
Abstract
Background and Purpose:
Robot-assisted pyeloplasty (RAP) has been established recently as an option in the management of ureteropelvic junction obstruction (UPJO). We present the first Canadian experience with RAP with respect to operative results and outcomes. We compare the surgical outcomes between experienced and trainee surgeons, with respect to operating room times and success rates.
Patients and Methods:
Eighty-eight patients underwent transperitoneal RAP for UPJO using the da Vinci robotic platform. Two surgeons performed Anderson-Hynes dismembered pyeloplasty in 85 cases and YV-plasty in 5 cases. Five patients had RAP for secondary UPJO after failure of other treatments. Diuretic renography was performed at 6 weeks, and 6, 12, 18, 24, and 36 months postpyeloplasty. The mean follow-up was 14.1 ± 8.5 months.
Results:
The mean operative time was 167.7 ± 43.2 minutes, and the mean anastomotic time was 41.9 ± 14.1 minutes. The mean operative duration significantly decreased with time (P < 0.05). Ten patients needed simultaneous nephroscopic stone management via the pyelotomy incision. The mean blood loss was 56.6 ± 55.4 mL, and the mean hospital stay was 2.5 ± 0.5 days. There were five major postoperative (stent migration, urinoma) and three minor complications that were associated with the RAP procedures. Postoperative renal scintigraphy demonstrated only four cases with persistent obstruction. Eighty-three (94.3%) patients experienced improvement of symptoms whereas 5 continued to be symptomatic. Two patients needed secondary procedures to relieve persisting obstruction. There were no statistical differences in outcomes between the experienced surgeons and trainees (P = 0.28).
Conclusions:
In the first large case series of RAP from Canada, we demonstrate that RAP can be performed with relatively short operative times and is safe and effective, achieving similar long-term results with standard open repair. We show that robot-assisted surgery can be safely transitioned to surgical trainees. With its cost and availability, its role in the Canadian system needs further study.
Introduction
Schuessler and associates 2 were the first to describe laparoscopic pyeloplasty in 1993. The laparoscopic surgery offered benefits of decreased postoperative pain, length of hospitalization, and postoperative recovery time, while maintaining the high success rate of open surgery. Since then, the procedure gradually emerged as a “gold standard” treatment for UPJO. 1
Robot-assisted laparoscopic surgery offers the potential to improve reconstructive laparoscopic surgical technique. Benefits of enhanced three-dimensional visualization, greater precision, and improved range of motion make robot-assisted surgery appealing. Most of all, robot-assisted surgery allows the surgeon to overcome technical difficulties with intracorporeal suturing, which is the rate-limiting step of traditional laparoscopic UPJ repair. 4,5 The wide increase in use of the robot-assisted surgery within the last decade, 6 in combination with the previously recognized benefits, identified RAP as a potential new standard of care. 7 In addition, the benefits of RAP have a potential to enhance the transitioning of this technique to surgical trainees.
In this study, we describe the first Canadian experience with RAP, in terms of operative results and long-term outcomes. We describe our experience with transitioning RAP to trainees, as well as the impact of trainee involvement on surgical times and outcomes.
Patients and Methods
Demographics
We performed a retrospective review of prospectively collected data from 88 consecutive patients who underwent robot-assisted laparoscopic pyeloplasty between March 2003 and June 2009 at our institution, following approval from The University of Western Ontario Health Sciences Research Ethics Board (#16511E) and Lawson Health Research Institute (#R-09-436). There were 49 women and 39 men in this study. All surgeries were performed by two staff surgeons (SEP, PPWL). Patients' presenting problems were flank pain (68), gross hematuria (1), microscopic hematuria (1), recurrent pyelonephritis (5), urosepsis (2), and renal failure (2); there was incidental discovery in 9 cases. All patients were initially investigated with either ultrasonography or CT. All patients underwent diuretic renography after the initial imaging study, which demonstrated delayed renal function. Thirty-nine patients had crossing vessels, which were preserved in all cases (Table 1).
Technique
At our center, all patients received full mechanical bowel preparation the day before surgery. All patients underwent ureteral stent insertion under fluoroscopic guidance just before the surgery, or an exchange of a previously inserted stent. Retrograde pyelography was performed in the same setting. 8
Pyeloplasty was performed with the patient in a lateral decubitus position. A three-arm port configuration was used. Dismembered pyeloplasty was performed on 83 patients and Foley YV-plasty on 5 patients. Any renal calculi that had been diagnosed previously were removed at this time by performing a small pyelotomy and using a flexible nephroscope with a stone basket. In one case, the calculus was inaccessible because of its location in a narrow neck caliceal diverticulum.
The anastomosis was performed based on individual surgeon preference. Surgeon 1, running suture with 5.0 polydiaxone suture; surgeon 2, interrupted suture with 3.0 polyglactin suture. Reduction of the renal pelvis was performed as assessed by the surgeon.
A case was defined as having significant trainee participation if the trainee performed bowel mobilization, UPJ dissection, and UPJ reconstruction in the same sitting. Trainees were inclusive of two clinical fellows (first and second year of fellowship, respectively) and a final year urology resident. The fellows performed seven cases, and the resident performed three cases.
Postoperatively, the bladder catheter was removed in 1 to 2 days. The close-suction drain was removed if there was no significant output increase, with patients voiding spontaneously. The ureteral stent was usually removed 4 to 6 weeks postoperatively.
Follow-up intravenous urography (IVU) or diuretic renography was performed 6 weeks postoperatively. Diuretic renography was repeated at 6 months and then at 12, 18, 24, and 36 months, if needed. Radiologically, success was defined as absence of obstruction on IVU or diuretic renography and either an improvement or stabilization of renal function on follow-up diuretic renography. A t1/2 of less than 10 minutes was considered normal with absence of obstruction.
Results
Thirty-four cases had a left- sided, 52 cases had a right-sided UPJO and 2 patients had bilateral UPJO (and underwent staged repair). Thirty-nine patients were found to have a crossing vessel at the time of the procedure. Eighty-three patients had RAP as a primary treatment; 5 patients had endopyelotomy performed previously. As well, 10 patients had associated renal calculi (Table 1) and 2 patients had renal cysts that were found to contribute to the obstruction and were decorticated. Two patients had horseshoe kidney and one had a pelvic kidney.
Between March 2003 and June 2009, 90 RAPs were performed at our center. The mean operative time was 167.7 ± 43.2 minutes (range 98–360 min). The mean operative time decreased with the increasing number of cases performed. Ten cases had a significant resident or fellow teaching component, which did not affect total operative time significantly (Fig. 1). The time to dock the robot decreased as the operating experience increased. The mean time to perform the anastomoses was 41.9 ± 14.1 minutes. The mean blood loss was 53.4 ± 34.9 mL (range 10–150 mL). There was one intraoperative complication involving injury to an epigastric vessel, which was recognized intraoperatively and managed without adverse sequelae (Table 1).
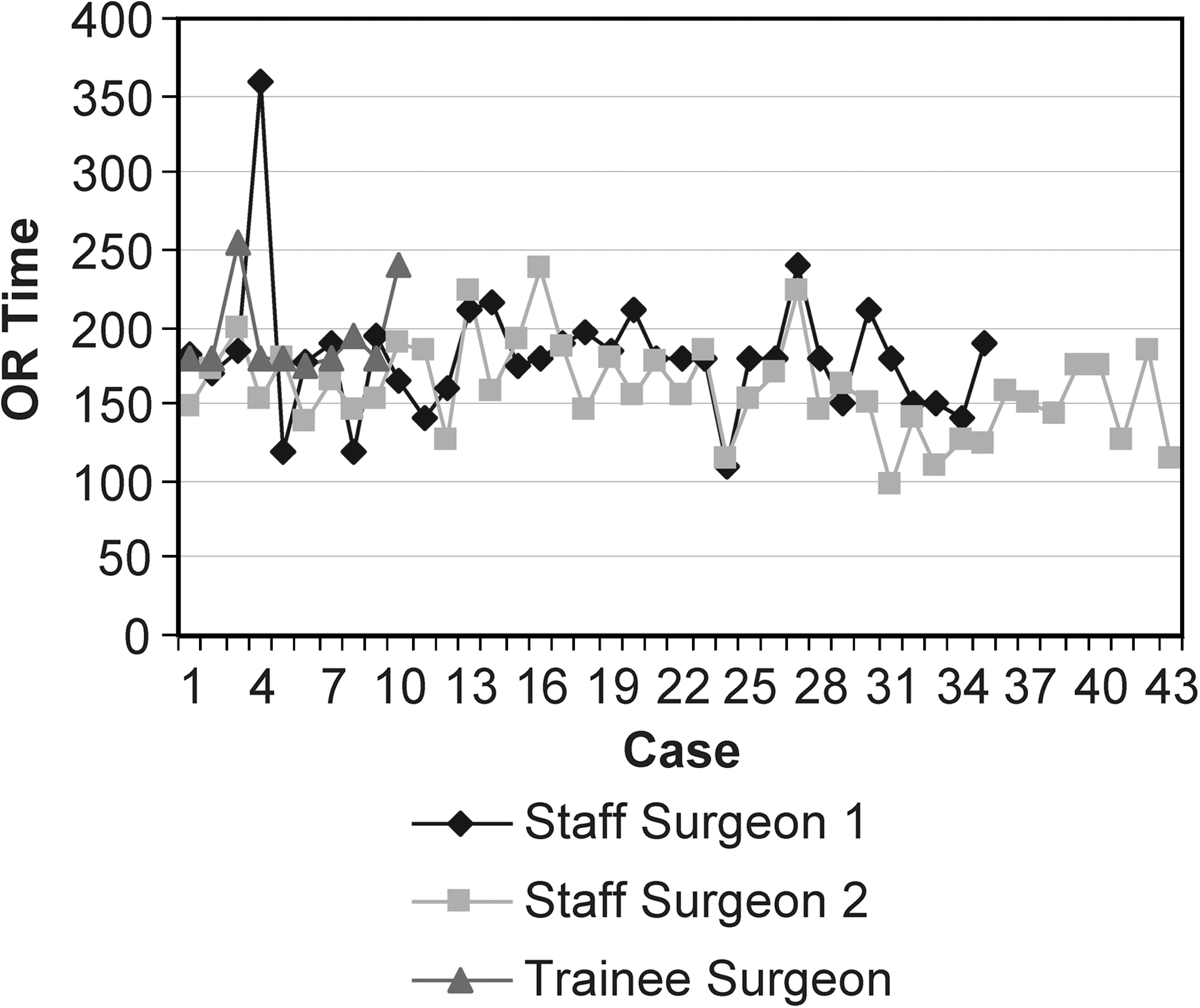
Comparison of total operative (OR) time between the staff surgeons and trainees.
Ten patients were found to have renal calculi preoperatively and underwent flexible nephroscopy and basket extraction of the calculi. The mean operative time was 176.4 ± 35.7 minutes for these cases. The stone-free rate was 90%.
The mean hospitalization was 2.5 ± 0.9 days. Five patients experienced major postoperative complications: Three patients had a migrated stent, one patient had a stent anchored with a renal pelvis anastomoses stitch, and one patient had a urine leak (necessitating percutaneous drain insertion and subsequent resolution) (Table 1).
Eighty-two patients experienced complete symptom resolution. Sixty patients were available for scintigraphic follow-up, 56 of whom were found to have scintigraphic resolution of obstruction. The resolution of obstruction was defined as t1/2 of less than 10 minutes. Long-term scintigraphic follow-up was not available for 28 patients. Four patients underwent secondary endopyelotomy for persistent obstruction. Five patients continued to have symptoms despite scintigraphic evidence of resolution of obstruction (Table 1).
The operative data and follow-up data for the first 10 cases were subdivided and analyzed according to the surgeon performing the procedure. The trainees were supervised by the staff surgeon and completed the UPJ dismemberment and reconstruction completely. All other steps of the surgery performed in isolation or without UPJ reconstruction were not considered as significant input. The mean operative times between the surgeons and trainees were 155.7 ± 28.2, 163.8 ± 20.5, and 196.1 ± 29.9 minutes, respectively (Table 2). There were no differences in outcomes between the three subsets of patients (P = 0.28) (Table 3).
No statistical significance (P = 0.28).
Discussion
Historically, UPJO was managed with open pyeloplasty. 9 Open pyeloplasty has a high success rate (above 90%), 9 –11 but it is associated with the morbidity of an open flank incision and prolonged recovery time. 12
Schuessler and colleagues 2 first described laparoscopic pyeloplasty in 1993. Since that time, laparoscopic pyeloplasty gradually emerged as a procedure of choice for managing UPJO in adults. 1 Jarrett and coworkers 12 published the largest single-center series with more than 100 patients, demonstrating a success rate of 96% and mean operative time of 260 minutes. 12
Although the pure laparoscopic approach offers advantages of decreased surgical morbidity and shorter recovery time, 13 –16 it has limitations. The main limitation of laparoscopic pyeloplasty includes its steep learning curve, which is directly related to intracorporeal suturing and knot tying. The nonwristed laparoscopic instruments offer only four degrees of freedom, and the standard laparoscopic camera offers only a two-dimensional view. 17
We reported the initial experience with RAP in Canada previously using the Zeus robotic system. 18 Since then, the da Vinci® platform became available, demonstrating its superiority. 19 After the initial experience, all the RAP cases were performed with the da Vinci robotic platform. To our knowledge, our series is the largest published series of RAP in Canada and one of the larger published series worldwide. We have performed a total of 90 pyeloplasties since the introduction of robotic technology at our center. In this series, two surgeons completed RAP in a mean of under 3 hours. Accordingly, the total operative time decreased with experience gained.
This series is the first to compare contemporaneous cases between staff surgeons and trainees. We compared mean operative times and outcomes in the first 10 cases performed by each group. As outlined in Table 2, the mean total operative time for trainees was 32 to 41 minutes greater than that of the staff surgeons. Importantly, there were no significant differences in long-term outcomes between the groups (Table 3). Therefore, we demonstrate that RAP can be safely transitioned to the trainees, with only modest increase in the total operative time.
At our center, the trainees are previously involved with pure laparoscopic renal surgery (radical and partial nephrectomy) and robot-assisted radical prostatectomy (to a smaller extent). We do not perform open or pure laparoscopic pyeloplasty. Trainees complete an annual “dry” robot laboratory that introduces basics of robot-assisted surgery and focuses on performance of simple tasks on the console, such as object transfer and suturing. Our lab includes porcine laparoscopic radical nephrectomy as well.
We conclude that the intuitive nature of the robot permits trainees to perform complex laparoscopic reconstructive surgery with relatively limited training. The ease of technique transition can be enhanced further with the introduction of a double console robotic platform, which will allow the staff surgeon direct involvement at the time of instruction.
In our current series, the success rate of pyeloplasty in providing complete symptom relief was 93%. Radiologic success in this series was also 93%, reflecting the clinical success. There were no robot failures nor were there conversions to open surgery for any reason. The overall complication rate in this series was low. The rate of stent migration was relatively high in our early experience. To address the stent migration complications, we now use a 30 cm Double-J stent in all patients who are undergoing RAP.
Robotic technology carries inherent disadvantages as well. Although the surgical principles behind RAP and pure laparoscopic pyeloplasty are similar, we acknowledge that the trainees were deprived of the experience of performing pure laparoscopic pyeloplasty. In the current Canadian system in which most centers do not have a surgical robot, this may eventually limit the ability of the trainee to perform minimally invasive UPJO repair.
Perhaps the most significant limitation of RAP is that of cost. The initial expense of the da Vinci robotic platform is more than $1 million, and annual running costs are in excess of $80,000. 20 Further study of surgical robotic costs in the Canadian Health Care System is needed.
Conclusions
This is the first large case series of RAP from Canada. We demonstrate that RAP can be performed with relatively short operative times and is safe and effective, achieving similar long-term results with those of standard open repair. The procedure can also be easily transitioned to surgical trainees. With its cost and availability, however, its role in the Canadian system needs further study.
Footnotes
Disclosure Statement
No competing financial interests exist.