
Abstract
Introduction:
The aim of this study was to review recent advances and to provide future perspectives in renal focal therapy.
Methods:
Most relevant available data from current literature and reports from major urological meetings as well as clinical and experimental experience at our institution have been considered.
Results:
Effective treatment of incidentally detected small renal masses continues to evolve. Major recent advances have been made toward three main directions: enhancing accuracy of probe positioning, improving ablative energy efficiency, and reducing treatment-related morbidity.
Conclusions:
Renal focal therapy can offer the advantage of combining a nephron-sparing surgery together with a minimally invasive approach. Technical refinements will include emerging clinical data for radiofrequency and cryoablation. Single-port access renal cryotherapy has been shown to be feasible and safe. Although in its infancy, natural orifice translumenal endoscopic surgery might represent a further step toward scarless surgery. Radiosurgery is under investigation and oncological outcomes are awaited to determine its role. Stereotactic surgical navigation and robotic needle placement would facilitate and increase the accuracy of percutaneous probe placement.
Introduction
Probe-ablative treatment of small renal masses have been applied for selected cases, with the potential benefits of decreased morbidity, shorter hospitalization, earlier return to normal activities, preservation of renal function, potentially lower costs, and the ability to treat patients who are at poor surgical risks. 3
Several ablative technologies that have been investigated either clinically or experimentally include cryoablation, 4 radiofrequency ablation (RFA), 5 high-intensity focused ultrasound (US), 6 laser interstitial thermotherapy, 7 microwave thermotherapy, 8 and chemoablation. 9
Clinically, cryoablation and RFA are the two modalities currently used in the treatment of small renal masses and are considered as an option in selected cases in current clinical guidelines. 10
First described by Uchida et al 11 in 1995, cryoablation represents the most applied and studied of all ablative modalities. 12 It derives its tumoricidal effects from intracellular ice formation and delayed microcirculatory failure and is currently performed by one of two main minimally invasive approaches: laparoscopic and percutaneous. 13
The initial feasibility of RFA for the treatment of renal tumors was reported by Zlotta et al 14 in 1997 in three patients undergoing surgical resection after ablation. Since then, several case series of percutaneous RFA have been published, but with much greater variation in patient selection, technique, and follow-up. RFA uses alternating current to heat tissue to cause cell death and ischemia, with eventual coagulative necrosis. Although RFA has been applied using open, laparoscopic, and percutaneous techniques with US, CT, and MRI guidance, a meta-analysis of the current literature found that approximately 94% of patients undergoing renal RFA are treated with a percutaneous approach. 15
The aim of this study was to review recent advances and to provide future perspectives in renal focal therapy.
Basic Principles
Cryotherapy
Current cryoablation manufacturers for renal applications use argon gas to cause rapid freezing at the probe tip, based on the Joule–Thomson effect: argon gas passes through the cryoablation needle, and the tip of the needle is cooled, forming an ice ball. 16 Ablation can be monitored by a thermocouple or by US to confirm appropriate extension of the ice ball. In clinical practice, tissues are generally cooled to −40°C and the ice ball is propagated 1 cm beyond the target lesion. 14 Tumor destruction occurs through rapid freeze–thaw cycles, and two freeze–thaw cycles appear to achieve the best tissue ablation. 17 Cell death results from protein denaturation and extracellular ice formation during freezing, which disrupts cell membranes and causes movement of intracellular water, with subsequent alterations in cellular pH. Cell death may continue as a result of delayed tissue necrosis from thermal injury to local microvasculature. 16,18
Radiofrequency ablation
The goal of RFA is to destroy tissue by heat using RF energy. The procedure involves delivering an alternating electrical current at high frequency causing agitation of ions, which in turn results in heat. It has been shown that heating tissue to 55–60°C for 5 minutes results in irreversible cellular damage, and heating to more than 70°C causes cell death and tissue coagulation. 19 Temperature-based RFA machines use temperatures as high as 105°C during treatment.
Originally, RF energy was applied only as “dry” RFA by an electrode causing rapid increase in temperature resulting in tissue desiccation and necrosis. 20 However, this technique increases tissue impedance (resistance to energy flow), thus limiting the created size of the lesion. “Wet” RFA (interstitial saline infused) was developed to improve electrical conductivity through tissue creating a larger ablation zone. 21
Monopolar RFA devices available for ablation of renal tumors vary in the way energy delivery is monitored and controlled. Mainly there are temperature or electrical impedance (resistance)-based RFA generators. Various probes are available for RFA such as multitine probes and single probe. All RFA devices consist of a generator, an applicator (electrode), and dispersive electrodes.
Current Approach
Cryotherapy
Laparoscopic renal cryoablation allows precise cryoprobe positioning and monitoring of the evolving ice ball under real-time ultrasonic and visual control. Percutaneous approach is appealing when the targeted mass is accessible away from bowel and vital organs such as pancreas, gall bladder, or great vessels. General anesthesia and overnight hospital stay are required after the laparoscopic approach, whereas conscious sedation with local anesthesia is mostly used when cryoablation is performed percutaneously, allowing the procedure to be as outpatient setting.
Radiofrequency ablation
Laparoscopic RFA has the advantage of mobilization of the tumor and avoidance of adjacent organ damage, whereas percutaneous RFA is well tolerated and can be performed under sedation on an outpatient basis. The size of the ablated tissue depends on tissue impedance, ablation time, amount of energy delivered, and surface area of the electrodes. RFA probes can be inserted under US, CT, and MRI guidance.
Outcome of Thermal Ablation
Overall, majority of studies evaluating outcomes after renal tumor ablation consist of single-institution reports with relatively limited patient numbers and short-term follow-up. Therefore, it remains difficult to compare focal renal ablation to partial nephrectomy, for which reported series comprise considerably larger numbers of patients and longer follow-up.
Recently, two series have matured to provide 5-year follow-up data on renal cryoablation. Hegarty et al 22 reported on 66 patients (mean tumor size was 2.3 cm) having ≥5 years follow-up since laparoscopic renal cryoablation. Five-year overall survival was 81% and cancer-specific survival was 98%.
Another series with up to a 5-year follow-up included 48 patients (median lesion size was 2.6 cm), each of which had a ≥3-year follow-up. 23 Twenty-four patients had open cryoablation and the other 24 were treated laparoscopically. Overall survival rate was 89.5% and cancer-specific survival rate was 100%.
The longest follow-up available for biopsy-proven RCC treated with percutaneous RFA was reported by McDougal et al. 24 A small sample of 16 patients with a total of 20 tumors were treated. There was a reduction in the ablation defect with sequential imaging, approaching 92% at 4 years.
In a cryoablation/RFA comparison study, Hegarty et al 25 retrospectively reviewed the Cleveland Clinic experience with laparoscopic cryoablation (179 renal lesions) versus RFA (81 tumors) and noted radiographic evidence of disease persistence in 1.8% of lesions after cryoablation versus 11.1% of lesions after RFA.
A similar outcome was found in a recent meta-analysis of the available literature comparing RFA with cryoablation. 15 Forty-six studies from 44 institutions including 1234 localized renal lesions, treated with either open, laparoscopic, or percutaneous cryoablation or RFA, were analyzed. Repeat ablation was performed more often after RFA (8.5%) than cryoablation (1.3%).
Complications
Overall, cryoablation is well tolerated. Its most common sequelae are self-limited pain and parasthesia at the sites of probe insertion. 12 Other rare complications include hemorrhage, infection, visceral injury, pneumothorax, and delayed ureteropelvic junction obstruction. 26
In a multi-institutional study evaluating complications after 139 cryoablation procedures, 2 major and 18 minor complications were reported. 27 The only major complication in the laparoscopic group was open conversion during a procedure because of inability to access the tumor. Urinary fistulae due to collecting-system injury after renal cryoablation are rare.
Among 179 renal tumors treated at Cleveland Clinic by using laparoscopic cryoablation, 11 complications were observed. 25 Three major complications included hemothorax, congestive heart failure, and myocardial infarction.
Similar to cryoablation, RFA is generally well tolerated. The aforementioned multi-institutional review showed major and minor complications associated with RFA to be 2.2% and 6%, respectively. 27 Potential serious renal complications associated with RFA are urinoma and a proximal ureteral stricture. 21
Lastly, few studies to date examined the effects of thermal ablation on renal function. Cryotherapy and RFA seem to have a minimal effect on renal function. 12,21
Recent Advances
In the effort of improving the outcome and reducing the morbidity associated with probe-ablative procedures, major recent advances have been made toward three main directions: more accurate probe positioning, increased energy delivery, and reduced treatment-related morbidity (Table 1).
NOTES = natural orifice translumenal endoscopic surgery; RVS = real-time virtual ultrasonography; SPARC = single-port access renal cryoablation.
Improving probe placement
Real-time virtual ultrasonography
Reliable real-time image guidance is necessary for probe placement, monitoring the extent of the ablative lesion, and evaluation of operative outcome. Although US may have the ability to monitor real-time probe placement and formation of cryolesion, the quality of image is not optimal and sometimes shadowed with ribcage or cryoprobe itself. As such, a reliable real-time imaging modality remains to be found.
Real-Time Virtual Ultrasonography™ (RVS™; Hitachi Medical Corporation, Tokyo, Japan) represents a new technology allowing the fusion of real-time US and preoperative CT data. RVS displays the synchronized pictures of both real-time US and preoperative CT of the same section of the body, displayed on a split screen simultaneously. 28 Thus, the most important advantage of the RVS is its presentation of enhanced high-resolution CT side by side with a real-time US image.
Ukimura et al 29 evaluated the usefulness of percutaneous RFA under RVS guidance for RCC, with the aim of assessing whether RVS could achieve precise needle placement and thus potentially reduce radiation exposure compared with conventional CT-guided needle placement. Ten patients with 13 RCCs were all treated in one session. There were no significant complications, and none of the patients had a local tumor recurrence during the follow-up.
More recently, Haber et al 30 investigated the accuracy of percutaneous cryoablation for kidney tumors performed under combined real-time US and three-dimensional (3D) CT scan navigation with the RVS imaging system in a porcine model (Fig. 1). Eleven pigs were divided into an acute group (n = 3) and a chronic group (n = 8). After percutaneously injecting two tumor mimic lesions into each kidney, a CT scan was performed and digital data were saved into a navigation system (RVS) that allows 3D reconstruction and synchronization with real-time US images. The cryoprobe was guided percutaneously into the kidney tumor mimic and ice ball formation was monitored continuously during cryoablation using the RVS system. Kidneys were harvested and sent for macroscopic and histopathologic analysis at day 0 in the acute group, and at days 15 and 30 in the chronic group. Thirty-five renal tumor mimics (mean tumor size 2 cm) were created and treated by percutaneous cryotherapy. Synchronization between the CT scan 3D reconstructed images and real-time US was achieved in all cases. Three (8.5%) positive margins were found.

Percutaneous cryoablation for kidney tumors performed under combined real-time ultrasound and three-dimensional CT scan navigation with the real-time virtual ultrasonography imaging system in a porcine model. Note the split screen displaying the real-time ultrasound image beside the preoperative CT scan image (adapted from Haber et al 30 ).
Stereotactic surgical navigation
Percutaneous image-guided tumor ablation is likely to have a prominent role in the minimally invasive treatment of renal tumors as precise cryoprobe placement is essential for a favorable outcome. CT-Nav™ (Koelis, La Tronche, France) is a novel stereotactic surgical navigation system allowing precise percutaneous cryoprobe placement while reducing radiation exposure compared with conventional CT-guided procedures (Fig. 2). A prospective pilot study was performed to evaluate the technical feasibility, safety, and accuracy of the CT-Nav system during renal cryoablation. 31 Patients with enhancing renal masses amenable to renal cryoablation underwent preoperative CT scan with a preplaced tracking sensor taped to the body of the patient. Using a stereoscopic infrared camera, the tracking sensor was located three dimensionally and a tracking handle was used to guide the cryoprobe percutaneously based on the preoperative preloaded CT scan. Immediately after cryoprobe placement, a CT scan was repeated to confirm placement accuracy. A total of 13 tumors (mean size 2.2 cm) in 10 patients underwent cryoablation using the novel navigational system. Mean operative time was 155 minutes. No intraoperative or postoperative complications were noted. Mean length of stay was 9.5 hours. Mean targeting registration error was 4.2 mm.
Percutaneous cryoprobe placement under stereotactic surgical navigation guidance with CT-Nav (Koelis). Note that the probe guide is tracked by infrared sensors to synchronize the probe position with preloaded CT scan of the patient.
Electromagnetic technology
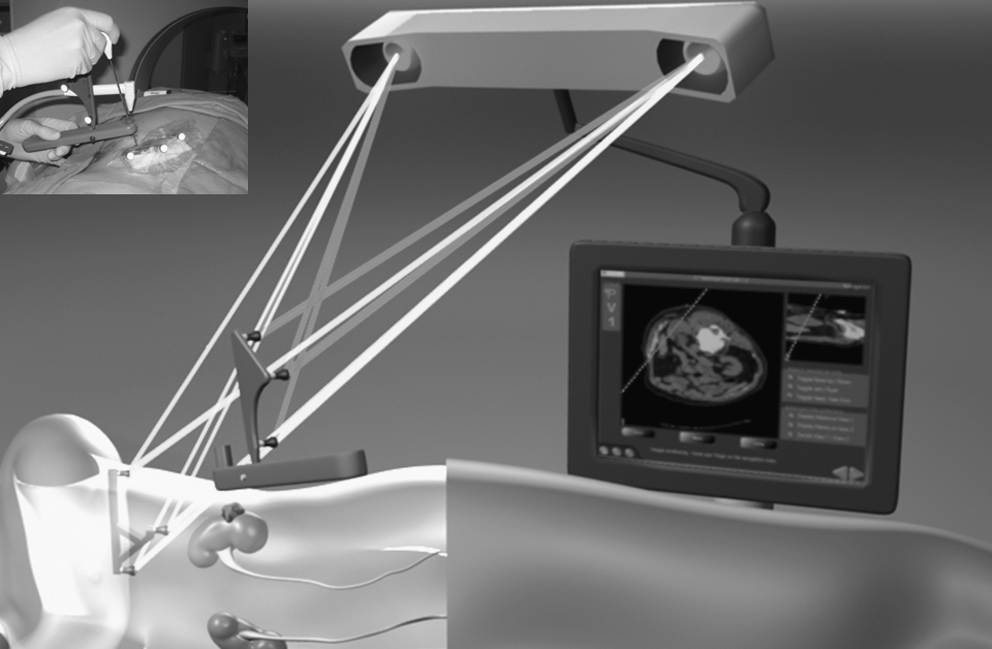
This new technology allows clinicians to utilize moving images to navigate instruments within organs including the lungs, liver, and kidneys. The Veran IG4 Delivery System™ (Veran Medical, St. Louis, MO) has four-dimensional capabilities allowing the system to capture and display 3D images that were gathered at various moments in time (the fourth dimension) along natural movement cycles (respiration and heartbeat) (Fig. 3). The Veran IG4 system allows for critical instrument “tracking,” which translated into the possibility of accurately targeting the lesion within a moving organ. The system enables clinicians to display rich and varied diagnostic information such as contrast-enhanced CT (or CT/positron emission tomography) at the point of care and therapy delivery.
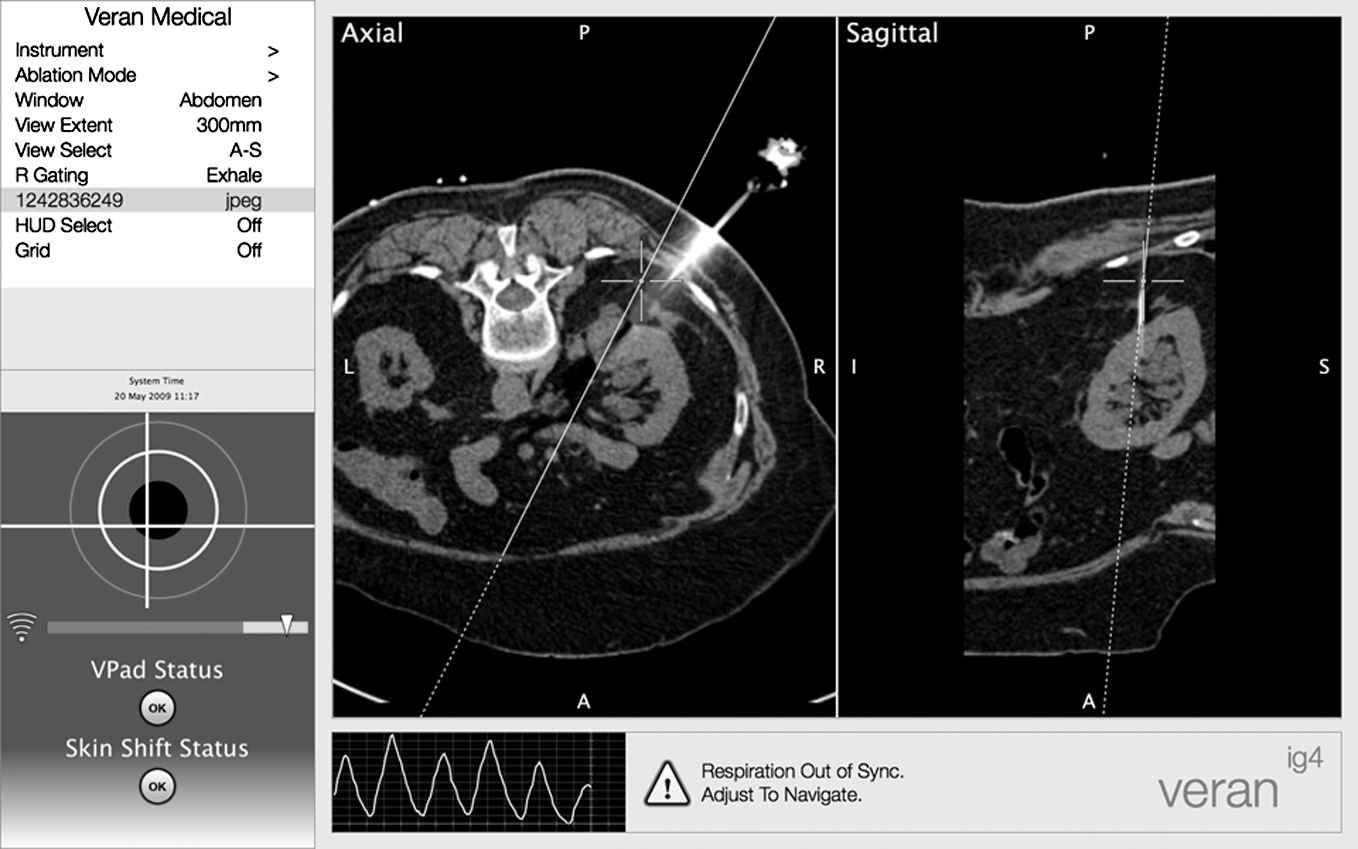
Four-dimensional volumetric navigation with Veran IG4 Delivery System (Veran Medical). Note the CT scan image showing the dotted lines that represent the suggested probe tract needed for optimal probe placement. Respiratory movement can be corrected automatically by the system.
Maximizing ablation efficacy
Third-generation cryotechnology
Cryomachines and cryoprobes evolved significantly over the past decade. The third-generation cryotechnology using argon/helium gas circulation and ultrathin 17-gauge needles has improved the procedure with nontraumatic penetration of the renal capsule and precise insertion of the cryoprobes into the tumor. 21 It also allows placement of multiple small probes into the tumor, minimizing blood loss when the probes are removed.
Recently, Laguna et al 32 have collected a multi-institutional European experience with 144 patients treated with ultrathin probes. Using strict criteria shows a 15% complication rate, of which 50% were relatively minor complications (not requiring surgical, endoscopic, or radiographic intervention).
Cool-tip RFA
Newer generators provide “high-energy” ablation, with power levels up to 200 W. 33 Increased energy delivery results in larger ablation zones. A method of limiting heat build-up at the electrode surface was also introduced through cooling of the electrode by circulating cooled water through an internal lumen, as in the CoolTip™ RF system (Valleylab, Bulder, CO). This system is based on a high-energy delivery through a cluster of thin probes of different lengths allowing the treatment of larger lesions in a shorter period of time under monitoring of the tissue impedance and self-adjusting of energy output. This is translated into optimization of energy delivery and minimal damage to surrounding structures.
Microwave ablation
Microwave ablation (MWA) involves the insertion of flexible antennae placed directly into target tissue, which channel microwave energy to create a rapidly alternating electromagnetic field, ultimately resulting in coagulative necrosis. Liang et al 34 recently evaluated the feasibility, safety, and efficacy of US-guided percutaneous MWA for small (<4.0 cm) RCCs. A total of 12 patients underwent US-guided percutaneous MWA. All tumors were ablated in one session, and there were no reported complications. No residual tumor recurrence was observed at a median follow-up of 11 months (range: 4–20 months). The researchers claim potential advantages of MWA, which include a broad zone of active heating and the fact that its transmission through tissue is not limited by desiccation and charring.
Minimizing surgical morbidity
Single-port access renal cryoablation
In an attempt to decrease number of laparoscopic ports used, we recently reported our initial experience with single-port laparoscopic approach. 35 Patients with localized small renal mass (<3 cm) ineligible for partial or radical nephrectomy were included. A multichannel single port was positioned in the umbilicus during the transperitoneal approach and at the tip of the 12th rib during the retroperitoneal approach. A 5-mm, zero-degree lens laparoscope with a flexible, steerable tip is used (Olympus Surgical, Orangeburg, NY). Intraoperative biopsy was performed and a 3.8-mm cryoprobe (Endocare, Inc., Irvine, CA) was inserted under US guidance through one of the multichannel working ports (Fig. 4). Two freeze–thaw cryoablation cycles were performed.
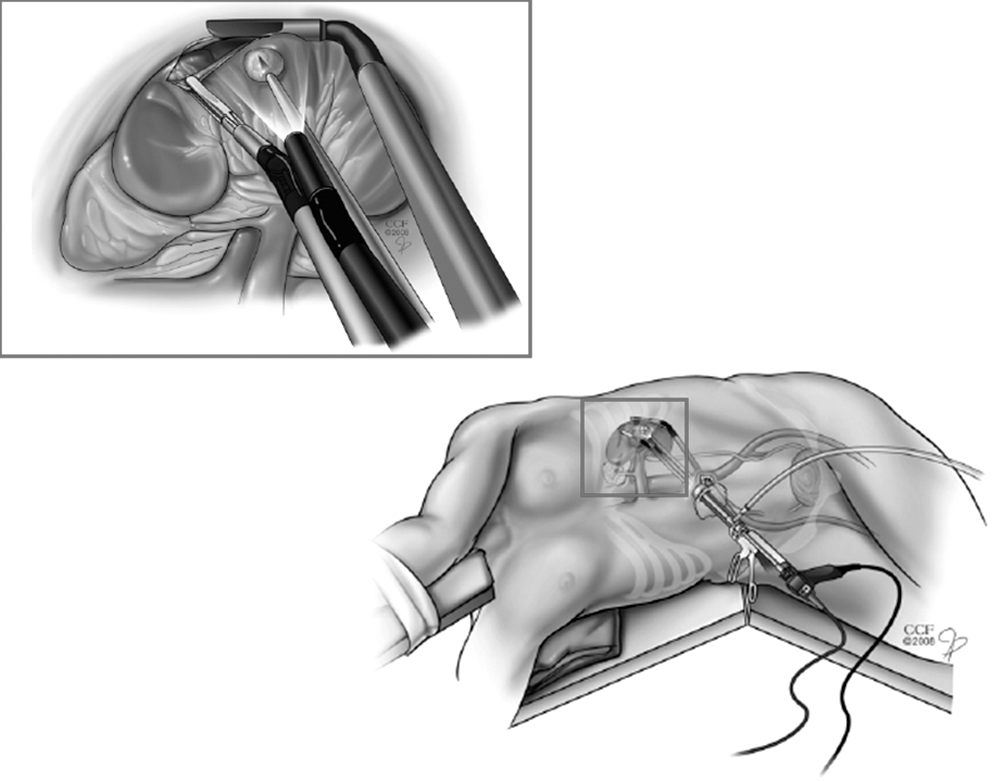
Single-port access renal cryoablation (adapted from Goel and Kaouk 35 ). Note that all laparoscopic instruments are inserted through a single port in the umbilicus.
All six cases (mean tumor size 2.6), four retroperitoneal and two transperitoneal, underwent single-port access renal cryoablation (SPARC) without conversion to laparoscopy or open surgery. No intraoperative complications were noted and mean hospital stay was 2.3 days. CT with contrast documented no residual tumor enhancement in three cases. Our early experience demonstrates that SPARC is feasible and safe, allowing a virtually scarless surgical procedure. However, some pitfalls related to single-port surgery need to be recognized and further addressed. With parallel insertion of laparoscopic instruments, the range of motion is limited and instruments frequently clash. Second-generation laparoscopic instruments are needed to obtain better ergonomics and instrument maneuverability.
Radiosurgery
In contrast to the thermal ablation techniques, radiation destroys dividing tumor cells by mitosis-linked apoptosis. At higher doses, it results in complete ablation of tissue and thus provides the basis for solid mass ablation. By dividing the radiation dose into multiple separate individual beams, radiosurgical technology can deliver high-focal doses of radiation necessary to ablate a lesion completely, without increasing collateral damage.
One of the major limitations to extracorporeal solid organ ablation of renal tumors is the inherent back-and-forth movement of the kidney associated with the respiratory cycle. This limitation can be circumvented by a highly advanced radiosurgical image guidance system so that the beam remains aligned with its target. With the aid of this technology, renal tumor motion can be tracked in 3D space, allowing for exceptionally precise treatment (within 0.3 mm).
Ponsky et al 36 reported three patients with a mean tumor size of 2 cm, candidates for surgical treatment who underwent radiosurgery followed by a partial nephrectomy after 8 weeks. The patients received a total of 16 Gy in four fractions delivered over 2 days. At 8 weeks after radiosurgical treatment, a preoperative CT scan was obtained, and patients underwent the surgery. Mean follow-up was 56 weeks. No acute toxicities and no changes in renal function were noted. The initial two patients had histologically demonstrated viable tumor remnants. No viable tumor was seen in the last patient.
Promising work with radiosurgical technology has also been reported more recently by Hong et al. 37 They assessed 14 patients with a mean tumor diameter of 4.1 cm treated with 21 Gy, divided into three fractions. Patients were then imaged every 3 months with serial CT scans. Tumor volume decreased by a mean of 44% without signs of disease progression at 12 months of follow-up.
Future Developments
Natural orifice translumenal endoscopic surgery
Natural orifice translumenal endoscopic surgery (NOTES) is an emerging technique with significant experimental and clinical ongoing investigation. 38 We recently presented our experience with transgastric and transvaginal NOTES renal cryoablation in a porcine model, as an alternative to the laparoscopic approach, for anteriorly located renal tumors not accessible percutaneously. 39 In two female farm pigs, we performed four procedures of NOTES renal cryoablation. For the transgastric approach, a dual-channel video gastroscope (Olympus, Tokyo, Japan) was used, the stomach wall was punctured using a needle-knife, a guidewire was passed into the abdominal cavity, and the access dilated using a controlled radial expansion balloon. The bowel was mobilized medially and the Gerota's fascia overlying the upper pole was dissected. For the transvaginal approach the gastroscope was introduced through the posterior fornix of the vagina. After gaining intraperitoneal access and complete dissection of the kidney upper pole, the Veress needle was removed and replaced by a 2.4-mm cryoprobe, which was inserted at the same skin puncture site of the Veress needle under direct gastroscopic control. Pneumoperitoneum was maintained by continuous insufflation through the gastroscope. Two freezing cycles were performed and the ice ball formation and advancement were monitored gastroscopically. All four procedures were performed with no intraoperative complications. No additional laparoscopic ports or open conversions were necessary. Mean operative time was 83 minutes. Stomach closure was tested watertight, and there were no abdominal or pelvic injuries found at autopsy. The authors concluded that NOTES can provide adequate minimal surgical dissection for safe and effective percutaneous renal cryoablation under direct videoscopic monitoring at kidney locations otherwise not accessible percutaneously. This approach can be used for renal cryoablation providing a scarless surgery. Limitations were represented by the lack of suitable instrumentation to use through the gastroscope and surgeon's training to navigate flexible endoscopic instruments. A specific NOTES cryoprobe that might be inserted through the gastroscope working channel or alongside the gastroscope needs to be developed to be able to perform a pure NOTES cryoablation by introducing the cryoprobe through the endoscope. Moreover, a NOTES robotic platform coupled with a surgical navigation system will represent a step forward in this field.
Robotics
The use of robotics in various urological procedures has been increasing rapidly in recent years. Investigators from the Johns Hopkins developed robots for obtaining percutaneous access to the kidney (PAKY). 40 The first robot had an active manipulator and a motorized arm driving the access needle. In live animal experiments, however, it had a low accuracy rate. To reduce cost and complexity, a second robot PAKY was developed with a passive manipulator and an active injector system. This system mimics the standard surgical technique applied in the operating room using a C-arm. A passive arm with seven degrees of freedom is mounted to the operating room table. The C-arm and needle are aligned fluoroscopically over the target calix, highlighted by injecting air through a ureteral stent. The PAKY system does not require computer-based image processing for image correction and calibration. This system is currently being evaluated clinically.
Combination therapy
Combination of chemotherapy and probe thermal ablation may improve efficacy of local renal tumor destruction. A synergistic response has been reported in a renal-cell model, suggesting that 5-FU chemotherapy may be more effective when followed by cryosurgery. 41 In the clinical setting, synergistic activity of cryoablation and cyclophosphamide is currently being evaluated on advanced epithelial tumors (NCI Trial protocol NCT00499733).
Conclusions
Effective treatment of incidentally detected small renal masses continues to evolve. Probe-ablative therapy provides an attractive nephron-sparing treatment. Cryotechnology is rapidly developing and cryosurgery can offer the advantage of combining a nephron-sparing surgery together with a minimally invasive approach. Technical refinements will carry emerging clinical data available for RFA. SPARC has been shown to be feasible and safe. Although in its infancy, NOTES might represent a further step toward scarless surgery. Radiosurgery is under investigation and oncological outcomes are awaited to determine its role. Stereotactic surgical navigation and robotic needle placement would facilitate and increase the accuracy of percutaneous probe placement while reducing radiation exposure compared with standard CT guidance.
Footnotes
Disclosure Statement
Jihad H. Kaouk, M.D., is a speaker for Endocare and a proctor for Intuitive Surgical. No competing financial interests exist for the other authors.