
Abstract
Ureteritis cystica is a rare, but recognized cause of ureteral obstruction. To our knowledge, we present the first case where obstruction secondary to the cystic component is confirmed with a functional study. Additionally, we present high-quality radiologic and endoscopic images of two cases of ureteritis cystica.
Introduction
Ureteritis cystica is usually a silent lesion with no typical signs or symptoms. Flank pain or hematuria can be present, however. Flank pain or renal colic results from obstruction secondary to either ureteral calculi, strictures, long-standing infection, or the cystic lesions of ureteritis cystica themselves.
Although ureteritis cystica is often described as a recognized cause for upper tract obstruction because of the cystic component, this is based on numerous case reports and the finding of hydronephrosis intraoperatively, pathologically, or radiologically. In these reports, obstruction is inferred from the finding of hydronephrosis only, and functional investigations, such as diuretic renography and Whitaker testing, are lacking. To date, there have been no reported cases with accompanying functional investigations that demonstrate obstruction.
We present two cases of ureteritis cystica, including both the first endourologic images and the first case of obstructive ureteritis cystica secondary to the cystic component, proven with a functional investigation.
Case Reports
Case 1
A 64-year-old woman presented to the emergency department with left flank pain and hematuria. She had multiple medical comorbidities, including diabetes mellitus type 2, hypertension, obesity, a previous deep venous thrombosis, and an ischemic stroke. CT of the abdomen and pelvis showed severe left-sided hydronephrosis and a possible ureteral tumor (Fig. 1). A nephrostomy tube was inserted for acute management of the obstruction.

Case 1: Axial (
She subsequently underwent bilateral retrograde pyelography and ureteroscopy, under general anesthesia, for evaluation of the ureteral mass. Findings on the right retrograde pyelogram were normal. On the left, there were multiple spherical filling defects (Fig. 2A). Both semirigid and flexible ureteroscopy were performed to evaluate the complete length of the left ureter, renal pelvis, and calices under direct vision.
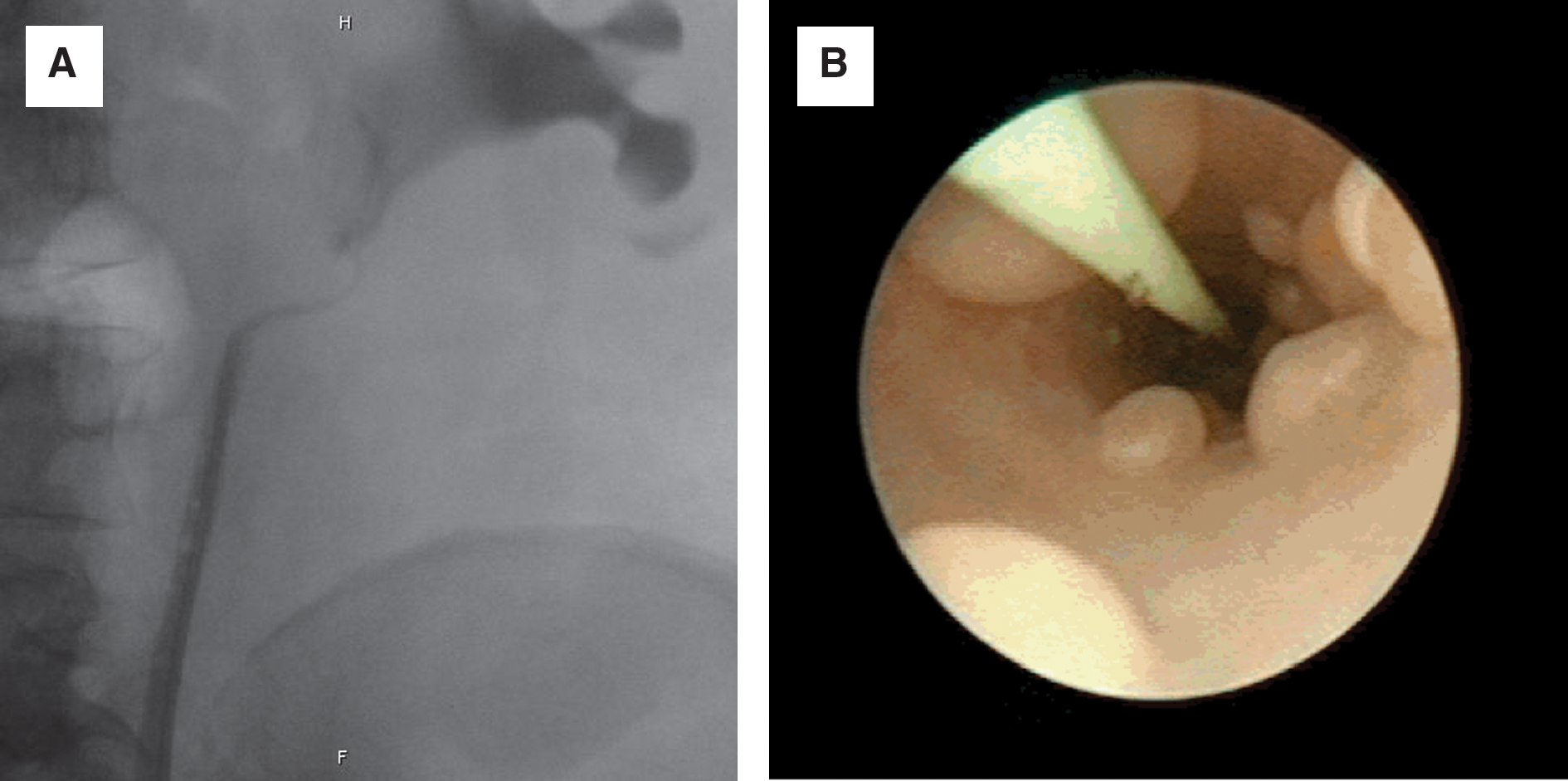
Case 1: (
Numerous cystic nodules consistent with ureteritis cystica were visualized within the wall of the left ureter (Fig. 2B). Involvement was most severe proximally, consistent with the point of obstruction as seen on the CT scan. The finding of a large number of cysts in the proximal third of the ureter is in keeping with previous reports that the number of cysts is greatest within the upper third of the ureter and decreases distally. 3 There was also evidence of cystic nodules within the renal pelvis, consistent with pyelitis cystica.
Left ureteral washings revealed benign atypia consistent with reactive transitional cells with no evidence of malignant cells. Abundant neutrophils were also seen.
The patient's condition was managed acutely with a nephrostomy tube, and the hydronephrosis resolved. After removal of the nephrostomy tube, repeated imaging revealed recurrence of severe hydronephrosis and a transition point in the upper ureter. There was no evidence of a crossing vessel. A diuretic renal scan demonstrated good drainage from the right, but a t1/2 of 110 minutes on the left indicated mechanical obstruction from the ureteritis cystica cysts. The patient refused a ureteral stent or further treatment at that time.
On follow-up 9 months later, the patient has had recurrent urinary tract infections, but her creatinine level has remained stable at 96 μmol/L.
Case 2
A 60-year-old woman presented with a history of recurrent left-sided pyelonephritis, flank pain, and microscopic hematuria. CT demonstrated a large conglomeration of stones within the lower pole of the left kidney. In addition, there was significant cystic degeneration and cortical scarring. More concerning, however, was a soft-tissue filling defect that was seen within the upper left ureter. Retrograde ureteropyelography was performed and demonstrated multiple filling defects (Fig. 3). Ureteroscopy again revealed characteristic lesions that were consistent with ureteritis cystica (Fig. 4). Ureteral biopsy was performed, but results were inconclusive.

Case 2: (
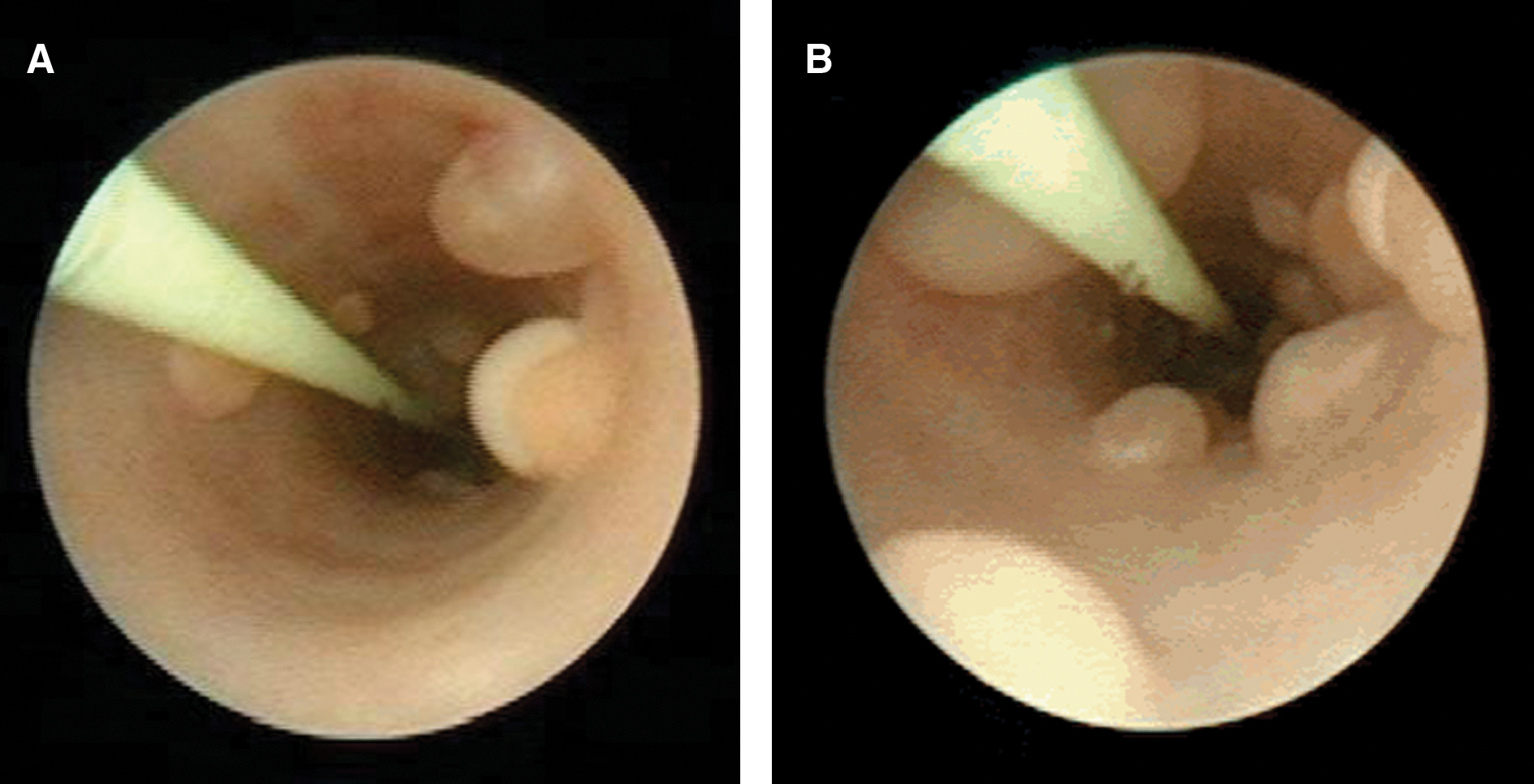
Case 2:
In this case, there was no functional obstruction of the left kidney and the left kidney contributed 34% of overall renal function. As is usually the situation, the cysts were not causing obstruction in this patient, and so no treatment of the ureteritis cystica was indicated. The stones in the lower pole were infected, however, and therefore were removed percutaneously.
A contrast imaging study was not performed in the follow-up period to reassess the ureteritis cystica, because the patient remained asymptomatic.
Footnotes
Disclosure Statement
No competing financial interests exist.