
Abstract
Focal renal therapy for small renal masses (T1a or T1b) has been used as primary treatment for patients with comorbidities who are considered poor candidates for surgical resection. With a continuing effort toward optimization of minimally invasive nephron-sparing modalities, the effort to expand the patient pool will continue. As long-term results of renal ablative therapies become available and the safety, precision, and efficacy become well established, renal ablation may be used with increasing frequency for a wider group of patients. When this happens, high-quality imaging for localization and targeting of these renal lesions will become the central core of the treatment, with emphasis on superior results, accurate positioning of the probe, precise localization of the tumor, and real-time intraoperative monitoring of outcomes.
Introduction
Radiofrequency ablation (RFA) and cryoablation are the two most popular techniques used for renal ablation. Local tumor eradication is the primary aim of treatment. Avoidance of the risk of major surgery has, until now, been the primary reason for performing these procedures, however. Therefore, in many centers, this modality is currently reserved for the high-risk patient who is not considered a good candidate for surgical excision. We believe that this promising modality should not be limited to poor risk candidates and offer it to many healthy, younger patients.
With a continuing tendency toward more minimally invasive nephron-sparing modalities, the effort to expand the patient pool will continue. As long-term results of renal ablative therapies become available and the safety, precision, and efficacy become well established, renal ablation is predictably going to be used with increasing frequency. More patients without significant comorbidities could, in the future, be treated primarily by percutaneous ablation performed on an outpatient basis. When this happens, high-quality imaging for localization and targeting of these renal lesions will become the central core of the treatment with emphasis on superior results, accurate positioning of the applicator, precise localization of the tumor, and real-time intraoperative monitoring of outcomes. At the moment, ice-ball formation or peripheral thermometry are the only reliable means of assuring adequate tumor coverage.
This review will look at the role of targeting in renal focal therapies, the need for precision, and the consequences of imprecise targeting.
Principles of Targeting/Navigation
Renal ablation is a minimally invasive option for the management of small renal tumors that has lower costs, minimizes patient morbidity, decreases convalescence, and improves the chances of early return to work. The main aims behind using advanced image-guided navigation systems for renal ablation is to have the accuracy that will enable the operator to destroy the same predetermined volume of tissue that would have been removed had a conventional surgical excision been performed.
All forms of surgical or interventional therapies require a good understanding of the regional anatomy and precise localization during the procedure. Unlike open or laparoscopic techniques in which the surgeon can see the tumor, during percutaneous ablation, the surgeon has to depend heavily on high-quality cross-sectional imaging to achieve good results.
Renal focal therapy with optimization of targeting can be divided into four components (Tables 1 and 2). The first of these is treatment planning, which comprises identifying the tumor(s) and adjacent structures at risk, locating potential heat sinks that can affect outcomes, and making a preoperative plan of the approach, the probe sizes and types, and the number of applications to be used.
Cryo = cryoablation; RFA = radiofrequency ablation; US = ultrasonography; CT = computed tomography; CEUS = contrast-enhanced ultrasonography; MRI = magnetic resonance imaging; lap = laparoscopy; intraop = intraoperative; FAIR = flow-sensitive alternating inversion recovery; FISP = fast imaging with steady state precession.
The first component of this step is to segment the kidney into normal tissue, tumor, and key vessels and structures, such as the collecting system and the ureter. Preoperative assessment and planning performed using currently available imaging modalities requires that the treating physician perform the entire three-dimensional (3D) reconstruction and conceptualization in his or her mind. This is difficult for complex nonspheroidal tumors but can be near impossible when the kidney has many lesions or cysts and the tumor is surrounded by or in close association with other cysts.
The second step involves probe placement and ablation under image guidance—the placement of the applicator or temperature probes in the exact spatial location in relation to the tumor. With the advanced machines and software that are fast becoming available in many centers, virtual ablation needles can be positioned on a simulation—on the preablation CT image along with superimposition of predefined virtual treatment zones of different shapes and sizes. 2
Intraoperative targeting and monitoring continue to be a challenge, however. For needle insertions, most centers continue to use ultrasonography (US) and CT. 3,4 Studies of liver masses have shown that US visualization can be poor, and even preoperative contrast-enhanced CT may not provide adequate visualization. 5,6 In such situations, estimation of target position is performed by using nearby discernable anatomy and a “mental coregistration” on a previously obtained two-dimensional (2D) or 3D image. 7
Some commonly used modalities of imaging for this step are shown in Table 2. Most authors perform the initial follow-up CT or MRI with contrast in the first 6 weeks (Table 2). Evidence of failure includes enhancement on follow-up CT (defined as an increase from a precontrast 10 Hounsfield units (HU), 8,9 or 20 HU, 10 or simply reported as “enhancement”), or a positive biopsy from the ablation site at 6 months, 11 or a 15% signal increase on MRI. 8,9 Tumor size increase was used as a criterion rarely, 12 and one author used contrast-enhanced US (CEUS) for follow-up treatment monitoring and follow-up. 13
There is less uniformity in assessing real-time end points of the treatment in the literature. Some form of temperature monitoring or monitoring of ice-ball formation was performed by most authors (Table 2). Impedance roll-off in RFA was used exclusively by one group, 8 but these authors also routinely used overlapping spheres of treatments for their patients. In a series of patients with renal-cell cancers, Park and associates 14 used the manufacturer recommended setting of 12 minutes RFA time with a success rate of 72% for the first ablation. We would recommend some caution in just following the manufacturer recommendations, because different tumors have different characteristics, and multiple tissue/organ variables, such as vascular flow (heat sink effects), lipid content, and conductivity, can alter the end effect even using the identical power and time settings. We routinely advocate the use of nonconducting peripheral temperature monitoring. 10,15
Immediate postablation contrast CT or MRI was used by some authors. 9,12,16,17 Ganguli and colleagues 17 have also described a phenomenon of postablation involution in the size of tumors, with a mean tumor size decrease of 5.4 mm in patients who were undergoing renal RFA.
Clearly, there is some variability in the way the procedure is performed, completeness of ablation is assessed, and long-term follow-up is performed. With more experience in this field, we expect better consensus on many aspects of renal ablation.
The third step essentially monitors the adequacy of ablation. This means real-time visualization of changes in characteristics of tissue with progression of treatment. Thermal monitoring is important for all modalities using thermal energy for ablation. In cryoablation, temperatures less than −20°C have been shown to be lethal to cells. 18,19 In RFA, temperatures above 55°C are lethal. 19 Thermal monitoring with nonmetallic thermistor probes is one way of using preset temperature end points as a surrogate marker of adequacy of treatment. Thermometry can also be performed by using sophisticated software. Changes in CT HU have been shown to correlate with temperatures, and mathematical models using finite element analysis of the bioheat equation have also been used. 2 This is currently in an investigational stage, and tweaking the components of the mathematical function can even adjust for and consider the effects of blood flow, tissue characteristics (such as fat or salt content), and proximity of adjacent vital structures. 2 As part of monitoring, the operator also needs to avoid complications.
Post-treatment, a CT or MRI with contrast needs to be performed to identify incomplete ablation or recurrence. Although there are no established protocols, most surgeons would prefer to obtain a contrast CT or MRI within the first 6 weeks and then repeated imaging twice in the first year. After that first year, follow-up needs to be modified to suit the patient. If the pathology report shows a benign condition such as angiomyolipoma, follow-up can be performed on an annual basis. Renal-cell carcinomas may be followed with CT/MRI every 6 months for a total of 2 years and then CT scans annually.
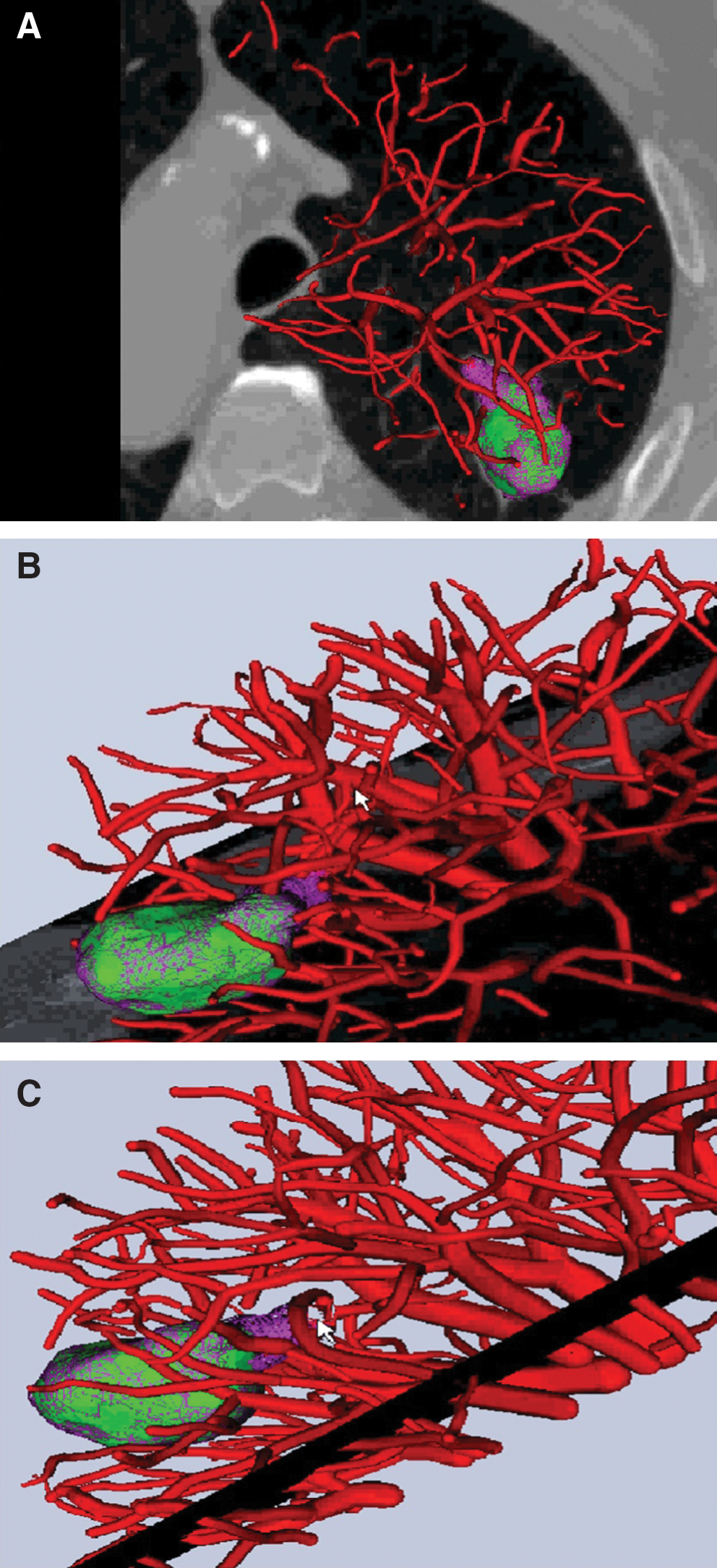
The follow-up imaging can use stacked images over a period using time as a fourth dimension. This means that progression of tumor will be recorded as stacked superimposed color-coded images over baseline images (Fig. 1). Progression will then be seen as spillage of different colored sectors outside the boundaries of the baseline image (Fig. 2). The software for this is currently being developed to incorporate this complex imaging overlay by Intio Inc.
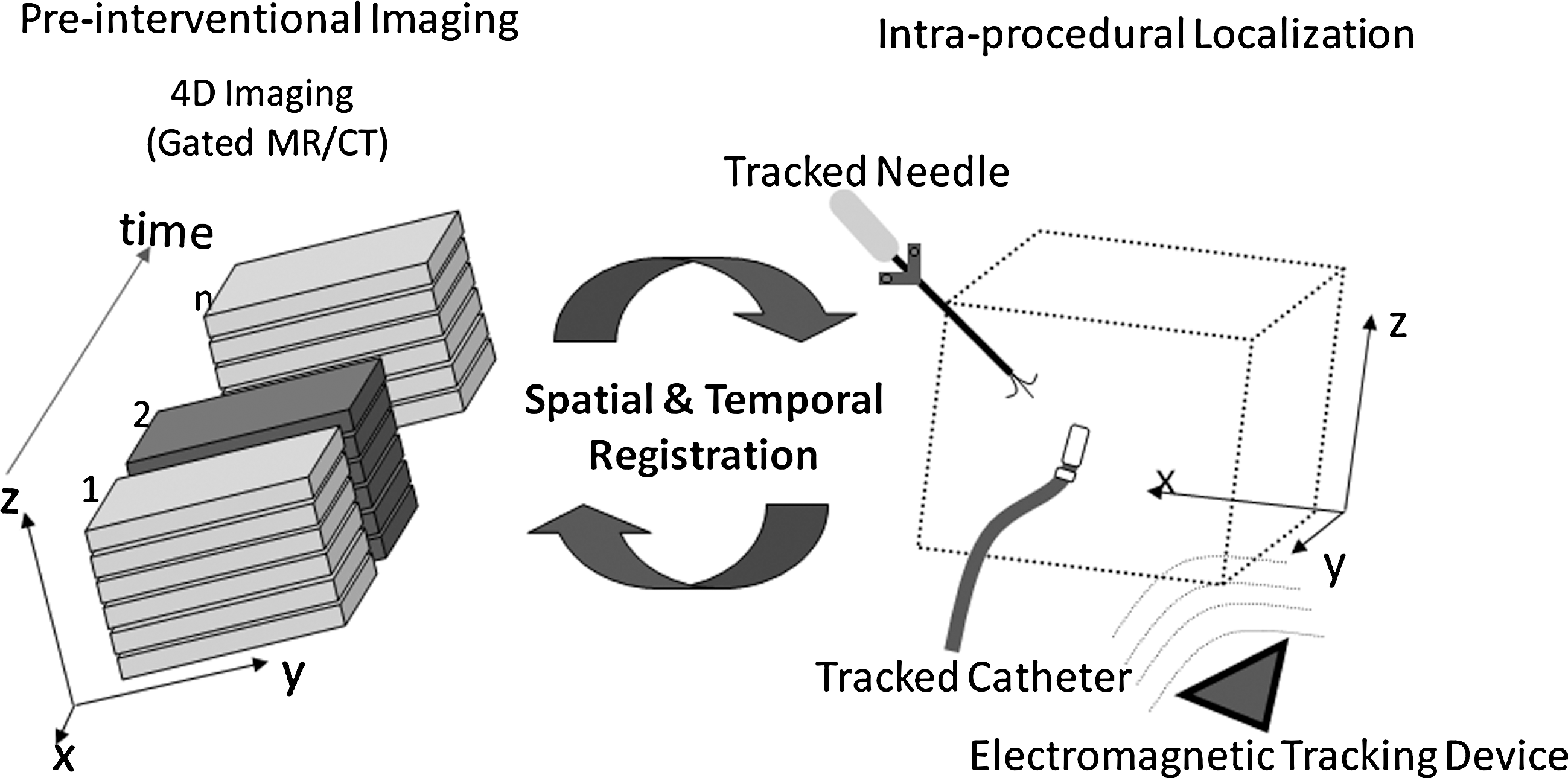
Concept of time as the fourth dimension. Three-dimensional reconstructions are very useful for treatment planning. A tumor could progress or enlarge in time, however. This can be captured and superimposed using digital addition and subtraction. Electromagnetic tracking can then be used for navigation and targeting, with or without robot assistance. Reprinted with permission from Veran Medical Technologies Inc.
Medical navigation essentially uses geometric and anatomic data in patients and enables the operator to approach a target position by fixing the spatial relationship of interventional equipment with respect to organs in the patient 20 and can be performed with CT or MRI guidance. Optical tracking uses 3D cameras to determine the position of an instrument (tracking) and achieves this by using either active tracking (use of light emitting diodes) or passive tracking (use of reflected light). 20 Electromagnetic (EM) tracking uses EM needle tips and matching sensor pads. The sensor pads, which have been previously placed on the patient's body, act as fixed reference points (Fig. 3).

Electromagentic tracking using the Veran System in a mannequin model. The tracking markers are placed over the abdomen (white squares), and the needle is connected to the tracking module. In the top panel, the needle is over the abdomen and the image reflects the position and angle of the needle. As the needle is moved up, the axial cuts on cross-sectional imaging shows the location over the upper thorax with the underlying lung (lower panel). Note the point of entry on the skin changes with lateral displacement and the line of trajectory changes when the needle is tilted (lower panel). This ensures complete 3D tracking of the progress of the needle toward the target lesion. Reprinted with permission from Veran Medical Technologies, Inc.
The basic components of advanced imaging systems that are necessary during treatment include: Equipment and software capable of 3D reconstructions using CT or MRI to visualize the tumor and other nontarget structures; real-time 3D guidance using various tracking techniques; and monitoring progression of treatment by thermometry or isotherm mapping or projected zones of ablation using bioheat equations and finite element analysis.
To accurately display the instrument position with respect to the patient position on sectional imaging, the exact spatial relationship between patient anatomy and CT or magnetic resonance (MR) scanner needs to be determined by the computer as a mathematical transformation, a procedure referred to as coregistration. 20 If the patient remains in the scanner without moving or being moved, the primary spatial relationship between the patient and MR scanner does not change and coregistration is easy. 21 If, however, the patient is moved with respect to the scanner, the new patient position needs to be registered again using repeated imaging to search and map fiducials or well-recognized common anatomic landmarks in the patient. Repeated patient movements may necessitate multiple and repeated acquisitions of the image data and coregistration with the latest patient position—a procedure called navigation update. 20 All of this necessitates advanced high-quality imaging, computers, and appropriate software.
Medical navigation can provide static or dynamic guidance. Neurosurgeons have been using stereotactic approaches for many decades, and this is a form of static guidance that can be readily used on parts of the body where there is no movement (because of respiration or arterial pulsation) of organs with respect to each other. Based on measurements, changes in patient orientation caused less than 1 mm of gravity-induced movement of the brain in the closed cranium. 22 Static guidance can therefore be used readily on the brain. This modality, however, may not be appropriate for an intra-abdominal organ such as the kidney. Dynamic guidance with orientation of the slice in such a way that the instrument is displayed along its entire length may be a better alternative, because this allows for freehand navigation. 20
Real-time imaging is very helpful for accurate needle placement. Because real-time dynamic image guidance necessitates repeated image acquisition and capture, this technique involves significant radiation exposure when CT is used. MRI can be used instead of CT, but the chief limitations are the cost and use of nonmagnetic instruments, as well as special shielding.
Integration of high-resolution US as the real-time imaging modality with CT seems to offer a way around this problem. This real-time fusion of US and CT image is made possible by EM tracking of the ultrasound probe. Registration is a process of bringing two image data sets into spatial alignment, and fusion is the integration of complementary information provided by the different modalities. 2 The 2D US image is superimposed with variable opacity and blended onto the corresponding slice on the CT scan. Movements of the ultrasound transducer allow for integrated translation of the change in position because of real-time updating of fused US and CT images. 2
Various devices using different technologies have been developed to assist with targeting and accurate placement of the probe. Some use 3D reconstructions and CT-integrated stereotactic arm (PinPoint, Marconi Medical Systems) while others use EM tracking (Percunav, Traxtal Inc, and Philips Medical Systems), and IG4 (Veran Medical Technologies).
Need for precision
Ablations, especially using RF, can be optimized using some form of peripheral temperature monitoring (Figs. 4 and 5). Temperature monitoring allows the surgeon to identify potential areas of inadequate ablation and helps in relocating the probe to target these areas. Given the importance of temperature monitoring, many ablations are performed with multiple probes (with or without multiple applications) and temperature sensors (Fig. 6). For a tumor that measures 4 cm, often three RF applicators and four temperature sensors are used. This means using six needle devices within a small area. These devices, therefore, need to be placed with extreme precision.

Effect of not using temperature sensors. (

When temperature probes are routinely used (

The need for precision: Many ablations (both laparoscopic and image-guided percutaneous ablations) are performed with multiple probes (or in the least, multiple applications) and temperature sensors. For a tumor that measures 4 cm, multiple devices will need to be placed under extreme precision within a narrow area.
The percutaneous approach for RFA of kidney lesions, although less invasive, has, in general, a higher incomplete ablation rate compared with the laparoscopic approach, with recurrence rates ranging between 14% and 18%, 23 and it is unclear how much of this is possibly because of inadequacies in targeting. As with RFA. percutaneous techniques for cryoablation of kidney tumors are less effective compared with laparoscopy, with recurrence rates ranging between 13% and 21%. 24 Patient selection and intent to treat may also contribute to these higher failure rates. The absence of visual cues during percutaneous ablation may result in less precise placement of probes or temperature sensors and may be responsible for this difference.
Multimodality guidance enabled by EM tracking of devices can also augment single-modality imaging guidance, 25 –27 and improvements in basic tracking error from 5.8 mm ± 2.6 to 3.5 mm ± 1.9 have been described. 7 Computers and robots under direct human guidance and with direct human input further improve the accuracy of targeting. Average placement accuracy of 1.44 mm ± 0.66 mm can be expected with the use of a robot, as seen in a study performed on a cadaver model with preplaced metal beads, using fluoroscopy for image guidance. 28 In this study, in most cases the physician was able to drive the needle directly toward the target. In some cases, however, the needle deviated slightly, and the physician needed to correct the needle path by reorienting the needle slightly in the direction opposite to the deviation. 28
Consequences of imprecise targeting
Incomplete ablation
Inaccuracies of a few millimeters or angle changes of a few degrees can get amplified based on the distance of the target from the skin, because the pivot of the needle trajectory is on the skin surface. For a given angle, the degree of spatial displacement of the needle from the intended primary location during planning gets larger as the distance from the skin to the tumor increases (Fig. 7). This can result in a volume of tissue different from the planned amount being ablated, and residual unablated tumor can be the result (Fig. 8).
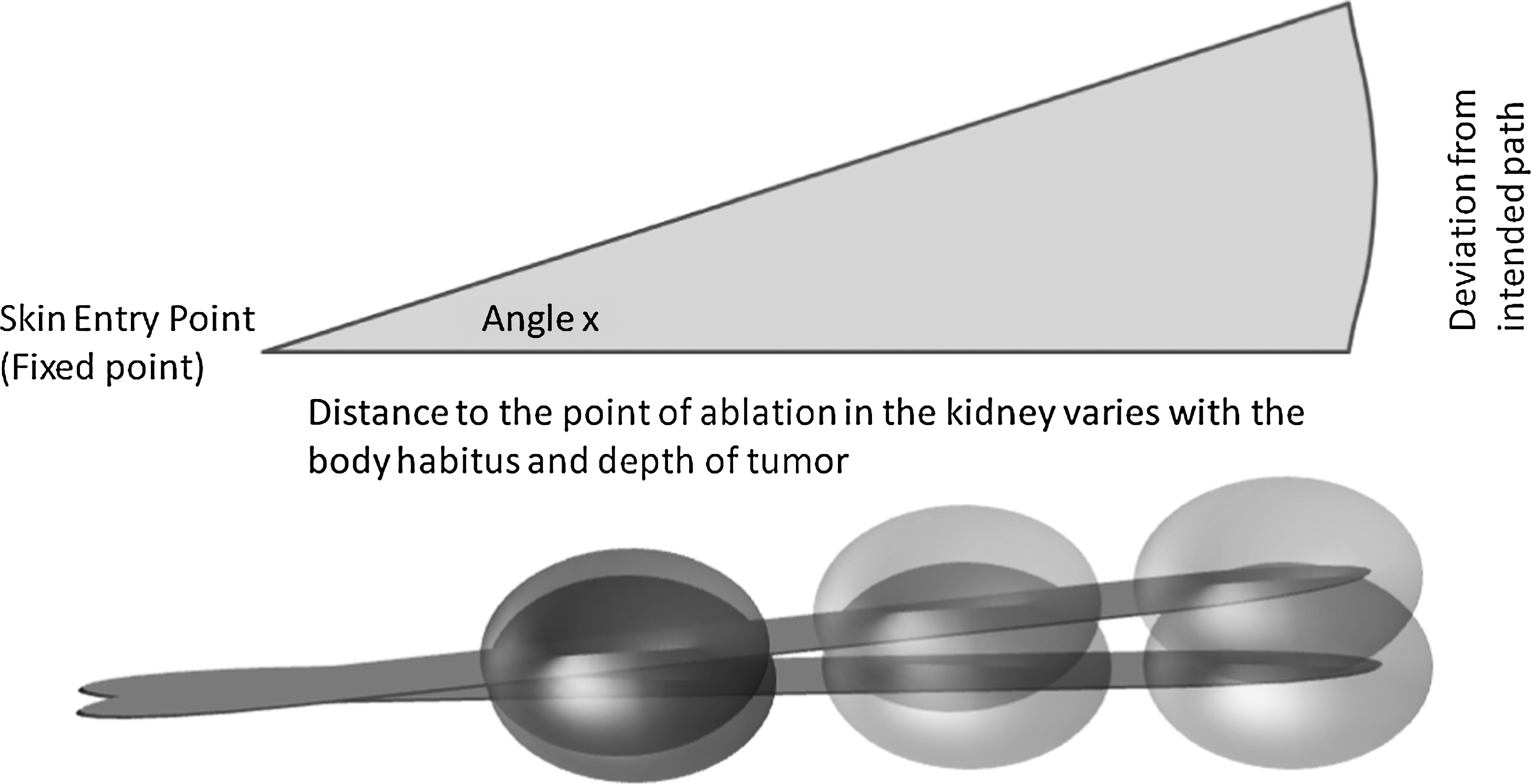
Effect of inaccurate probe placement. The lower line shows the intended trajectory; the upper line depicts the actual trajectory, and the angle of error is ‘x’. Even for a small ‘x’, the targeting error gets proportionally magnified as the distance of the targeted lesion increases from the skin.

Consequence of improper targeting (or improper needle placement) is incomplete ablation. (
Incomplete ablation can also occur in two specific situations. The first is in relation to a large blood vessel that has a significant heat sink effect. Inability to visualize and realize this situation can cause an ineffective ablation zone (Figs. 4 and 5). The other situation relates to multiple applications. When multiple probes are used, 3D imaging is helpful in visualizing the area of overlap.
Time taken for the procedure
Imprecise targeting can cause imprecise needle placement, and this can have an impact on the time taken for the procedure. Current ablation cycles using a standard Cool-tip® probe are approximately 6 to 12 minutes. If two cycles need to be used, ablation times of up to 30 minutes are common; this is a fourth to a sixth of the whole procedure, which for a CT-guided percutaneous RFA procedure can range from 2 hours to 4 hours. Movement from breathing or changes in patient positioning can further contribute to inaccuracies and increased procedural time.
Complications, adjacent organ injury
Inaccurate registration between planning images may be responsible for multiple needle punctures and repeated relocations. This can increase the risk of bleeding or pneumothorax as a direct consequence of the increase in the number of interventions. Many of the above complications are related to proximity of the tumor to neighboring organs. 29 The patient's mobile organs, such as the bowel, can move as a consequence of positioning or from respiratory motion. If this is not recognized and adjusted for, adjacent organ injury can occur.
Thus, there is a need for continuous dynamic feedback during the procedure. This is particularly true for small renal masses on the posterior and medial aspect of the lower pole of the kidney. These could sometimes be in close relationship with the ureter. Ureteral strictures have been reported, 15 and these could be minimized by the use of highly precise targeting as well as temperature monitoring and anatomic knowledge.
To avoid many of these complications, the distance between the tumor and neighboring organs can be increased by changing the patient's position, using the RF electrode as a lever, or hydrodissection. 29 Laeseke and coworkers 30 described the use of 5% dextrose in water (D5W), which is a nonelectrolyte solution. Hydrodissection with D5W can protect by creating an insulating envelope around the adjacent structures, minimizing the risk for complications such as bowel perforation. 31 Pneumodissection by injecting CO2 around the tumor avoided thermal injury in patients who were undergoing RFA. 32
Both CO2 and D5W, however, can dissipate or undergo resorption, and therefore repeated injections in the proper plane of dissection may be necessary to maintain adjacent organ displacement, away from the probe. Repeated injections have their own risks, and injection in the wrong planes can have serious adverse effects.
Additional maneuvers to achieve extra bowel displacement could include additional manual torquing of the RFA probe and use of angioplasty balloon interposition. 33 When the electrode is used as a lever, the distance between the tumor and bowel during percutaneous CT-guided RFA is increased by more than 5 mm, and no thermal injury to the bowel was noted. 34
The ureter can also be protected by using infusions of chilled solution via ureteral catheter or nephrostomy. 35 The technique of using cooled D5W retrograde pyeloperfusion is particularly recommended for patients who are undergoing ablation of tumors within 1.5 cm of the ureter. 36
Inadequate temperature probe placement and inadequate monitoring
Inappropriate temperature probe placement can result in inadequate monitoring. Probes should ideally be placed approximately 5 mm from the tumor edge, and these probes should register at least 60°C (lethal temperatures) for RFA and less than −20°C for cryoablation. Probes placed into the tumor or more than 1 cm away from the edge of the tumor may give a falsely abnormal reading. This can cause unnecessary redeployments of the ablation needle, inapproriate heating, and, therefore, inappropriate ablation. Advanced thermal models and noninvasive thermal mapping with color-coded isotherms that can be fused with the source CT images would be very useful. These thermal models can even be fused with the intraprocedural CT reconstructions to visualize areas that have been (or have not been) ablated, and this can provide intraprocedural feedback 2 and help the operator to redirect the applicator.
Targeting for accurate temperature probes placement can be equally challenging. Deviation from the intended path can result in an abnormal placement of the temperature sensor with its effect on the temperature recorded. In cryoablation, there is rapid warming toward the periphery, 19 and the edge of the ice ball has to extend at least 3.1 mm outside the tumor margins to cause adequate cell death. 37 A displacement of 2 mm in an outward direction away from the probe can cause a temperature decay of approximately 5°C to 10°C.
Targeting Techniques
Percutaneous needle insertion for RFA or cryoablation therapy and treatment monitoring can be performed using US, fluoroscopy, CT, or MRI guidance (Table 3). 38,39 Real-time US is generally used during the procedure to guide electrode placement, but for evaluating the results of treatment, contrast-enhanced CT and MRI have traditionally been considered more effective. Each has some limitations (Table 4), and now multimodality imaging with coregistration and fusion of CT imaging and real-time US is becoming more readily available. In general, for needle insertions, US and CT are the primary guidance modalities. 3,4 The registration and fusion of real-time US with a preacquired 3D image, such as CT, addresses some of these difficulties. 3,12 Trajectory planning is possible in the 3D image, and placement can be verified in real time using the US image. 2
Cryo = cryoablation; RFA = radiofrequency ablation; US = ultrasonography; CT = computed tomography; CEUS = contrast-enhanced ultrasonography; MRI = magnetic resonance imaging.
CT = computed tomography; MRI = magnetic resonance imaging.
Sonography-guided ablation
US allows the body to be scanned from various positions and angles. The images generated by conventional cross-sectional images (CT/MRI) are displayed as horizontal tomographic slices and need some mental reconstruction of a 3D model of the body from many 2D horizontal images. Real-time virtual US (RVS, Hitachi Medical Corporation) is a variant of technology that allows the fusion of real-time US and preoperative CT data. 40
On a sonogram, the ablated area shows increased echogenicity as the temperature rises and tissue coagulation necrosis occurs. 41 When tissue is heated, dissolved gases are released to form microbubbles in the tissue, which appear as hyperechoic foci (referred to as “gassing out”) and sometimes escape into adjacent vessels. Although this phenomenon may provide general information about the area being ablated, one cannot predict the size of the necrosis on the basis of this information.
The deterioration of the US image (Fig. 9) by gas microbubbles released during thermal treatment along with limitations because of nonavailability of suitable windows from bowel gas or intervening bone (eg, overlying ribs) imposes major restrictions on the routine use of US as a stand-alone modality for renal ablative therapies. Also, the visualization of the needle is dependent on the needle angle and is limited by partial-volume averaging. 42 In fact, US as a stand-alone imaging modality thus seems to be the least favorable for RFA. 43 US is also not very useful for monitoring during cryoablation, because progressive ice-ball formation impedes transmission of the ultrasound waves and disables adequate monitoring of the opposite side of the lesion as treatment progresses.

Deterioration of ultrasonographic images with continuing radiofrequency ablation (gassing out).
The limitation of monitoring ablation outcome during the procedure could be overcome in part by using CEUS. CEUS has been used to monitor the RFA procedure in hepatic tumors. 44 CEUS using sulfur hexafluoride microbubbles has been shown to provide valuable information on the effects of RFA in an effective and more economical way compared with CY or MRI in liver ablations and without exposing the patient to ionizing radiation. 44 Lack of flow, however, is not adequate, because edema, thrombosis, and image degradation may all result in false positives. Temperature change to >60°C should be considered the lethal end point.
US with Doppler flow imaging can be helpful to show the vascular structures adjacent to the tumor and can impact on planning the needle route to avoid inadvertent vascular injury and also to take into consideration the potential heat-sink effect related to larger vessels nearby.
CT-guided ablation
CT is currently one of the most widely used imaging modalities for renal ablative therapy. All RFAs performed percutaneously at our institution use CT guidance. The capacity to build 3D reconstructions is extremely helpful in treatment planning. These give the operator the ability to form a 3D map of the organ and appreciate spatial relationship of needle trajectory and its relationship to the pleura, lung, and adjacent nontarget structures such as the ureter or bowel. A 3D projection also can show spatial relationship to overlying structures (eg, ribs) that are considered zones of no entry, or, can also segment the organ into normal tissue, tumor and key vessels. The capacity to develop a good thermal treatment plan lies on the principle of ablating all tumor and avoiding injury to local key structures. 3D reconstructions with the needles in place can show the spatial relationship of the tumor and needle and temperature probe (Fig. 10). The Clearview™ Oncology Visualization System (Intio) leverages state-of-the-art graphics processing capabilities coupled with proprietary software algorithms to register multiple CT image sets in real time (Figs. 1 and 2).
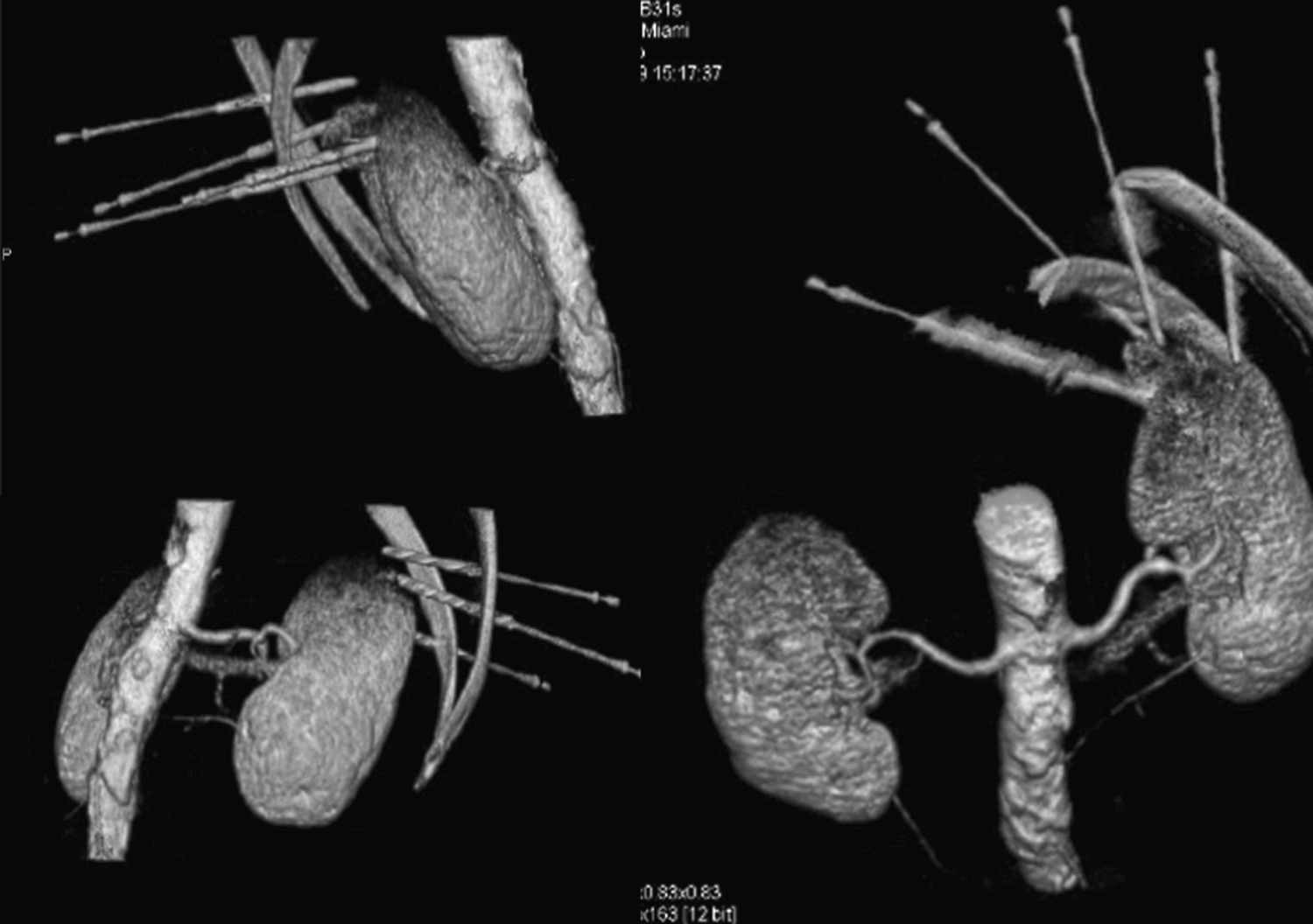
Three-dimensional reconstruction views of kidney and tumor (seen on the top of the left kidney) and spatial relationship to ribs. Also seen is the location of the temperature probes in relation to the tumor.
Role of tracking
Standard techniques for registration include optical (active or passive) and EM tracking. Optical tracking uses light (either from diodes active or reflected light passive) and needs an unobstructed line of sight, which may not be available during image-guided renal ablation. EM tracking is thus more commonly used and involves the use of position sensors that provide location information of the tracked device (which could be the needle or catheter). 26 Matching sensor pads previously placed on the patient's body act as fixed reference points 20 (Fig. 3). Tracking allows for use of preprocedural images, dynamic movement of the tracked device during the procedure, and the option of dynamic fusion and use of multiple modalities, such as real-time US plus preoperative CT (Fig. 3).
EM tracking uses fiducial skin markers that are placed at the time of preprocedural CT or MRI, or at the beginning of the procedure. The ablation navigation system (Fig. 11) then allows multiple preprocedural imaging modalities to be used with real-time feedback during the RFA, showing the location of the electrode and treatment zone in relation to the enhanced CT or MRI target. 45
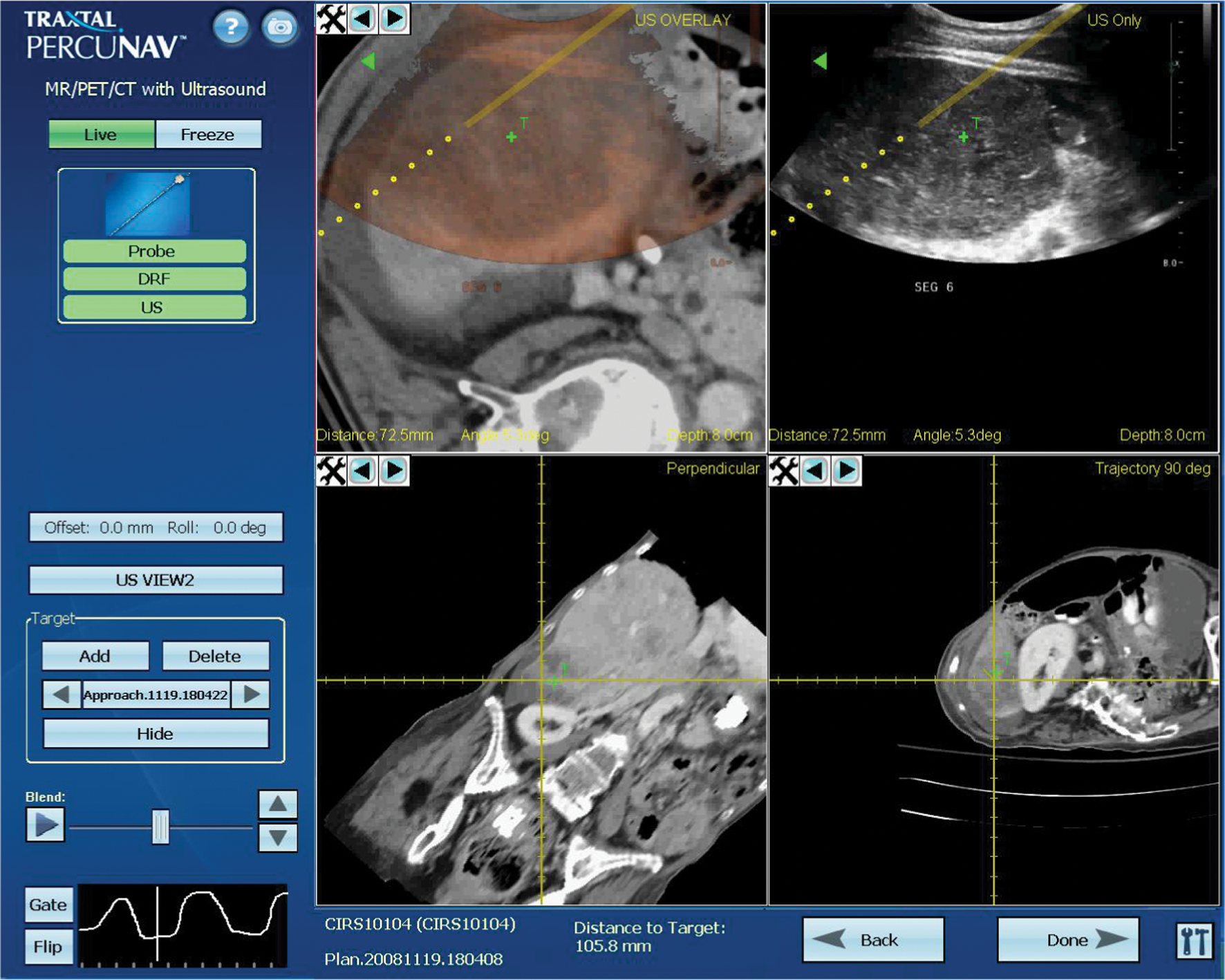
Imaging system with navigation screen, showing fusion of ultrasonography and CT. Upper right panel shows a real-time ultrasonographic imaging of the liver and overlay on a CT image (upper left panel) along with probe angles and target “T,” distance to target of 105.8 mm along the trajectory of the probe (lower two panels). Reprinted with permission from Traxtal Inc.
Robot-guided ablation
CT–integrated robotic needle placement along a predetermined trajectory is now possible with the use of a gantry-mounted robot that is integrated to work with the scanner's 3D coordinate system. The CT-integrated robot is able to insert the needle with a pneumatic gripper using remote controls (automatic insertion); or the physician may choose to do it in a laser-guided semiautomatic manner with the laser pointing out the correct angulation and insertion point for the needle. 46 “Point-and-click” ablation is possible after rapid selection of virtual skin entry and target points with the planning display of resulting ablation volume. 2 The CT-integrated robot (National Institutes of Health, Bethesda, MD, and Philips Medical Systems, Cleveland, OH) is different from other previously reported CT-compatible robots in that it is a single platform with true seamless integration and does not need the time-consuming steps of frame grabbing, accessory computers, intraprocedure registration steps, or extra software. 47
Laser-guided ablation
Intersecting planes of helium neon laser light beams have been used in the past to accurately localize lesions for biopsy. 48 This system used perpendicular planes of light to guide needle passage and has demonstrated accuracies of ±1 mm and ±1°. Gantry-mounted laser guidance systems 49 are available for treatment planning on most newer CT machines and are used for image guidance with the use of a radiopaque grid of skin fiducials. Nongantry-mounted, freestanding systems 50 have the distinct advantage of allowing laser-guided access even after the patient is removed from the scanner.
Monitoring of Ablation and Thermometry
We have routinely used fiberoptic probe thermometry for monitoring of temperatures during ablation. 15 When dealing with small tumors, placing three or four temperature monitors around the tumor can be challenging. Noninvasive temperature monitoring using MRI has been used in some studies. Temperature-sensitive MR parameters, such as the proton resonance frequency (PRF), the diffusion coefficient, T1 and T2 relaxation times, magnetization transfer, the proton density, as well as temperature-sensitive contrast agents can all be used. 51 Because the RF generator interferes with MRI, it might be necessary to use a switching circuit to alternate between power application and imaging, 52 and this can increase the time taken to perform the procedure. By using the current filtering technique, 53 however, temperature maps can be obtained simultaneously during RF application. In general, PRF-based temperature mapping has by far the greatest acceptance for many applications. 51 The biggest limitations of MR thermometry are because of the inadequacies in fat-rich tissue and artifacts from interscan or intrascan motion. Fat suppression can be used to help to reduce errors from fat.
Conclusions
EM tracking and advanced navigation systems have the potential to revolutionize the management of renal tumors. Real-time guidance provided by the newer imaging modalities ensures efficient tumor ablation without significant complications. Routine temperature monitoring is made possible because of the ability to place probes with precision in a small area and will be useful until CT thermography becomes routinely available. Completely automated robot-driven RFA, in which the surgeon outlines the needle path and encircles the target area on a console, with the robot performing the rest of the procedure, may become a reality in the not too distant future. Urologists should become knowledgeable about these newer technologic advances and embrace their development as more and more in situ treatments will likely replace the scalpel and scissors.
Footnotes
Disclosure Statement
Rajan Ramanathan: No conflicts of interest exist.
Raymond Leveillee: Angiodynamics, research contract with University of Miami; Covidien, research support (equipment) for lab (no financial remuneration); Intio, research agreement with University of Miami (no financial remuneration).