
Abstract
Purpose:
We investigated urinary bladder stone, surgical tools, and procedures in urologic sections of textbooks of Abul-Qasim Khalaf Ibn Abbas Alzahrawi (Albucasis) and Serefeddin Sabuncuoglu. In addition, we compared the relation of their textbooks with urologic surgery.
Materials and Methods:
Al-Tasreef Liman Aajaz Aan Al-Taaleef (Al-Tasreef), a surgery textbook written by Alzahrawi (who lived in Endulus between 930 and 1013) and Cerrahiyyetu'l-Haniyye, written by Sabuncuoglu (who lived in Turkey between 1385 and 1470) were evaluated with regard to urinary bladder stone and surgical instruments.
Results:
The textbooks give information about urinary bladder stones. They include definitions of diseases, etiologies, and surgical techniques, and describe surgical tools. Cerrahiyyetu'l Haniyye is a colorful miniaturized textbook.
Conclusion:
The urinary bladder stone section in Cerrahiyyetu'l Haniyye is the translation of Al-Tasreef with some additional information and illustrations. Surgical tools and procedures described by the two physicians have reached to our century. Tools and procedures invented by Alzahrawi come to the present day in similar or developed styles.
Introduction
Abul-Qasim Khalaf Ibn Abbas Alzahrawi (930–1013 AD) was a famous surgeon in the 10th century, known as Albucasis. He lived in Andalusia, mostly in Cordova, a city with 50 hospitals. In the 10th century, the term barber-surgeon was given to surgeons in other countries, while medico-surgeon was used in Andalusia. 3 Alzahrawi's textbook Al-Tasreef Liman Aajaz Aan Al-Taaleef (Al-Tasreef) was the largest first surgical book. 4 Alzahrawi's modifications and innovations were widely used in Europe until the beginning of the 18th century, which saw the start of the modern method using the suprapubic instead of the perineal approach for the removal of bladder stones. In addition, he was the first to describe, in detail, the operative technique in women and to recommend the two-stage operation in complicated cases. He was the founder of lithotripsy and invented some instruments to crush and drill the stones.
Volume 30 of Al-Tasreef is devoted to surgery and operative intervention and is a landmark in the history of surgery, being the first to describe and illustrate rational and complete surgical instruments. 5 This textbook was translated into Latin, for example, by Gerard de Crémone in the 13th century and was titled Chirurgia. The Latin translations of major Arabian texts largely contributed to the rise of medical sciences in the Christian Western world during the Middle Ages. 6
Serefeddin Sabuncuoglu (1385–1468), a famous Turkish physician, lived in Amasya. He practiced medicine at Amasya Hospital, one of nine large hospitals in the Ottoman Empire. This hospital functioned until the beginning of the 19th century. He experimented with animals and also with his own body. 7 He used the Turkish language well and wrote several important books on medicine: A book on experimental medicine (Mucerreb-name [The Book of Experiences]) and a book on surgery (Cerrahiyyetu'l-Haniyye [Imperial Surgery]). He translated Al-Tasreef into Turkish, added some information, and named it Cerrahiyyetu'l-Haniyye. Cerrahiyyetu'l-Haniyye, written in 1465, has been reviewed by various authors and is the first color illustrated surgical textbook in the Turkish-Islamic literature. It contains Sabuncuoglu's color miniatures of operative procedures. 7,8 Old references did not mention Sabuncuoglu, because his textbook had been written in Ottoman-Turkish. In these ancient centuries, the scientific books had been written traditionally in the Arabic or Persian languages.
Ruscuklu Hakki was the first scientist to give information about Sabuncuoglu in 1920. In 1923, he was noted in the textbook of Bursali Tahir Ottoman Authors. In 1925, Osman Sevki mentioned him in his book Ottoman Medical History. 9 One of the most important inventions of Alzahrawi, which preserves its currency in our century, is the extraction and crushing of urinary bladder stone. 5 This innovation was important to the development of bladder stone surgery, because it significantly decreased the death rates previously caused by earlier attempts at this operation. 1
In our research, we investigated urinary bladder stone, surgical tools, and procedures in urologic sections of the textbooks of Alzahrawi and Sabuncuoglu.
Materials and Methods
Al-Tasreef, the surgery textbook by Alzahrawi, and Cerrahiyyetu'l-Haniyye, written by Sabuncuoglu, were evaluated with regard to urinary bladder stone and surgical instruments.
Al-Tasreef
This medical encyclopedia is composed of 30 separate volumes, and every volume consists of several chapters. There are a lot of handwritten copies of Al-Tasreef in the world. We examined the handwritten Arabic copy of Al-Tasreef in the Bashir Agha Collection. 5,10 We accessed it from the Sulaymaneyya Library in Istanbul.
Cerrahiyyetu'l-Haniyye
We examined the handwritten Ottoman-Turkish copy of Cerrahiyyetu'l-Haniyye in the department of medical history of the Istanbul University Medical School in Istanbul and the revised copy of this book written by Uzel in 1992. 7 Cerrahiyyetu'l-Haniyye has only three original handwritten copies: One in the Bibliotheque National in Paris and the other two in the Fatih Millet Library and the department of medical history of the Istanbul University Medical School in Istanbul. Two copies of the book were originally written by him and one copy was written later in the 18th century.
Our illustrations were taken from original textbooks for each author.
Results
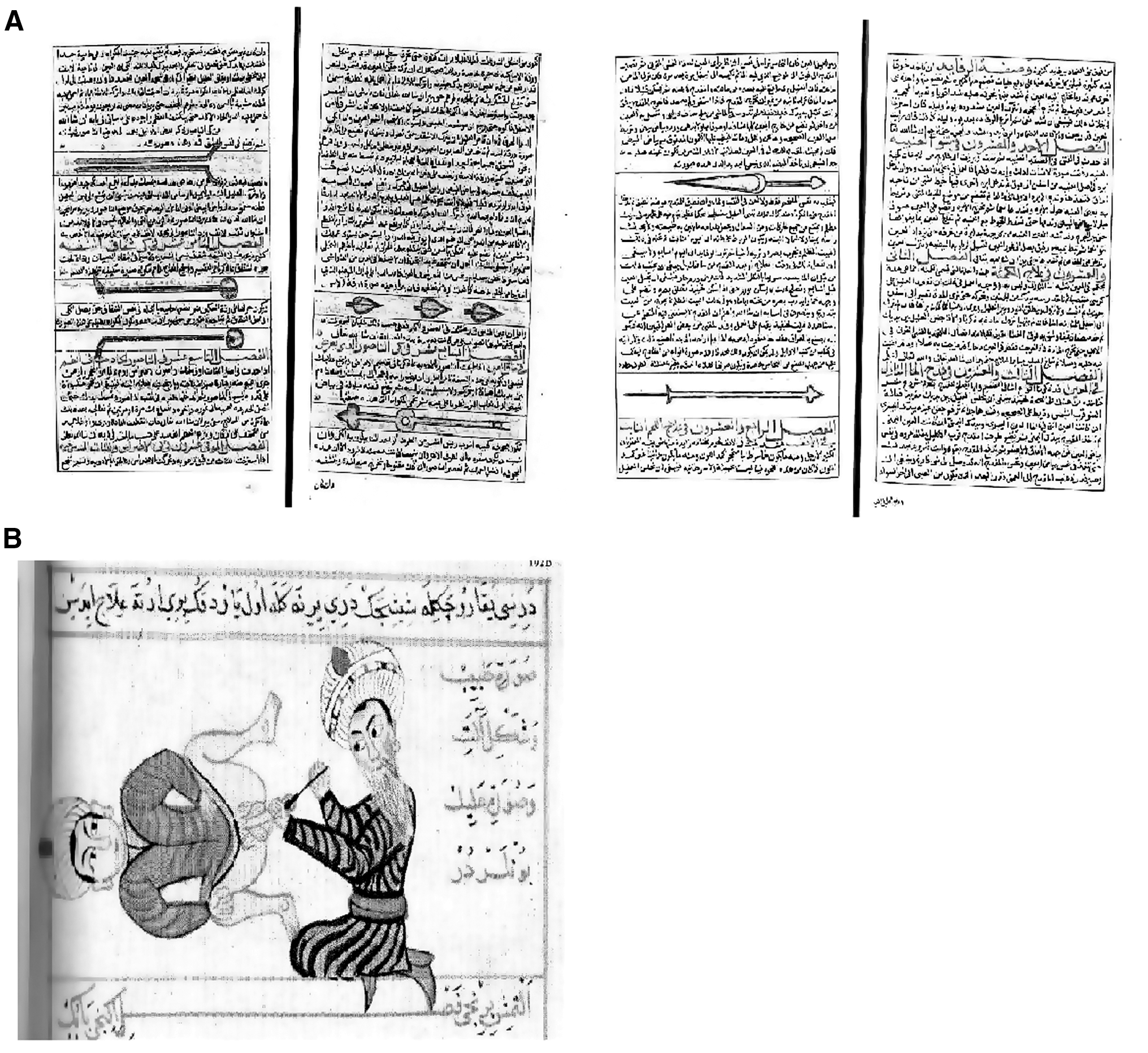
Kasatir, zerraka, and mihkan, described by Alzahrawi and Sabuncuoglu, are used as catheter, injector with piston, and evacuator, respectively, for the same purpose in urologic procedures as in the present day, although there are some differences (Figs. 1 and 2).
(
(
Instruments used by Alzahrawi and Sabuncuoglu for urinary bladder stone diseases
Kasatir. This is a very fine silver tube with a goblet-shaped appendix at its end. It includes a doubled-fiber, which contains a piece of cotton or wool at its tip like a plug, and takes urine out of the bladder. He introduces the catheter into the urethra, first downward, then upward in the direction up to the urinary bladder. When the catheter reaches the bladder, he pulls the fiber back, then urine comes out. This process is repeated until the bladder is empty. 11
Sabuncuoglu clarified that the reason for “the residue urine in urinary bladder” was stone, blood clot, inflammation, or polyp. First, the patient is shaken. If this method is not enough, the physician must use the catheter known as kasatir. Procedures are the same as that in Al-Tasreef. 7
Zerraka. Liquid medicaments can be given by this injector through the urethra to the bladder. This method is used for the treatment of polyp, blood clot, or inflammation. The diameter of the injector, made of silver or ivory, is suitable for the dimension of the urethra. It has a piston on the back, and its pin on the front has three holes. The piston pushes the liquid material, and it reaches through these orifices to the bladder. 11
Sabuncuoglu explained that the zerraka was used for the same purpose. He gives the same information about its three holes. The piston is located into the zucchini, which is empty and has a hole in the middle. 7
Mihkan. This is for instillation of the urinary bladder. A coverall like a balloon functions as a piston. A ram bladder is taken and filled with liquid medicament. It is tied to the pin of the injector that has a groove for a string. After that, this sac can be filled with a liquid. 11
Sabuncuoglu had similar information; it is made of silver and has orifices on its tip. It is passed through the urethra to the bladder. A lamb bladder was tied to the tip, and the medicament could be given by forcing strongly. 7
They give information about many varieties of stones, such as small or large, smooth, rough, or branched, and emphasize the importance of operative technique according to the type of stone.
Alzahrawi's description of the extraction of urinary bladder stones
“In the beginning of the treatment of bladder stone, an enema is necessary for the patient to clear out his bowel because the stools may prevent to search and locating the stone. Then the patient should be held by his legs and shaken downwards to bring the stone down to the bladder neck or, he could jump from a height several times. Seat him upright facing you with his hands beneath his thighs to make the whole bladder tilted downwards. Then search for the stone by palpating him externally. If you feel the stone in the lumen, cut upon it right away. But if the stones don't come at all under your finger, insert finger, by lubricating with oil, into his anus and search out for the stone when it comes under your finger move it, little by little, to the bladder neck. Press upon it with your finger pushing it outwards to the place where you wish to make your incision. Request an assistant to squeeze the bladder with his hand. Another assistant should help to extend away the testicles with his right hand and with his other hand to stretch the skin beneath the testicles away from the place. Then take the Al-Nashl scalpel and incise the area between the anus and the testicles not in the mid-line but to the side of the left buttock. The incision is made directly on the stone itself while your finger in the anus is pressing it outwards. The incision is made oblique, and it should be just enough to allow the exit of the stone, not larger, as your finger in the anus leads to its extrusion without difficulty.”
Sabuncuoglu mentions the method of stone extraction from the urinary bladder in a manner similar to Alzahrawi. He emphasized that it is necessary to look through the anus to find the stone in the neck. After that, two assistants must help with the process.
Alzahrawi used the lateral approach in lithotomy procedures when the stones have angles and edges because of difficulty in extracting them: “Sometimes, you need to slightly extend the incision. If still the stone doesn't come out you should maneuver it either by holding it with a strong forceps, or introducing underneath it a slender instrument with a curved end.”
He used Al-Kalbatain (pliers), similar to forceps, for the same purpose. Alzahrawi is the first physician who used forceps for the extraction of the stone (Fig. 3).

Al-Kalbatain from Alzahrawi (
Advice from Alzahrawi if there is still a problem with the extraction
“If you, still, cannot extract the stone, widen the incision a bit; and if some bleeding disturbs you, stop it with sulfiric acid. If more than one stone is encountered, first push the largest to the bladder neck, cut down upon it; and then push the small stone next. It is ignorance to use a very large incision, because the patient may die or suffer from permanent incontinence because of the insufficient wound heal. Try to manipulate the stone out or, maneuver breaking it with the Al-Kalbatain to deliver it out piecemeal.”
Sabuncuoglu also emphasized that it is necessary to crush the stone with Al-Kalbatain if a larger incision is not successful. The procedures are similar to Alzahrawi's.
Alzahrawi and Sabuncuoglu described the use of a drill to dissolve obstruction of the penile passage caused by a small stone and describe the types of drill. The drill was named Al-Mishaab by Alzahrawi, miskab by Sabuncuoglu (Fig. 4), respectively. “If the stone is small and moved to the penile passage, preventing the urine from coming out, take Al-Mishaab made of Foulaz (stainless steel) with a shape like this: Its end is triangular and sharp, and it is fixed to a wooden handle. Take a thread and tie it around the penis below the stone to prevent the stone return back to the bladder. Then gently introduce its iron end, revolve, little by little, upon the stone itself to make a hole and perforate to pass through the other side. Then, the urine will be immediately released. When you squeeze with your hand on the outside of the penis, remains of the stone will crumble and be passed out with urine.”

Al-Mishaab (drill) from Alzahrawi.
Alzahrawi and Sabuncuoglu said that incision was made on the penis to extract the stone if the drill was not successfully. “But, if this treatment was not feasible for you because of an impending obstacle, tie a thread below the stone and another above. Then cut down on the stone in the penis itself between the 2 ligatures and deliver the stone out.”
Al-Tasreef: urinary bladder stone extraction in women
“In women, the site for cutting on the stone is far away, from where the stone lies, so a very deep incision, which was dangerous, is required. You should take with you a competent midwife for looking after women or a woman knowledgeable about this art. Request her to follow all your instructions in, first of all, searching for the stone. If patient is virgin, she should insert the finger in her anus and feel for the stone. If she finds it and manages to trap it under her finger, then instruct her to cut down upon it. But, if she was not a virgin, instruct the midwife to introduce her finger in the patient's vagina and feel for the stone after she has placed her left hand on the bladder, applying a good amount of squeezing pressure. If she finds the stone, she should roll it away from the bladder until the stone is pushed down to the thigh. Then, she should cut down the vulva. And the incision is made small at first, if it is necessary she may extend the incision a little. You should know that some of the stones are small and some are large; smooth and rough, oblong rounded and branched. Different approaches are needed. If you are overcome by hemorrhage and you knew, from its pulses, that it is coming from an artery that has been severed, put the powder on the area, band it up with tight bandages and leave the stone, do not extract it since this may cause the death of the patient.” 5,10
Sabuncuoglu gives similar information that he received from Alzahrawi.
Discussion
Alzahrawi remarkably improved the technique of perineal incision for extraction of stones and reduced its risk (such as using lateral incision instead of median incision) when compared with the description of this technique given during the ancient Indian civilization (Charaka in the 1st century and Susrata in the 5th century) and during the Greek civilization in Aegean Sea Greece (Paulus Aegineta, 625–690 AD). There are studies that confirmed the originality of Alzahrawi who described operative steps and invented operative instruments not known in the Greco-Roman era. 5,6,12
Rhazi, Avicenna, and Alzahrawi were the most efficient physicians for Islamic and Western medicine. The period between Alzahrawi and Sabuncuoglu included many physicians, following the same methods. The most famous physicians were Ibn Cezle, Ibnu’-Baytar, Ibnu'n-Nefis, El-Bagdadi, Ed-Dahvar (12th century); En-Nahcuvani, El-Konevi (13th century); Hekim Bereket, Hacı Pasa (14th century); Mumin B. Mukbil, Ibn Serif, Ak Semseddin, Altuncuzade (15th century). 13 Hekim Ahi Celebi (16th century) also used the books of Alzahrawi and Sabuncuoglu. He included information about urinary stones, improved catheters, and crushing the stones in his book. 14
Some of the monks tried perineal incisions. German Emperor Heinrich II was cut by a Benedictine at Monte Cassino in 1022. There is a relief showing this. Romanis (1520) still used perineal lithotomy with a vertical incision. In Europe, most of the lithotomists, such as Italian Marianus Sanctus (16th century), the French Jack de Beaulieu (17th century), and the English William Cheselden (18th century) were using Alzahrawi's lateral approach, incising on the left side. 15
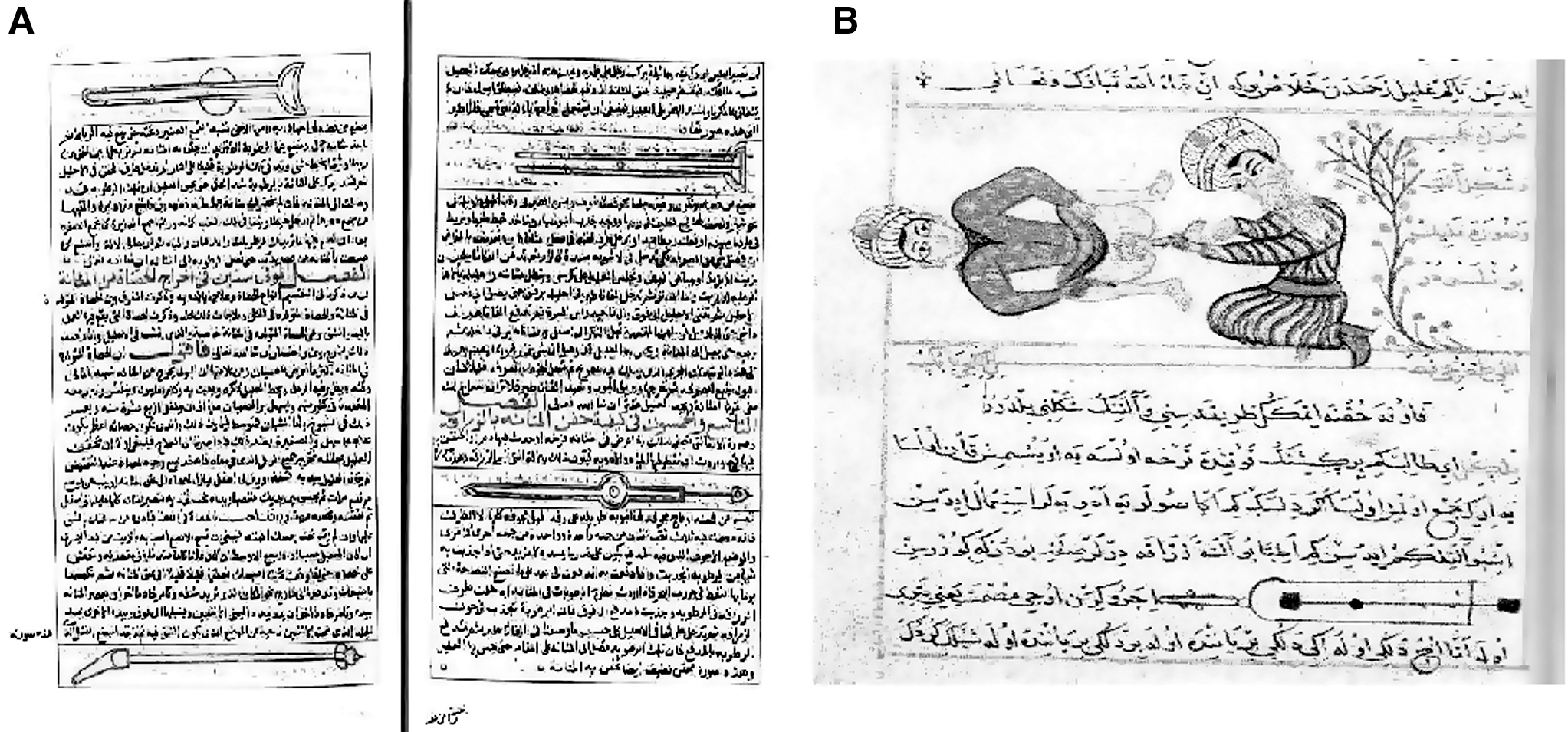
In addition, Alzahrawi provided a lot of information that was not known very well in the Western world. He emphasized that it was essential to prepare the patient with an enema in the preoperative period to locate the stones more easily. He classified the stones and revealed the difference between kidney and bladder stones. He mentioned that the stones were frequent in boys, and their treatment was easier. He described the operative techniques for boys, elderly persons, and women. He believed that it was necessary for a female surgeon to perform operations on women. Sabuncuoglu accepted this and illustrated these female surgeons and female patients in his book. In the Islamic world, the painting of human figures was disliked. Despite Islamic rules, he showed female surgeons, called Tabibe, in operations. 16 Alzahrawi and Sabuncuoglu emphasized the importance of postoperative wound treatment for amelioration.
Alzahrawi suggested a lithotomy position for surgical operations under the umbilicus level such as extraction of urinary bladder stone. Sabuncuoglu included some illustrations showing the lithotomy position. This position was used in the Western world after Alzahrawi. 3
It was thought that Cerrahiyyetu'l-Haniyye was a translation of Al-Tasreef. Despite some similarities, a careful analysis of these two treatises revealed that there are 137 different observations and recommendations in Sabuncuoglu's book. The most significant difference between the two books is that Al-Tasreef contains only drawings of surgical instruments, but Sabuncuoglu, for first time in the Turkish-Islamic medical literature, drew illustrations of patients being examined or operated on. 8 Vecihe Kilicoglu, however, said that these two textbooks were the same when the copy of Cerrahiyyetu'l-Haniyye in the Biblioteque National was compared with Al-Tasreef in the Ayasofya Library. 9 With a different idea, llter Uzel said that Cerrahiyetu'l Haniyye was not a simple translation. 7 He claimed that Sabuncuoglu translated 30 volumes of Al-Tasreef, and his book included different additional information and illustrations.
Each copy of Cerrahiyyetu'l-Haniyye differs from the others, and none is complete. The surgical atlas was rediscovered in 1936 by Suheyl Unver, a Turkish medical historian, and its illustrations were published in a separate book, although some parts are suspected to be missing. An in-depth review on these copies of the book was written by Uzel in 1992. 7,17,18
Alzahrawi's book was translated into many European languages, such as Latin, French, and English. Alzahrawi's influence is vividly seen in the practice of the Italian lithotomist Marianus Sanctus (16th century), the French Jack De Beaulieu (17th century), and the English William Cheselden (18th century). Alzahrawi introduced Al-Kalaleeb forceps to crush large bladder stones and Al-Mishaab to drill and fragment an impacted urethral stone. Andreas a Cruce (18th century) only added screw action to the Al-Kalaleeb lithotrite, but Amussat managed in 1822 to apply it transurethrally. Similarly, with the notion of transurethrally reaching the stone while within the bladder, Alzahrawi's idea of drilling by Al-Mishaab was the foundation of the litholepte of Fournier de Lempdes (1812), the instrument of Gruithusien (1813), Civiale's trilabe (1818), and the brise coque of Rigal De Galliac (1829). 5,15
Surgical tools and procedures invented by Alzahrawi come to the present day in similar or developed styles. Sabuncuoglu, one of the most influential surgeons of the early Ottoman era, was partly influenced by Alzahrawi. In the introduction to his surgical textbook Cerrahiyyetu'l-Haniyye, Sabuncuoglu refers to Alzahrawi as a master and mentor. 7,18 He is also the successor of Alzahrawi and protected the value of his illustrations to the present day.
Footnotes
Disclosure Statement
This work had no financial support.