the performance of the existing cryoablation mechanisms (beyond manufacturer recommendations) to see if future more effective iterations of cryoablation technology will be feasible (to demonstrate that a higher pressure differential [i.e., a higher starting pressure] results in a greater change in temperature in a tissue gel matrix).
Materials and Methods
All cryoablation trials were performed in a standardized system consisting of transparent gelatin (Kraft; Knox Gelatin, Glenview, IL) molds at 25°C. Gelatin was made by the addition of 28.8 g of dry powder to 1 L of boiling water. The mixture was poured into 10 transparent containers and cooled to room temperature and allowed time to solidify. On the surface of each container calibrated measuring markings were created using a standard ruler. About 1.47-mm cryoablation probes (IceRod; Galil Medical, Plymouth Meeting, PA) were inserted into the gel to a depth of 6 cm.
Two sets of trials were performed. The first trials evaluated temperature and ice ball size for a given tank pressure when a single needle was fired. The second recorded ice ball temperatures for each probe when multiple probes were fired simultaneously to determine if the pressure distribution diminished ice ball metrics.
Trial 1
A fixed template was used to precisely secure four single-sensor thermocouples at fixed distances (1.0, 1.5, 2.0, and 2.5 cm) from the cryoablation probe to give periodic temperature information throughout the experiment. The cryoprobe was activated for a single 8-minute freeze cycle, and was activated alone (no other probes attached to the system). A total of 13 pressures were tested with an initial tank starting pressure ranging from 4500 to 3200 psi (evaluated at 100 psi intervals). Each test was performed 10 times for a total of 130 ice balls. Time-lapse photography was used to document ice ball size at 1-minute intervals. Ice ball rate of formation and final ice ball size were documented for each group. The size of the ice ball was precisely measured using standardized measurement techniques. Temperature data for each thermocouple were documented at 3.4-second intervals for each trial. For statistical analysis, groups were stratified by low (3200–3500 psi), intermediate (3600–3900 psi), and high starting pressures (>4000 psi). Each group was compared for differences regarding rate of ice ball formation, final ice ball size, and change in temperature for each thermocouple using analysis of variance (ANOVA) technique.
Trial 2
Each cryoablation machine possesses five columns (a channel in which probes can be activated simultaneously), each with five ports to which cryoablation probes can be engaged (Fig. 1). We simultaneously engaged five probes in one channel to fill all the available slots (vertical probe positioning). The active cryoablation tip of each probe was inserted into one of five different containers as previously described. One thermocouple was deployed in each gel at a fixed distance of 1 cm from the cryoprobe. Next, we repeated a simultaneous five-probe evaluation with each probe attached to the first port site in each different channel (horizontal probe positioning), with the active ends again inserted each into one different gel container as previously described. Both vertical and horizontal multiport trials were performed a total of 10 times. All of these trials were performed with an initial tank pressure of 3200 psi to allow for completion of the experiment with a single gas tank (increased pressure exhausted the gas supply before completion of the trial). Temperature data for the thermocouple was documented at 3.4-second intervals for each freezing cycle. Interprobe temperature differences within the vertical and horizontal port placement groups were assessed using ANOVA techniques. Additionally, probe temperature change dynamics were compared with the single probe findings from trial 1 for the 3200 psi group using ANOVA techniques.

Rear panel of cryoablation machine. Five vertical channels, each with five ports, can be seen.
Results
Trial 1
The low-, intermediate-, and high-pressure systems reached a mean minimum temperature of −2.52°C (standard deviation [SD] = 2.85), −8.17°C (SD = 2.27), and −9.57°C (SD = 1.94) (p < 0.001), respectively, at the 1.0-cm thermocouple (Table 1). The mean rate of temperature change was −0.19°C, −0.21°C, and −0.24°C/3 seconds for the low, intermediate, and high starting pressure systems, respectively (p < 0.001) (Fig. 2). The mean maximum ice ball diameter was smaller (27.8 mm) for the low-pressure group than for the intermediate- (30.8 mm) and high-pressure (31.3 mm) groups (p < 0.0009) (Fig. 3). Mean growth rates were 3.2, 3.6, and 3.6 mm/minute, respectively (p = 0.26) for the low-, intermediate-, and high-pressure groups.
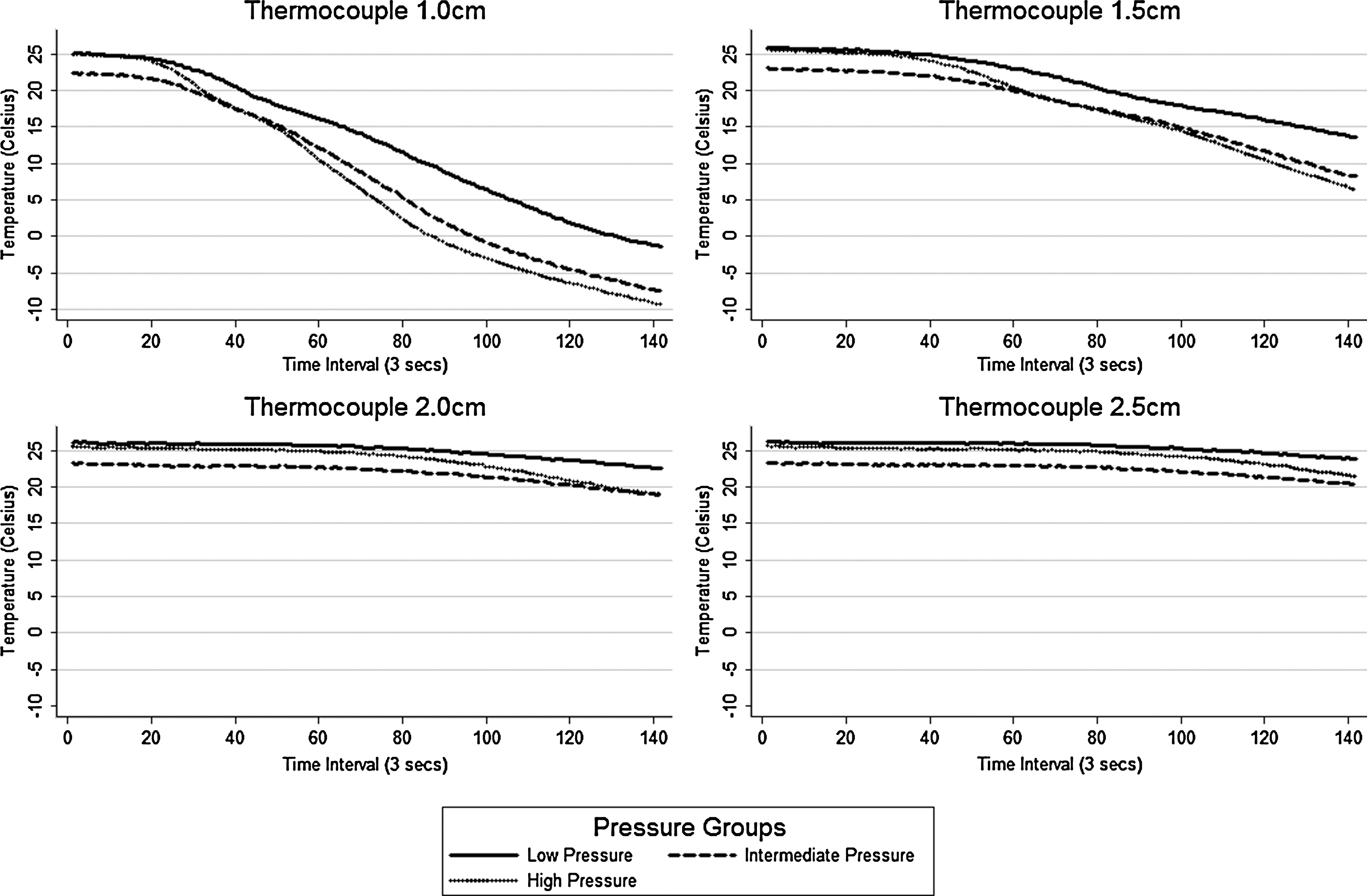
Mean temperature over time. A more rapid drop in temperature, and lower final temperatures were achieved at the thermocouple closest to the cryoprobe. At 1.0 cm the high-pressure group had a greater rate of temperature drop than the intermediate or low-pressure groups (p < 0.001).

Time-lapse photographs of ice ball formation over time at 1-minute intervals for the low-, intermediate-, and high-pressure groups.
Higher initial tank pressures resulted in lower final temperatures. As distance from the cryoprobe increased, so did temperature; the lowest temperatures were demonstrated at the thermocouple 1 cm from the cryoprobe.
Trial 2
Cryoprobes attached in the vertical probe position had an initial gel temperature range of 18.1°C to 19.7°C (mean 18.1°C; p = 0.62), final gel temperature range of −1.85°C to 1.0°C (mean −0.11°C; p = 0.74), and a mean change in temperature range of −0.12°C/3 seconds to −0.15°C/3 seconds (mean −0.13°C/3 seconds; p = 0.93). Cryoprobes attached in the horizontal probe position had an initial gel temperature range of 18.1°C to 19.7°C (mean 19.1°C; p = 0.07), final gel temperature range of −0.33°C to 1.17°C (mean 0.53°C; p = 0.93), and a mean change in temperature range of −0.12°C/3 seconds to −0.13°C/3 seconds (mean −0.13°C/3 seconds; p = 0.70).
When we compared the 3200-psi-group single probe firing from trial 1 to the multiple simultaneous firing groups in both the horizontal and vertical positions from trial 2, the final temperatures were not significantly different between the single (mean 0.48°C), horizontal (mean 0.31°C), and vertical (mean 0.56°C) groups (p = 0.96). The average change in temperature for the 3200 single firing was −0.19°C/3 seconds, which was not statistically significantly different from the average rate of temperature change of −0.13°C/3 seconds in the multiple probe firing groups (p = 0.7149).
Discussion
In this study we performed a practical evaluation of the Joule–Thompson effect (that a greater drop in pressure results in a greater drop in temperature can be realized in a tissue model), and we tested the ability of contemporary cryoablation technology to deliver consistent results. In addition, we evaluated cryoablation performance beyond of contemporary technology beyond the current manufacturer's recommendations (higher initial starting pressures).
As anticipated, the current data confirm that in a gelatin/cryoprobe model, the rate of temperature change is directly related to the initial pressure of the gas being released, consistent with the Joule–Thomson effect initially described in nonideal gases. Additionally, we found that the group with the highest starting pressures reached the lowest mean temperature and had the largest mean ice ball size. In clinical practice it is critically important to use the cryoablation device and probes within the ranges suggested by the manufacturer. Currently, with the system tested, only 3500 psi is acceptable. However, as future technology, manufacturing, and materials improve, it is clear that even without modification to the contemporary design, increased ablative efficacy is feasible.
Higher initial tank pressures were associated with faster freezing rates in this study. Previous work on cryoablation demonstrated that very fast freezing rates are associated with intracellular ice formation, which is a significant threat to cell viability and is almost always lethal to the cell. 10 –15 Our results would suggest the possibility for greater cell death in future technologies that utilized a system with larger pressure gradients. This conclusion, while alluring, was not evaluated in the current in vitro study, and hence its clinical applicability is unproven.
Ice ball size and the temperature gradients surrounding the cryoprobe are important factors, as the minimum temperature reached and rate of temperature change are related to cell death. 16 Higher initial tank pressures in our study were associated with a significantly increased ice ball size, with a mean ice ball diameter of 30.8 mm in the intermediate group and 31.3 mm in the high-pressure group compared with the 27.8 mm in the low-pressure group. The size of the ice ball was consistent with the temperature gradients evaluated by thermocouples at multiple distances from the cryoprobe, which revealed that the temperature was 0°C within 1 to 1.5 cm of the cryoprobe, equivalent to a diameter of 20 to 30 mm. These results are consistent with clinical findings by Ames et al 17 who used intraoperative ultrasonographic images to measure ice ball formation. They found that the ice ball surrounding a single cryoprobe was a mean 2.2 cm in diameter and correlated with a pathologic area of complete coagulative necrosis of 1.9 cm in diameter.
Weld and colleagues 9 described the tissue surrounding the area of complete coagulative necrosis, called the indeterminate zone, to consist of organized chronic inflammatory cells (predominantly lymphocytes and plasma cells), fibrosis, foreign body giant cell reactions, dystrophic calcifications, and a few scattered viable renal tubules. The average cross-sectional width of the indeterminate zone was 3 mm, but only 1.5 mm distally from tip of the cryoprobe. Whether a higher initial tank pressures and the resultant faster rate of temperature change and larger ice ball will affect the size of the indeterminate zone is unknown.
Multiple cryoprobes were fired simultaneously to evaluate if multichannel ablation diminished individual cryoablation probe efficacy on a practical level. Multiple probe ablation did not affect the rate of temperature change or final temperature compared with firing a single probe. Cryoprobe port site from the cryoablation machine did not affect performance either. Irrespective of probe port location or number of ports used, consistently reproducible results were obtained. These findings confirm that multiprobe ablations can be planned with the same confidence in freezing performance as single-probe ablations, which may be necessary to ablate larger areas than could be completely ablated by a single probe. 9
There are several limitations to this study. One is that we only used a gel-matrix model to test cryoprobe freezing dynamics; another is that we only used one type of cryoprobe. Although these factors may limit the generalizability of these findings to in vivo techniques or other cryoprobes, we chose this narrow scope of our study to focus on validation of the Joule–Thompson principle. Young and colleagues 18 recently compared different cryoprobes and tissue models demonstrating that agarose gel isotherms do not correlate well with porcine in vivo ablation zones (R.V. Clayman, pers. comm., 2009). Future work in in vivo models using higher pressure differentials will be required to precisely characterize the effect of these variables on ablation volumes and extent of necrosis. However, the data presented in the current article will likely reflect trends in ablative capacity.
The clinical relevance of the current study is twofold. First, these data emphasize the importance of maintaining proper Argon tank pressure during clinical cryoablation procedures. The low-pressure evaluation was consistent with the manufacturer's current guidelines for usage of the probes. The current suggested usage pressure is application of a 3500 psi tank pressure for safety and efficacy with the Galil Medical cryoablation system that we tested. This pressure provides optimal results when taking various parameters into consideration, including kill zone, ice ball size, and the rate of Argon gas consumption. A spokesman for Galil Medical noted that the kill zone may not correlate with ice ball size as consistently if different pressures are used (O Vaisman, pers. comm., 2008). Second and more importantly, we have clearly demonstrated that there is potential for improvement of contemporary technology by increasing the pressure gradient used for the cryoablation process. This information may help in the development of next-generation cryoablation probes that may be smaller and more effective in ablating larger volumes of tissue. Although improved ablation is intriguing, it is imperative that all clinical applications of ablation systems be in accordance with manufacturer's specifications.
Conclusions
In accordance with the Joule–Thomson effect, higher initial gas pressures used for cryoablation in a transparent gel model demonstrate statistically significant lower temperatures, faster decreases in temperature, and formation of larger ice balls than lower gas pressures do. Multiple simultaneous cryoprobe deployment does not compromise individual probe efficacy. The use of higher initial tank pressures will theoretically help future cryoprobes be more effective, creating a greater volume of cell necrosis and a smaller indeterminate zone.
Footnotes
Disclosure Statement
Jaime Landman—consultant for Galil Medical. No competing financial interests exist for the other authors.