
Abstract
Purpose:
To characterize the appearance of normal and malignant upper urinary tract lesion appearance under narrow-band imaging (NBI) using the new URF-V digital flexible ureteroscope (DFU), and to determine if NBI, when used in conjunction with white light (WL), could improve detection of malignancy.
Patients and Methods:
NBI and WL were performed in 27 patients at our university teaching hospital, 14 with known cases of upper urinary tract transitional-cell carcinoma (UUT-TCC) as follow-up (group A), and 13 patients with first-suspicion of cancer (group B). Full renal collecting system examination was performed first under WL and then under NBI by a single urologist. Biopsies were taken from all detected lesions using the biopsy forceps and sent for examination by a pathologist who was blinded to the gross description of the lesion. Pathology interpretations were then compared with the corresponding WL and NBI images. Holmium laser vaporization was performed for all apparent lesions.
Results:
Subjectively, NBI significantly improved the endoscopic visualization of the tumors, providing a detailed description of their limits and vascular architecture. Objectively, five additional tumors (14.2%) in four patients, as well the extended limits of three tumors (8.5%) in three patients were detected by NBI when findings by WL imaging were considered normal.
Conclusion
: This is one of the first reports regarding NBI for UUT-TCC. From this study, we recommend this technology as a valuable diagnostic method, because it considerably improves tumor detection rate by 22.7% compared with WL.
Introduction
White light (WL) images are, unfortunately, little reliable while aiming to diagnose the presence and the limits of urothelial tumors. Narrow-band imaging (NBI) is a new, alternative light-wavelength capture system that takes advantage of altered blood vessel morphology of urothelial mucosa. NBI opens a promising technique to enable us to make an accurate observation of small tumors, as well as establish their exact limits, closely related to their vascularization. These advances in tumor detection may have a substantial influence on conservative management of UUT-TCC, helping the urologist to perform a more complete vaporization of the small lesions that are not clearly visible with WL.
The aim of this study was to determine if NBI could improve detection of UUT-TCC compared with WL alone.
Patients and Methods
Between June 2008 and January 2009, NBI and WL, using the new URF-V Olympus digital flexible ureteroscope (Olympus Surgical, Orangeburg, NY), were performed in 27 patients—20 men and 7 women—with a mean age of 61 years (range 37 to 83 y). This study was performed after obtaining informed consent from all patients in a routine clinical practice. Fourteen patients (group A) were diagnosed previously and treated conservatively for UUT-TCC, and underwent NBI as part of their follow-up; on the other hand, studies of 13 patients (group B) were conducted in this practice to establish the diagnosis.
A standard protocol that included general clinical examination, blood tests, urinalysis, urine cytology, abdominal ultrasonography, intravenous urography, and CT was applied for newly diagnosed cases. The selection criteria for newly diagnosed patients were presence of hematuria, positive cytology, as well as suspected UUT lesions on radiologic images.
Endoscopic technique
The first stage consisted of careful full examination of the renal collecting system using the URF-V DFU in WL mode, resulting in a map of the suspicious lesions, followed by NBI, which described a specific map of all distinctive lesions. The repeated switching between WL and NBI provided the possibility to compare tumor visualization and its borders (Fig. 1) and to determine a tumor that is not visible by WL (Figs. 2 and 3). An abnormal appearance under NBI mode was defined as any area discordant in appearance vs WL appearance by either blood vessel concentration or appearance (ie, dotted, tortuous, or large-caliber, abrupt-ending vessels). Biopsies were taken (by Piranha biopsy forceps) from all the detected lesions that were visible by WL and even those lesions only visible by NBI, and then sent to be interpreted by a dedicated pathologist (MS) who was blinded to all clinical information except the anatomic location of the specimen. Holmium laser vaporization was performed for all visible lesions by WL and those lesions visible only by NBI mode. NBI control of the lesion margins was performed regularly after WL laser vaporization (Fig. 4).
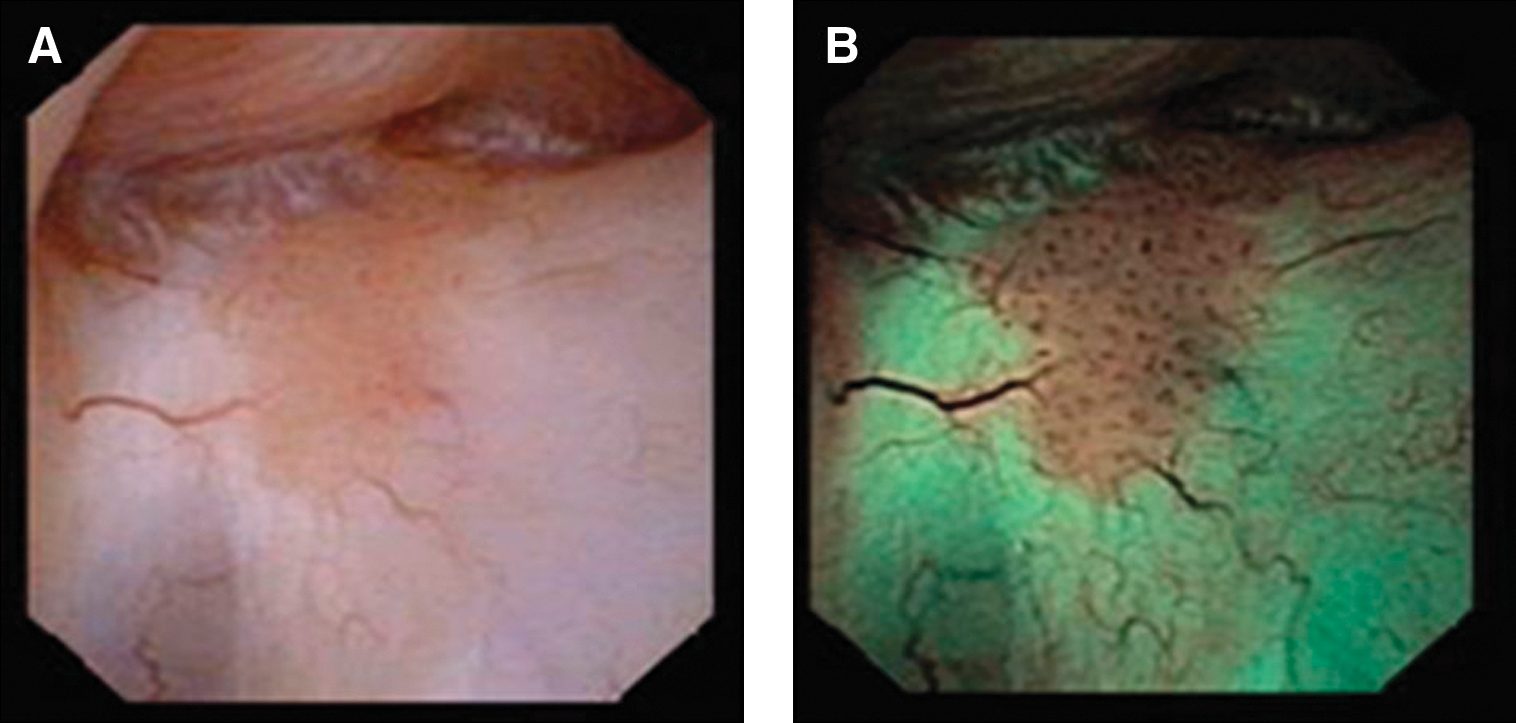
Urothelial tumor clearly visible with extended limits by


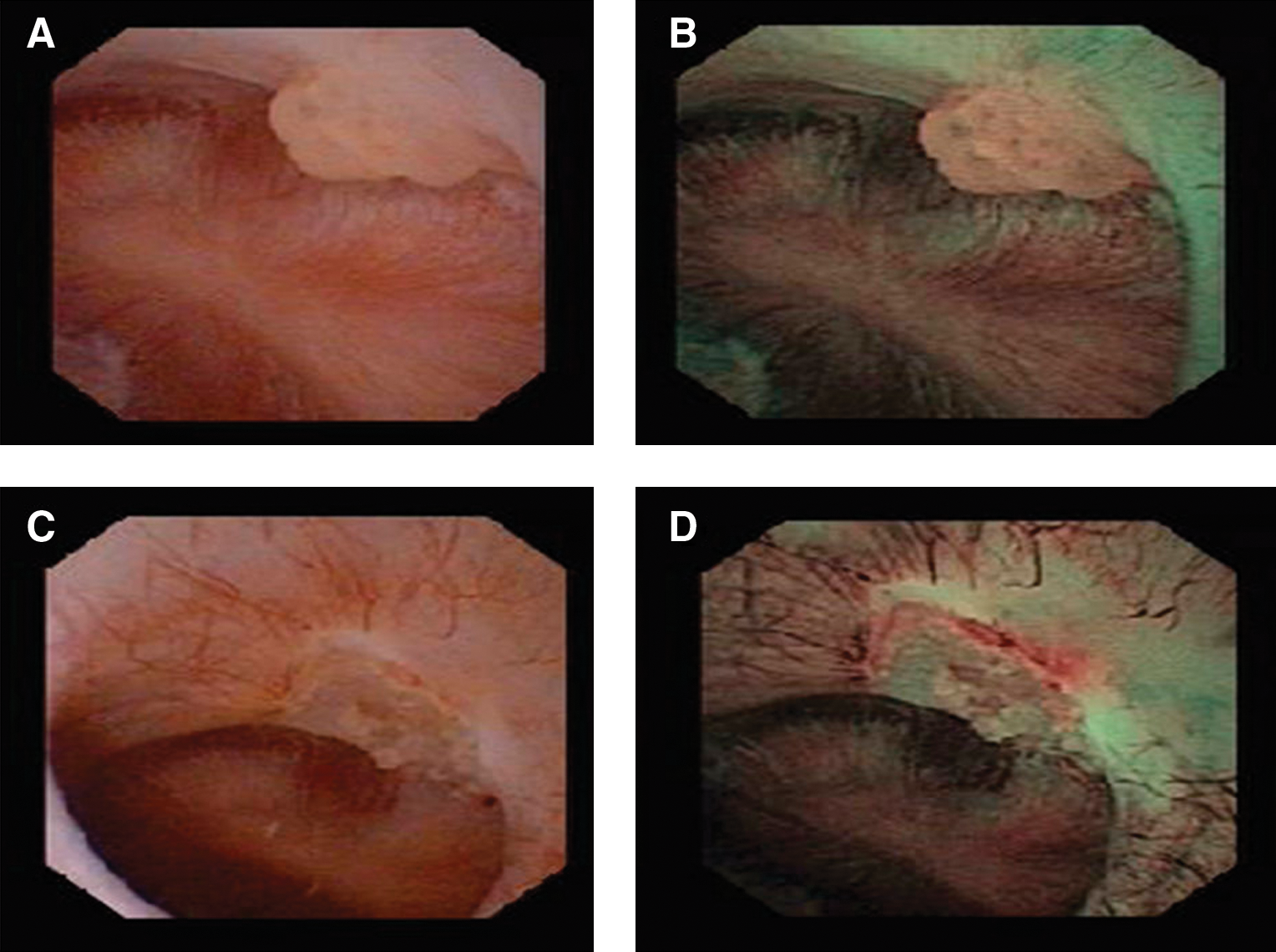
Tumor appearance before laser vaporization by
Results
Indications for procedures in this study were: UUT-TCC (51.8%), radiologic abnormality of the upper urinary tract (33.4%), hematuria (14.8%). Biopsy results are not always valid, because they are too small to confirm a pathologic outcome in 26%.
NBI compared with WL
In group A:
∘
∘
In group B:
∘
∘
NBI technology allowed us to diagnose and visualize clearly UUT-TCC and to identify tumor extended limits. In 5 of 13 patients with newly diagnosed UUT-TCC (38.4%), NBI provided additional diagnostic information. In these cases, the indications for conservative therapy were represented by moderate renal failures, single functioning kidney, and small single tumors.
In two (7.4%) patients, a complete inspection of the pyelocaliceal system proved to be impossible, because of the inaccessible lower calices.
There were 35 detected pathology confirmed transitional-cell tumors; NBI exclusively diagnosed 5 additional tumors (14.2%), and identified extended limits for another 3 tumors (8.5%). Therefore, tumor detection rate improves (22.7%) by using the NBI method (Table 1).
ABN = abnormal; NV = not valid; NL = normal; ABN* = abnormal with extended margin.
Discussion
NBI brings a new perspective to the currently developing field of diagnostic flexible ureteroscopy. The digital image is consistently more accurate and descriptive by comparison with standard one; moreover, the NBI mode enables us to identify in detail the vascularization of tumors. Specifically, optical image enhancement technology increases the visibility of capillaries and other delicate tissue surface structures by enhancing the contrast between them. NBI technology filters WL into two narrow-bands (415 and 540 nm), strongly absorbed by hemoglobin, thus penetrating the tissue surface and increasing the visibility of surface capillaries (shown in brown) and blood vessels (veins displayed in cyan) in the submucosa. Because of the vascular nature of urothelial carcinoma, NBI enhances the contrast between superficial tumors and normal mucosa. 1 –3
Subjectively, NBI clearly shows specific vascular architecture of UUT-TCC, creates the impression of a three-dimensional visualization of the tumors, and clearly defines the limits. The spatial representation of tumors, based on their vascular structure, improves the diagnostic accuracy of the method. Bryan and coworkers 1 reported this technology concerning bladder urothelial carcinoma, with a significantly increased detection rate. NBI cystoscopy improved the tumor detection rate of recurrent nonmuscle-invasive bladder tumors over standard cystoscopy.
One of the most important difficulties in UUT-TCC ureteroscopic diagnosis is represented by the reliability of pathologic specimens. In our study, none of the specimens included muscular fibers, so pTa stage (or noninvasive papillary urothelial carcinomas) can be considered doubtful. Various authors, however, considered that tumor grade may be just as predictive concerning the evolution and prognosis of the patients. 4
In our series, we identified four cases of high-grade UUT-TCC, which may have an indication for nephroureterectomy. Only 74% of our specimens provided a definite pathologic result. This result is comparable to the literature data; for example, Guarnizo and associates 5 performed 40 ureteroscopic multiple “cold-cup” biopsies and determined the correct pathologic diagnosis in 78% of the cases. Because of the small number of cases of UUT-TCC that were diagnosed among our series, percentages of patients can be considered as relevant. Nevertheless, that NBI provided additional diagnostic information is unmistakably significant in half of those patients with proven UUT-TCC.
There were no specimens taken from the extended margins of the tumors, which were visible only by NBI, so pathologic examination was unable to confirm this hypothesis. It is obvious, however, that NBI improves the chances for a complete laser vaporization of any lesion by showing extended tumor base vascularization. Therefore, we report that the little reliable WL visualization is not strongly considered concerning tumor-free status of the patient at the end of the procedure.
Difficult access because of some anatomic conditions, a perpetual problem when performing flexible ureterorenoscopy, was significantly reduced by good maneuverability of the URF-V. Complete exploration of the upper urinary tract was successfully achieved in various proportions in published studies: 66%, 6 78.3%, 7 82%, 8 90.5%, 9 95.7%. 10 Our series correlates with these results, describing 92.5% as a success rate in diagnostic flexible ureterorenoscopy. The limits are represented by difficult access to the lower calix. 11,12 In our series, it was easier to access the lower calix because of the 275-degree down-angulation.
To our knowledge, this is the first publication on NBI for UUT-TCC; however, this study has two certain limitations. First, we aimed to evaluate the concept of this work that NBI may, without a doubt, improve detection of urothelial tumors compared with WL, despite the fact that this is a new technology at the time of our assessment. Therefore, further study is the rational consequence to our primary results. The second limitation was the observer bias in overestimating abnormality and peculiarity of UUT lesions where no lesion may have existed.
Conclusions
NBI seems to represent a valuable diagnostic technology for UUT-TCC, showing considerable improvement of tumor visual accuracy as well as tumor detection rate. It also enables the urologist to determine the exact limits of tumors, thereby facilitating complete laser vaporization. Further studies are needed to clarify the impact of this technology on the diagnosis, recurrence rate, tumor-free survival period, and overall evolution of those patients. Future directions include combining NBI with molecular markers in those at high risk for UUT-TCC.
Footnotes
Disclosure Statement
No competing financial interests exist.