
Abstract
The purpose of this article is to review both routine T2-weighted and new MRI techniques in the imaging of prostate cancer (PCa) for focal therapy. T2-weighted imaging, knowledge of MRI prostate zonal anatomy, cancer morphology, and intraprostatic tumor spread remain essential for clinical PCa imaging; however, new techniques, such as dynamic contrast-enhanced MRI, diffusion-weighted imaging, and magnetic resonance spectroscopic imaging yield significant improvements in identification and volume estimation. Potential advantages of 3 Tesla MRI are adequate imaging without an endorectal coil. Future studies should work toward helping define standard, reproducible approaches to multimodality MRI and image reporting for research and clinical practice.
Introduction
Knowledge of MRI prostate zonal anatomy, cancer morphology, and intraprostatic patterns of spread of organ-confined PCa is essential for image interpretation and treatment planning decisions. 8,9 New MRI techniques, such as dynamic contrast-enhanced MRI (DCEMRI) and diffusion-weighted imaging (DWI), provide significant improvements to routine T2-weighted images (T2-WI) and will be reviewed.
MRI Anatomy
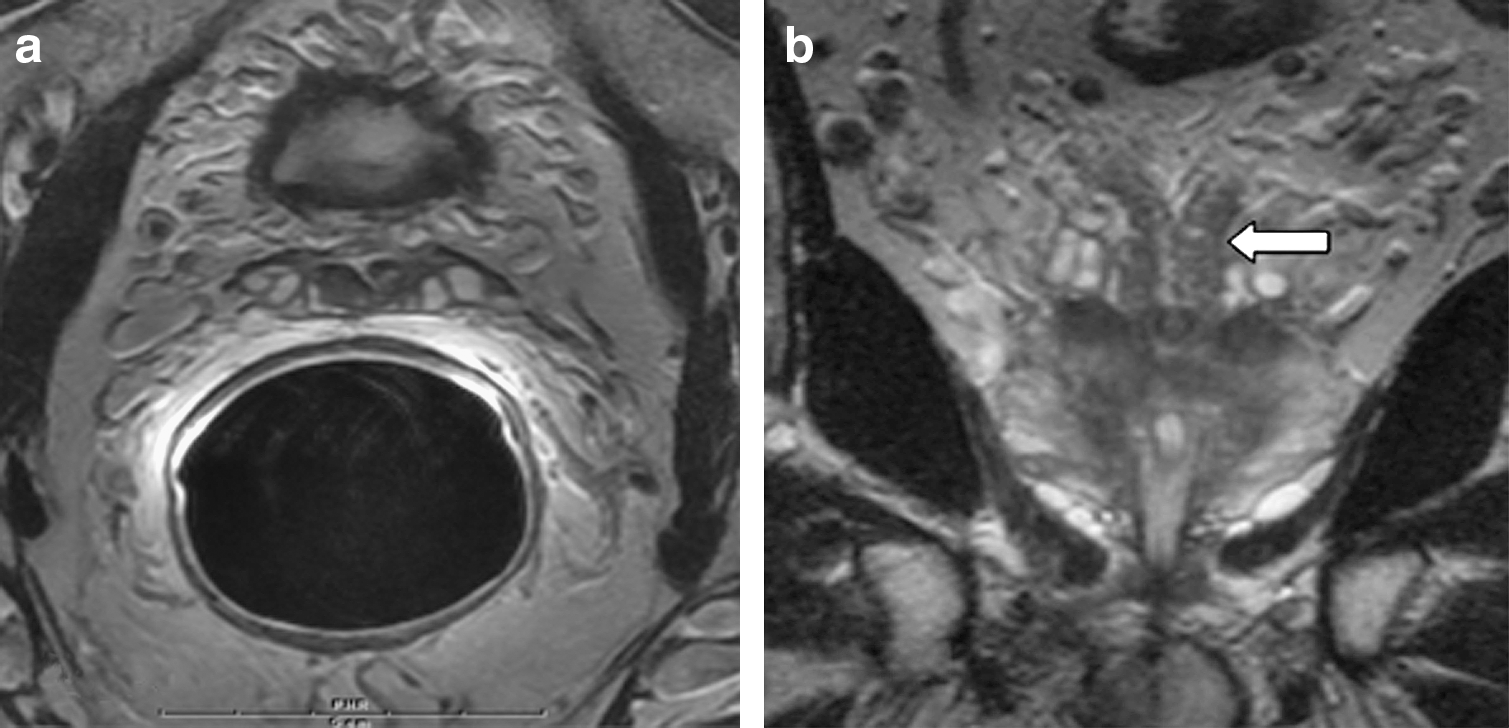
The pyramid shape of the prostate is seen well on coronal T2-WI (Fig. 1a), with the apex caudal and base cranial. The seminal vesicles at the base show lobulated high T2 signal intensity (Fig. 2a). A T2 low signal intensity area central in the seminal vesicles represents the vasa deferens (Fig. 3a, 3b), which continue through the prostate as ejaculatory ducts, fusing with the urethra at the verumontanum (Fig. 1b). Care should be taken not to misinterpret the T2 low signal medial in the seminal vesicles as seminal vesicle invasion by PCa.

Normal anatomy of the prostate using integrated endorectal-pelvic phased array coil at 1.5T. (

Normal anatomy of the prostate: Axial T2-weighted images through the prostate, with (
Normal anatomy of the prostate: (
The prostate can be divided into four zones: (1) the peripheral zone (PZ), (2) central zone (CZ), (3) transitional zone (TZ), and (4) anterior fibromuscular stroma (AFS). At the base, the prostate consists of all four zones (Fig. 2b), from dorsal to ventral; the PZ (bright T2), CZ (low T2), TZ (mixed T2 signal), and AFS (low T2). The CZ decreases in volume from base toward the verumontanum (Fig. 1b). On the coronal view the CZ has a characteristic triangular appearance (Fig. 1a), not to be mistaken for PCa. Anterior of the CZ at the base and anterior of the peripheral zone toward the apex lies the TZ, with mixed high and low T2 signal that embraces the prostatic urethra and extends from base to the verumontanum. The AFS is located anterior in the prostate (Fig. 2b) and demonstrates very low signal intensity. The AFS is not bordered by a prostate capsule and gradually blends with fat anterior of the prostate. Between the TZ and PZ, there is a visible capsule-like boundary—the surgical capsule, which is a pseudocapsule. The neurovascular bundles are located dorsolateral, between the rectum and dorsolateral prostate border.
Identification of PCa by Multimodality MRI
T2-WI
T2-WI are the most routine images generated by an MRI scanner. In general, images show pathology and depict water as a high signal (bright) and fat as a low signal (dark). The other basic sequences are T1-weighted images (T1-WI), where fat and proteinous material such as blood has a high signal (bright) and water a low signal (dark).
T2-WI provides high-resolution morphologic imaging of the gland and cross-referencing using three planes (Figs. 4a, 4b, 4c) and results in improved PCa imaging 10 (Fig. 5). Axial T1-WI is used to detect postbiopsy hemorrhage, which has a high signal intensity on T1-WI. The problem with using T2-WI alone is low specificity; for example, prostatitis, hormonal therapy, and benign prostatic hypertrophy (BPH) extending into the peripheral zone may look like PCa. PCa detection in the peripheral zone is easier than in the transition zone (Fig. 6), because of coexistence of BPH in the transition zone. Using the criterion of smooth low T2 signal, however, even using routine T2-WI, prostate cancer can be detected with a sensitivity of 76% and specificity of 87% 11 (Fig. 5). The main drawback of T2-WI is that readers need to be highly experienced to detect and stage PCa with high accuracy. 12
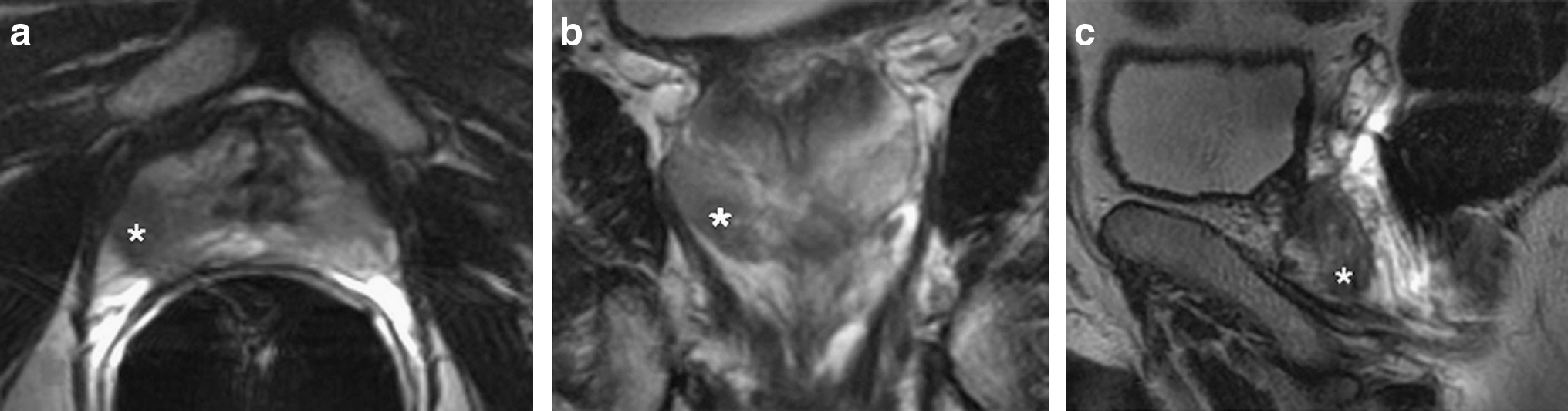
Prostate carcinoma, marked with the asterisk: Transverse (

T2-weighted transverse image of the prostate (

Anterior fibromuscular stroma cancer at multimodality MRI performed using a high resolution pelvic phased array coil at 1.5T, in a 66-year-old man with a prostate-specific antigen level of 13 ng/mL. (
DCEMRI and DWI
DCEMRI uses gadolinium intravenous contrast to demonstrate the enhancement of tissue in time. For example, cancer tissue may enhance differently compared with normal tissue; PCa enhances faster and shows more enhancement compared with normal tissue. After intravenous injection of gadolinium contrast, an image is scanned every few seconds, and in this manner, enhancement of the tissue of interest is demonstrated.
The combination of T2-WI sequences and DCEMRI using intravenous gadolinium chelate is considered to be the most sensitive sequence for identification and staging of organ-confined PZ or TZ cancers, either using endorectal-pelvic phased array coils (ER-PPA) 13 or high-resolution–pelvic phased array coils (HR-PPA). 14 –16 These coils can be understood as both receivers and antennas of the MRI signal. If the antenna/receiver is placed close to the organ of interest, the signal increases and the noise decreases, resulting in improved images. This is the reason the images using the ER coil show improved clarity compared with images without the ER coil. However, disadvantages of the ER coil include its cost, as it can be used only once, the occasional failure and possible inhomogeneous signal.
For localization of small PCa, additional subtraction for the dynamic imaging could be superior to both T2-WI and unsubtracted dynamic imaging. 17 For PCa both in the PZ and TZ, DCEMRI has been shown to have a higher gadolinium peak concentration compared with normal PZ and TZ tissue. 18 A problem in the TZ, as with normal T2-WI, is that BPH enhances in a manner similar to cancer tissue. One important and specific sign of PCa in the TZ is washout 18 (Fig. 6b).
As for the DCEMRI, DWI adds sensitivity without loss of specificity (Figs. 6 and 7). In DWI, the microscopic motion of water molecules can be seen. Focal changes in diffusion may signal alteration in tissue cellularity, permeability, or organization indicative of disease. Several studies have assessed its added value to T2-WI alone, with mean cancer detection sensitivity gains of 17% and 7% in PZ and TZ, respectively. 19 –25

Transition zone (TZ) cancer at multimodality MRI performed using a high-resolution pelvic phased array coil at 1.5T. Added value of diffusion-weighted imaging (DWI): a 69-year-old man with a prostate-specific antigen (PSA) level of 20 ng/mL with a free/total PSA ratio of 8%. He had a history of two negative transrectal ultrasonographic-G biopsy series in another facility with infectious complications each time. Digital rectal examination was normal. He was referred for a third series of biopsies. Prebiopsy MRI shows a typical TZ nodule of the anterior part of the midgland, which is concordant in all sequences of a multimodality MRI protocol (TZ cancer is shown at the white arrow): (
In a multireader study, the addition of an apparent diffusion coefficient (ADC) map to T2-WI improved the diagnostic performance of MRI in PCa detection. 26 The ADC map is a numerical representation of diffusion. ADC is significantly lower in malignant compared with nonmalignant prostate tissue, which increases the specificity of cancer detection. 27 There is a significant correlation between the ADC values and cell density (r = −0.50, P < 0.001), regardless of tissue type. 28 A recent study demonstrated that sparse cancers have ADC and T2 values similar to those of normal PZ tissue, suggesting that DWI may not, for the moment, substitute to DCEMRI in a multimodality MRI protocol. 29
A potential perspective of DWI is diffusion-tensor imaging, which measures diffusion coefficients in the three planes. 30,31 MR spectroscopy imaging (MRSI) allows assessment of tissue metabolism in a single or in multiple voxels. In PCa, there is reduced levels of citrate and elevated choline levels, compared with healthy prostate tissue. Technically, an ER coil is necessary for MRSI because of its high signal-to-noise ratio (SNR), but new HR-PPA at 3T may challenge ER coils. 32,33 Added value of this sequence for identification of confined PZ or TZ cancers and for treatment planning is proven, 34,35 but its use in daily clinical practice is still controversial. 36 In a meta-analysis, a limited number of small studies suggest that MRI combined with MRSI could be a rule-in test for low-risk patients, but further validation and cost-effectiveness of this indication still needs to be established. 37
Multimodality MRI
Puech and associates 38 concluded that multimodality MRI protocols can now assess the whole gland, including the challenging anterior part. Multimodality MRI is described as a combination of multiple complementary morphologic (T2-WI) and functional (DCEMRI, DWI, MRSI) sequences that generate consequently an important amount of data. This necessitates an integrated interpretation, and, according to some authors, new standardized reporting tools to increase reproducibility. 39 Studies showed the interest of combining T2+MRSI+DCEMRI, 40 T2+DWI+DCEMRI 8,24,41 (Figs. 6 and 7), T2+MRSI+DWI 2,25,42,43 (Fig. 8), and even T2+MRSI+DWI+DCEMRI. 39
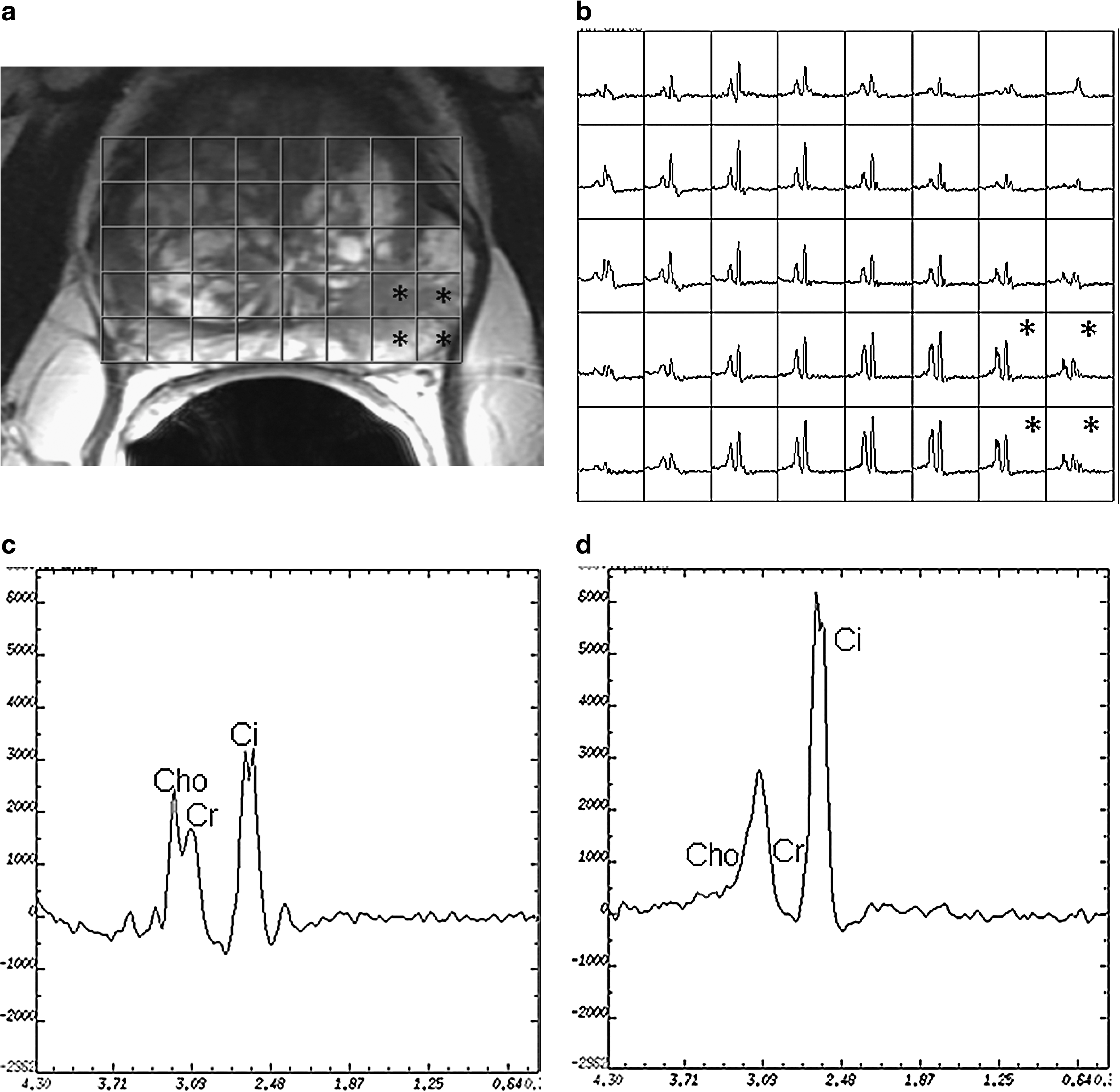
Magnetic resonance spectroscopic imaging of prostate carcinoma. Fusion of T2-weighted image (
3 Tesla
Tesla (T) refers to the magnetic field strength of the magnet. Most MRI scanners today are 1.5T. New MRI scanners have higher field strengths, such as 3T, which offers some advantages. Because of the higher field strength, the signals from the imaged object are higher, resulting in increased SNR ratio and thus clearer images. 3T MRI clearly improves spatiotemporal and spectral resolutions of prostate imaging on T2-WI sequences. Imaging criteria for malignancy, however, seem to be comparable at 3T and 1.5T, and added value of 3T MRI for cancer identification has to be measured in large series using full imaging protocols.
These advances were reviewed with an emphasis on imaging sequences; for example, T2-WI, DCE, DWI, and MRSI. 44 Because it is not readily available in most centers, 3T imaging may be at first indicated for patients who cannot or are not willing to be examined with the ER coil, or if there is no ER coil available. Hence, at 3T, cancer detection seems to be comparable between 3T without the ER coil and 1.5 T with the ER coil. 32,45
Conclusion
T2-WI using multiple views remains the mainstay of PCa imaging. New multimodality techniques, however, using DCEMRI and DWI improve on both sensitivity and specificity in PCa detection and staging, especially for less experienced readers. DWI may, for the moment, not substitute for DCEMRI, because cancer and normal PZ have similar ADC values. 3T diagnostic indices for cancer detection seem to be comparable with 1.5T MRI. Multimodality imaging requires integrated interpretation and standardized reporting tools. Prostate imaging should be done at high resolution, no matter if it is using HR-ppA, ER coils or 3T.
Footnotes
Disclosure Statement
No competing financial interests exist.