
Abstract
Laparoscopic surgical procedures are becoming common across surgical specialties, including urology. Maintaining a clear field of vision is paramount in such procedures not only for safety by preventing inadvertent injury, but also to improve precision and reduce operative time. Laparoscopic lens fogging (LLF) is a major impediment to a clear visual field during laparoscopy and is caused by condensation as well as particulate debris, blood, and smoke accumulation on the scope lens. Despite many available techniques to improve vision during laparoscopy, available data on etiology and methods to improve vision have only sporadically been considered in the literature. The objective of this review was to summarize current literature on the etiology of LLF and other causes of poor vision during laparoscopy and also review the current approaches for minimizing or reducing such events. In summary, although the etiology of LLF is well understood, that is, temperature and humidity differences, the methods to reduce its occurrence lack significant data. Of those methods that are often espoused, most are not supported in the literature, such as warmed and humidified insufflation gas, or simply lack data, such as antifogging solutions.
Introduction
Methodology
A literature search using various bibliographic tools available through our library service was performed. All publications were identified through PubMed, Embase, and Google Scholar for all English-only journals published during the period between 1970 and October 2009. The search strategies employed a number of free-text keywords as well as controlled vocabulary terms, including (but not limited to) the following concepts: LLF, laparoscopy, methods, equipment failure, equipment designs, vision, temperature, and humidity. We also conducted further searches of article bibliographies to ensure that no studies were missed. Any article encountered, whether review, original research, or case report, was permissible.
Implications of LLF and Other Causes of Reduced Vision
The implications of a poor visual field during laparoscopy may seem obvious but should not be discounted. A World Health Organization 6 report identified that problems with the lens of the laparoscope may contribute to surgical errors such as using a device incorrectly or placing instruments on structures other than those intended. Although this is not the likely outcome, LLF often leads to an increased operative time, suboptimal view when the vision is impaired and thus slowing procedural progress with the potential for adverse events, as well as the irritation due to repeated disruptions of having to remove the laparoscope to resolve the situation. Further, vision is likely to be impaired in situations where paradoxically the best vision is required: close-up viewing (where LLF is more likely to occur), accidental bleeding (with blood on the lens), diathermy to control bleeding (with increased smoke), and sudden pneumoperitoneal decompression (particulate debris, e.g., fat, blood, eschar). 4,5 It must also be stressed that minimal or no (in the case of robot assisted) haptic feedback in laparoscopy 7 ensures that vision and visual cues become extremely important.
The Etiology of LLF
From examining the literature, initially it appears that the etiology of LLF has been taken as given, with most accepted theories stating that LLF occurs when there is an imbalance between the temperature of the front lens of the laparoscope and the temperature of the abdominal cavity. 8 –10 This temperature difference results in condensation on the front of the lens and thus fogging of vision. In addition, a pneumoperitoneum has usually more than 85% humidity, which is much higher than the surrounding atmosphere in the operating room. 9 Likewise, the operating room temperature, typically 21°C to 24°C, is usually significantly lower than the intraperitoneal space. 11 Schurr et al 9 also concluded without data that the most important precondition for maintaining a clear visual field is continuous maintenance of the temperature of the front lens at 37°C.
However, if one examines the literature more closely (Table 1), the seminal works of the Australian-German minimally invasive surgery group in 1996 are the one that has really given us the understanding of LLF and the principles to help reduce its occurrence. 5,12 The physiology is basically what has been stated by others and is likely derived from their studies, but it is more complex. The Australian-German group performed some extremely valuable experiments in a porcine and then an in vitro model to help us understand why LLF occurs in laparoscopy. In essence, they investigated the environmental conditions within an insufflated abdomen and then determined the quality of vision under these conditions. 12
LLF = laparoscopic lens fogging; RCT = randomized controlled trial.
The Australian-German group established in the porcine model that the temperature of the insufflated gas equilibrates quickly with body temperature and remains close to 37.5°C. Interestingly, at maximum insufflation of 15 L/minute the temperature remained unchanged. Further, the humidity was around 85% despite the insufflation gas having 0% humidity prior to entry into the insufflation cavity. This supported another work in a canine model. 13 The in vitro model then explored relationships further in a controlled environment. Thus the key to understanding the mechanisms of LLF lies with the graphical representation they described, which pinpointed the relationship between vision, humidity, and temperature (Fig. 1). 12
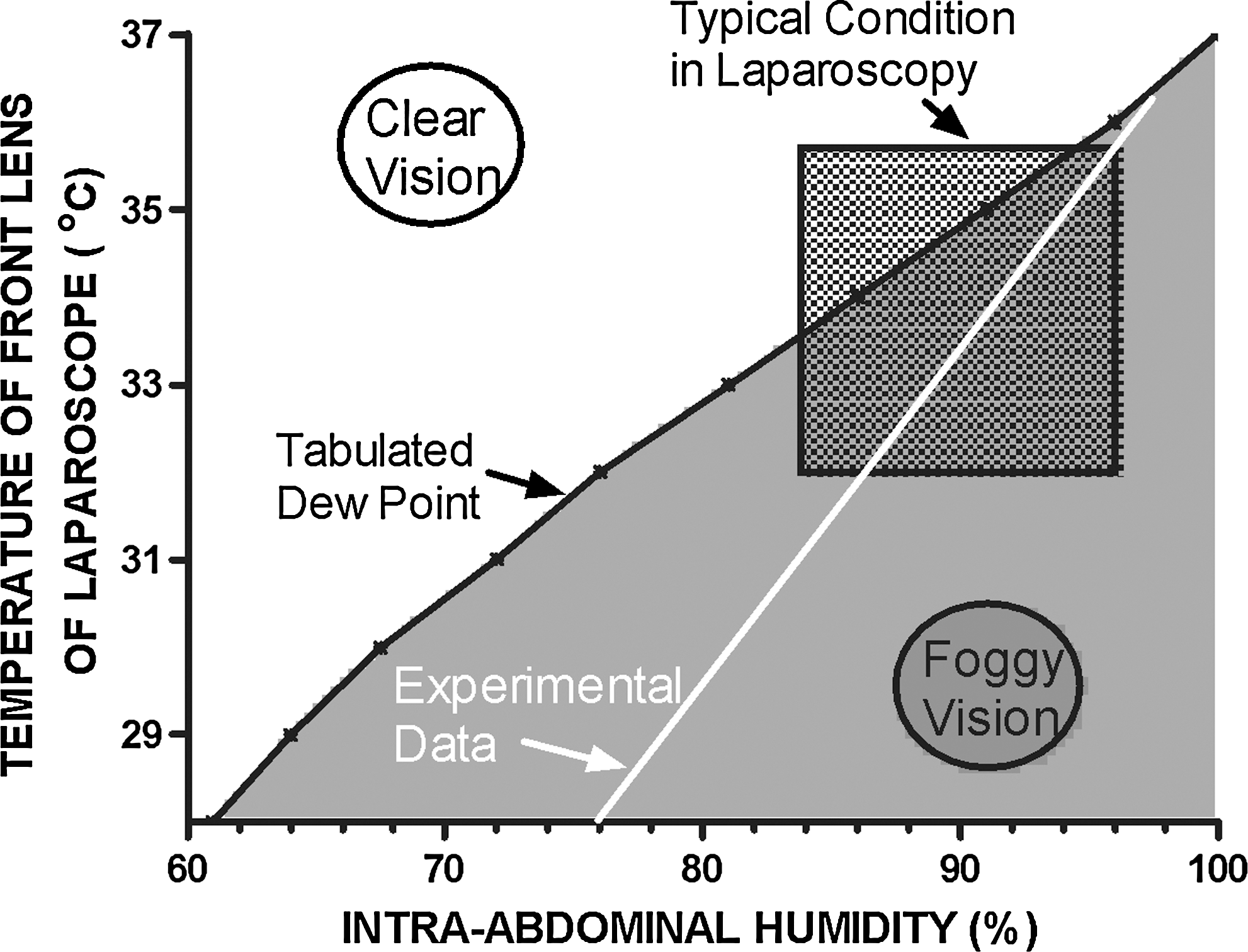
Graphical representation of the physical conditions that determine optical clarity during laparoscopic surgery (adapted from Flemming et al 12 ). For detailed description, please refer to the text.
In Figure 1, the horizontal axis represents the relative intra-abdominal humidity and the vertical axis is the temperature in front of the lens optic. You will note that both of these axes terminate at maximal physiologic values, 100% humidity and a temperature of 37°C. The upper diagonal of the graph is “clear vision” and the lower diagonal is “foggy vision,” both separated by the tabulated dew-point derived from scientific tables, which is the point when condensation should theoretically occur on the lens of the laparoscope. Dew-point thus represents the temperature at a given humidity and the temperature of the surrounding gas at which condensation occurs on a surface. The white line to the right of the expected tabulated data represents their experimental data. 12 The difference between the theoretical value and what they observed experimentally is likely due to vision being hindered when larger droplets accumulate and the optical wavelength (400 nm) exceeds. The outlined square on the graph represents typical conditions in laparoscopy, and in reality, using the experimental data, there is a potential for the scope to have condensation on the lens approximately half of the time if the humidity is raised or the temperature falls in the correct sequence. In other words, the scope temperature must be above 34°C for a humidity of around 85% (typically lower end of normal laparoscopy) to maintain vision. Another point is that if the scope lens is at a temperature above 37°C then condensation does not occur despite 100% humidity. 12 This led the Australian-German group to suggest that a complete optic should maintain the scope lens at above 37°C to be efficient at preventing LLF. 5
Flemming et al 12 also found that the lens temperature of the laparoscope varied with insufflation rate, insertion length, and length of the trocar, as well as the type and intensity of the light source and laparoscope model. All of these should be considered in any laparoscopic case, but not all are likely to affect each case. Of course, the theory of temperature and humidity supported by experiments of the Australian-German group appears sound. Most surgeons as they highlight 12 have experienced LLF, taking the laparoscope out for extracorporal cleaning of the lens in cold water or saline, only to find that the scope has cooled, leading to recondensation at reentry. The number of manuscripts spanning four decades cited in this review is also testament to the common nature of LLF and the realization it has not been resolved.
Finally, one must consider other physiological factors such as the length of surgery and impact on body temperature, which will in turn eventually affect the intraperitoneal temperature. It has been found that a decrease of 0.3°C in the core temperature was observed for each 50 L of CO2 insufflated. 14 Although the drop in temperature is small, a procedure lasting many hours will have an impact on body temperature but it is unlikely to manifest in changes in the incidence of LLF because of its small degree 15 and with compensation by the use of warming blankets on patients. The physiologic effects of insufflation temperature have been measured in many studies, 15 –17 such as the impact on body temperature, immunology, and postoperative pain, but these are not the subject of this review.
Principles to Assist Clear Vision During Laparoscopy
A list of principles to assist clear vision during laparoscopy were developed by the Australian-German minimally invasive surgery group in 1996. 5 They suggested the following principles: the laparoscopic front optical lens should be warmed to ≥37°C, presence of a facility to rinse and dry the front lens of laparoscope, a constant flow of insufflation gas, and presence of a facility to exsufflate smoke ± “burst” evacuation during electrocautery.
Some principles they raised have been challenged, all relating to the proposal that the insufflation gas should be warmed to 37°C to 45°C and humidified to 50% to 80%. Neither was found to be a factor in reducing LLF in a meta-analysis that included seven trials. 18 Of note, a large prospective randomized trial also had this conclusion. 19 Despite these findings, the American Urological Association (AUA) guidelines on laparoscopy 20 still appear to support warmed and humidified insufflation gas, based on a single nonrandomized pilot trial. 21
The group also recommended connecting the insufflation gas through the same port as the laparoscope to assist in reducing LLF because of their belief that humidity and temperature assist in reducing LLF. 5 If we accept that the insufflation gas temperature and humidity do not matter, then this point equally may not matter. However, it remains controversial 5,12 that connecting insufflation to an alternate trocar may actually reduce LLF, but it is certainly practiced by many surgeons.
Building on the aforementioned principles to help maintain vision, specific methods to reduce LLF may be divided into four broad categories (Table 2): Mechanisms to warm the laparoscope Antifogging solutions Equipment modifications to laparoscope Miscellaneous methods
Mechanisms to warm the laparoscope arose likely because of common sense but were certainly supported physiologically by the work of the Australian-German group. 5,12 The methods in Table 2 from a warmed thermos flask, to warming baths and scope warmers, even a recently developed disposable electric scope warming device (e.g., Matrix Medical, Melbourne, Australia), all appear sound but lack data. Hashimoto and Shouji 22 at least created a simulation model for their in-built scope warming device demonstrating efficacy. So we cannot answer the simple question of whether 1000 mL of warmed physiologic saline 23 is any better or worse than using an expensive thermos flask. 10 What is intuitive and supported is that a method of warming the scope appears a sensible step in any laparoscopic procedure. This should be undertaken prior to commencing, when LLF occurs, and at the time of cleaning or changing scopes.
Commercial antifogging solutions and readily available operating room liquids such as povidone–iodine solution (e.g., betadine) 24,25 have been used to prevent LLF. Of the commercial agents, Fog Reduction and Elimination Device or FRED™ (Covidien Autosuture, Mansfield, MA) 26 –28 is the most mentioned in the literature. It consists of less than 15% isopropyl alcohol, 2% surfactant, and more than 85% water as a liquid with a disposable sterile foam pad to help clean and disperse the product on the lens during procedures. 29 Europe Reso-clear™ (Resorba Wundversorgung, Nürnberg, Germany) is popular and follows similar concepts, but it is an impregnated sterile moist wipe. The mechanism of action in both instances is to cause the droplets of condensed steam to spread themselves rapidly over the surface of the cold lens thus clearing the vision. Most require cleaning of the scope prior to application and surgeons generally warm laparoscopes in conjunction with such methods. Dispersion methods such as applying the antifog via an insufflator or in a syringe are of interest but require more data. 28,30 Easily available liquids such as povidone–iodine act in a similar manner and are substantially cheaper (at least 10 × ) than commercial agents. No head-to-head or single-arm studies could be found in the literature to support and ascertain the efficacy of either group, and so their use is based purely on experience and expert opinion. Betadine solutions are typically aqueous solutions of 10% povidone–iodine and there are no studies comparing different concentrations or warmed versus room temperature, which all may potentially affect the efficacy. Finally, it had been stated in the past that robotic equipment could not have commercial antifogging solutions used with them, but this is now no longer the case (personal communication) and an article in this review using an agent with robotics is testament to this change. 28
Equipment modifications have resulted in new types of laparoscopy lenses from superhydrophilic, titanium dioxide-coated glass. Incorporating scope warming within the scope assists with the temperature, which as discussed is advantageous. The incorporation of irrigating channels is said to assist as is the newly developed vibration mechanism that physically cleans the lens surface. 31 Of these technical changes to laparoscopes, only the Japanese group 31,32 has studied them in detail. Laparoscopes with self-cleaning mechanisms appear not to become commercialized due to cost and practicality where additional size and potential for problems with operation or sterilization are a disadvantage.
Finally, for miscellaneous methods the one most commonly employed is wiping the camera on the viscera (e.g., liver or bowel) to clean the lens. 25,26,33,34 This method may cause protein to build up on the lens, hampering vision, and it can potentially damage the viscera. 25 Reported studies have found that the light source can be up to 750°C, 250°C at the end of the light lead and up to 100°C at the end of the scope. 34 They also discovered that cytological tissue damage occurred even after only 5 seconds of contact. In robot surgery where the laparoscope is warmer, the potential for injury with this maneuver is greater. 28 Finally, by wiping the lens on a visceral surface with unrecognized blood will cause the vision to deteriorate. 35 Of the other miscellaneous methods, ventilating gas is practiced, in which gas is connected to a port other than the camera trocar. 4,5,16 Following from ventilation, it is also a common practice to withdraw the laparoscope into the trocar for a brief period to allow the LLF to dissipate and smoke to be evacuated.
The Etiology of Other Causes of Poor Vision During Laparoscopy
The two major groups of poor vision other than LLF relate to the fluids and tissues passively encountered in the operative field (e.g., blood, fat, and ascites) and the reaction of tissue to accidental or intentional injury (e.g., smoke and eschar with thermal injury from diathermy, bleeding onto the lens). 4,5
Meticulous hemostasis should be accomplished because excessive blood in the operative field resulting in absorption of light and poor field is one of the causes of poor vision of operating field. 36 Oxidized cellulose (e.g., Surgicel®, Ethicon, Inc., West Somerville, NJ) or a gauze may be temporarily placed to stop bleeding so that the surgeon may focus on a different part of the procedure to return later for definitive treatment (resolved, suture, or fibrin glue, where appropriate).
Adequate use of retraction, culling of fat that is likely to soil the lens or be in the way of the operative field, is essential to improve vision. Also, common sense dictates that suction and irrigation are important tools to maintain a clear operative field and improve vision during laparoscopy. However, excessive use of either may in itself cause problems. Over irrigating may wash fresh clots away causing more bleeding and so judicious use of irrigation to wash a specific target such as a clot, fat, or debris is preferred. 35 Suction may also be used strategically in short burst to remove clot or fluids so as not to reduce the pneumoperitoneum, reducing vision and potentially encouraging venous bleeding, which is tamponaded by higher pressures. Smoke may be sucked out, but if again done too rapidly it will deflate the pneumoperitoneum in the same way as rapid decompression because leaking trocar causes the same result. 35 Smoke from diathermy and debris may be lessened from soiling the lens if the assistant or camera driver in the case of the robot is moved away from the tissue briefly at the time of energy application and then moved back. Regular ventilation of smoke will also assist in reducing poor vision. 4
Equipment issues such as poor focus, damaged cables, scopes, fiber optics, and software issues should also be considered when vision is impaired. 33 Moisture may build-up between the laparoscope and camera if these are separate pieces, and so both these components need to be disconnected carefully and cleaned with dry gauze. 24 Fogging of mask visors, spectacles, and protective eyewear have also been reported and need to be dealt with using antifog or better placement (e.g., closing of nosepiece on the operating mask). 37
Clear vision has also been improved with digital laparoscopes as well as more recent advances such as high-definition laparoscopy. 38 Infrared vision may be an adjunct but has yet to be commercialized. 39 Vision will be paramount with single-access port-type surgery in which removing instruments in and out is particularly burdensome. 31,40 Three-dimensional imaging is already in use in robot-assisted laparoscopic surgery, 41 but further advances such as optical sensors to let operator know the distance from anatomical structures are needed. 42
Conclusions
Reduced vision during laparoscopy due to LLF is a common problem. The physiology behind LLF is well understood based on meticulous experiments outlining the role of temperature and humidity. Although many methods to reduce LLF focus on temperature, they along with other methods have very little evidence-based literature to support their use. Methods to reduce LLF are few and far between. There are several anecdotal and descriptive papers on methods to prevent LLF. Certainly, we need more data to help overcome this common, frustrating, and potentially dangerous problem. We also believe that a realistic model of the operation process should be a starting point for every new design, 43 including testing methods to reduce LLF. Until then, surgeons need to understand LLF and perhaps look critically at all the methods, which are often expensive, to reduce LLF. Finally, other causes of poor vision need to be attended to and understood to further enhance the surgical performance during laparoscopy.
Footnotes
Disclosure Statement
No competing financial interests exist.