
Abstract
Purpose:
To evaluate the efficacy of transvesical obturator nerve block (ONB) in the prevention of obturator nerve reflex and leg jerking during transurethral resection of bladder tumors (TURBT).
Patients and Methods:
A total of 60 patients were studied, in whom the transurethral resection of tumors on the posterolateral bladder wall were performed under spinal anesthesia (SA). The patients were randomly divided into two groups. In the first group, we performed transvesical ONB and SA together, while the second group received only SA. The patients underwent TURBT using monopolar cautery. Incidence of leg jerking was registered and compared in these two groups. We used a nerve stimulator to detect the obturator nerve next to the lateral bladder wall. The obturator nerve was identified by its response to nerve stimulation. Then, 10 mL of 1% lidocaine was slowly injected through the working channel of a cystoscope.
Results:
In the intervention group, 34 ONBs (4 bilateral and 26 unilateral) were tried. We could not detect the obturator nerve by nerve stimulation in six patients, and lidocaine injection was carried out blindly in these cases. One patient in the intervention group experienced adductor contraction. Among 30 patients in the control group, 5 patients had leg jerking, and in 2 patients, the procedure ended incompletely because of muscle spasm. Comparing these two groups, transvesical ONB effectively decreased leg jerking during TURBT (16.5% vs 3%; P < 0.05).
Conclusion:
Local blockade of the obturator nerve during cystoscopy is an effective method to avoid its stimulation in TURBT. It can be performed easily, and we did not experience any serious complication.
Introduction
Minor bleeding and irritative symptoms are common side effects in the immediate postoperative period. The major complications of uncontrolled hematuria and clinical bladder perforation occur in fewer than 5% of cases. 1 The incidence of perforation can be reduced by attention to technical details, avoiding overdistention of the bladder, and using anesthetic paralysis during the resection of significant lateral wall lesions to lessen an obturator reflex response. 2 –4
For most tumors on the bladder floor or dome, there is no special anesthetic requirement. In dealing with tumors on the lateral bladder wall, however, electrosurgical resection is more likely to stimulate the adjacent obturator nerve, leading to inadvertent bleeding and bladder perforation. General anesthesia with paralytic agents is preferred in this situation. 1
The obturator nerve runs in close proximity to the inferolateral bladder wall, bladder neck, and lateral prostatic urethra. Transperineal local anesthetic blockade of the obturator nerve distal to the site of stimulation has been suggested to be effective in preventing adductor muscle contraction during the transurethral procedures. The success rate of the transperineal obturator nerve block using the ‘‘blind anatomic approach’’ has been reported to be 83.8 to 85.7%. 3 –6
In this study, we introduced a new method for obturator nerve block (ONB). In this method, we used the transvesical approach and a nerve stimulator named STIMUPLEX® (Fig. 1) to localize the obturator nerve. Then, 5 to 10 mL of lidocaine was injected around the obturator nerve across the lateral bladder wall during cystoscopy by passing a needle across the bladder wall.
Nerve stimulator.
Patients and Methods
A total of 152 patients with bladder tumors underwent TURBT between April and October 2009. Among these patients, 108 were at high risk for general anesthesia, and spinal anesthesia (SA) was strongly suggested by the anesthesiologist. After obtaining approval from our local ethics committee, 103 patients were included in our study.
Forty-seven patients presented with gross hematuria, and 20 patients presented with irritative urinary symptoms. The rest of the patients were detected in follow-up of previous bladder tumors. Results of the cytology study were positive in 30 patients.
Although there is no clear indication to perform ONB in TURBT, it is recommended in tumors of the dorsolateral part of the bladder wall. Thirty-eight patients were excluded from ONB because the tumor was very small (less than 1 cm) or there was not any involvement in the dorsolateral bladder wall and the tumor was exclusively in the dome or floor of bladder. In five patients, the tumor was too extensive; they were excluded from the study, and after confirmation of the disease through a biopsy procedure, they became candidates for radical cystectomy.
Finally, 60 patients who had obvious papillary tumor in the posterolateral bladder wall entered the study and were randomly categorized in the intervention and control groups. The patients were assigned to intervention and control groups using random allocation software. 7 In four patients, we blocked the obturator nerve bilaterally.
The mean ages of patients were 62 ± 11 years (range 43–79 y) in the case and 61 ± 12 years (range 40–78 y) in the control group. Male to female ratio was three.
After performing SA, confirming its effectiveness, and before draping, one electrode was connected to the adductor muscles of the thigh and the other was connected to a 22-gauge needle. We used this needle for both lidocaine injection and currency conduction. Then, we started cystoscopy. The needle electrode could be passed through the working channel of the cystoscope.
Although there is no specific landmark in the cystoscopy to determine the obturator nerve, the topographic relation of the bladder wall to the passage of the obturator nerve in the minor pelvis has been described in previous studies. The obturator nerve is supposed to pass in close proximity to the posterolateral bladder neck, trigone, and posterior urethra. 5 We inserted the needle electrode in the posterolateral bladder wall between the ureteral orifice and the bladder neck. To have a better view, we filled the bladder. Then, the needle was inserted about 1.5 cm in the bladder wall to pass the bladder diameter. Up to current intensity of 1 mA was transferred through the needle electrodes to induce obturator nerve stimulation. When the exact site of the obturator nerve was detected, we slowly injected 5 to 10 mL of lidocaine across the posterolateral bladder wall around the obturator nerve through the needle electrode (Fig. 2). We used electrical current to confirm ONB. Then the needle electrode was removed and TURBT started.
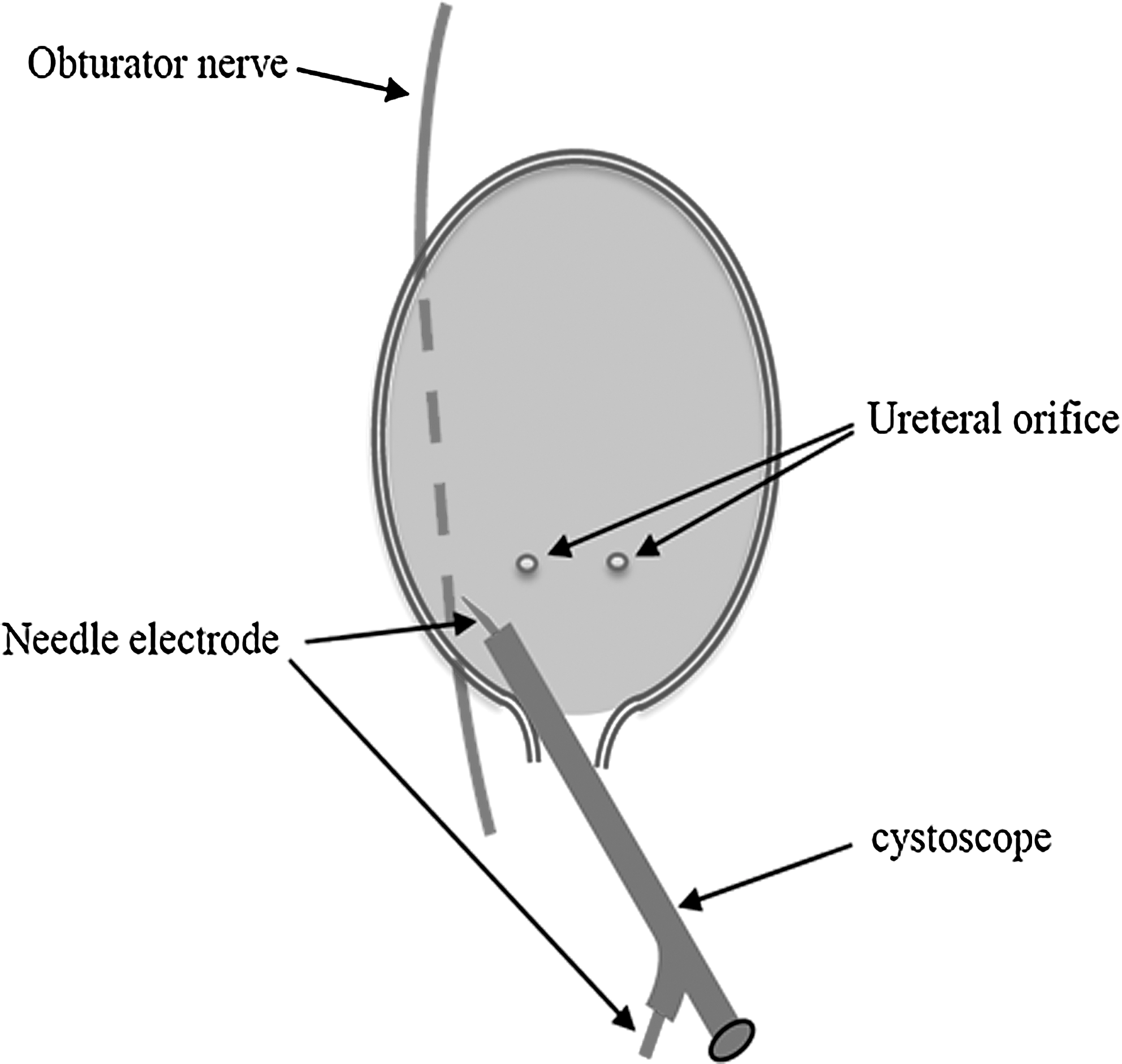
Nerve stimulation and lidocaine injection using a needle electrode through the working channel of the cystoscope.
Nerve stimulation was begun using a current intensity of 1 mA. If there was no adductor contraction with a current intensity of 1 mA, we would change the site of the needle electrode about 1 cm.
Insertion of a 22-gauge needle in the bladder wall sounds as if it is a safe procedure. We were meticulously cautious not to insert the needle into the tumor. All the procedures except SA were performed by urologists.
Using this technique, we provided 34 ONBs in 30 patients in the intervention group. Thirty patients underwent TURBT without ONB as the control group. TURBT was performed by another surgeon who was not aware of ONB.
Every lower extremity jerk was registered. Finally, the prevalence of adductor contraction and the duration of the procedure were calculated in the intervention and control groups.
The qualitative data were tested using a chi-square or Fisher exact test. All the analyses were performed using SPSS 13.0 software. We compared adductor contracture in case and control groups.
Results
Forty-seven patients were new cases and 13 patients were detected in a follow-up study of previous bladder tumor.
The procedure time was calculated from cystoscopy to insertion of a Foley catheter at the end of the procedure. It was 45 ± 10.4 minutes on average in the case group and 40 ± 8 minutes in the control group. ONB added 6.3 minutes to the time of operation in the case group.
Of 34 ONBs in 30 patients in the case group, 28 received the blockade after determination of the exact site of the obturator nerve by nerve stimulation (4 bilateral and 20 unilateral). In six patients, we could not find the exact site of the obturator nerve, and the blockade was carried out blindly. In one of them, muscle spasm occurred.
In the control group, five patients experienced adductor contraction during TURBT. Although we had no bladder perforation or inadvertent bleeding in the control group, in two patients, the resection of tumor could not be completed because of muscle spasm, and we performed TURBT under general anesthesia in another session in these cases.
Side effects of lidocaine, such as dysrythmia, seizure, anaphylaxis, and bradycardia, were not experienced in our cases. Lidocaine injection seems a safe and easy procedure to perform.
Using the Fisher exact test to analyze these data, we found that obturator stimulation is statistically less common after transvesical ONB (3% vs 16.5%; P < 0.05).
Discussion
Transurethral resection (TUR) of bladder tumors is both a diagnostic and a therapeutic procedure. During TURBT of tumors in the postero-lateral bladder wall, trigone, bladder neck, and proximal urethra without muscular relaxation, direct stimulation of the obturator nerve by the electroresectoscope is not unusual. In spite of some variations, the obturator nerve runs in close proximity of these organs. In one study, 63 of 114 patients experienced adductor spasm elicited by obturator stimulation during TURBT. 3 The resulting obturator reflex and adductor contraction may lead to severe complications—at worst, to a perforation of the bladder. Therefore, if resection of a tumor in the posterolateral bladder region is necessary, muscle relaxation is often needed. 1
When the patient is under general anesthesia, muscle relaxation can be applied using succinylcholine or other muscle relaxants. When the patient has received SA, however, muscle relaxation can result in respiratory failure. In general anesthesia, because the patient is under mechanical ventilation, muscle relaxation can be safe.
Most patients with bladder tumor are heavy smokers. In addition, the median age at diagnosis of urothelial carcinoma is 69 years in men and 71 years in women, so cardiopulmonary conditions are serious limitation for general anesthesia in the patients. 8 In a major proportion of patients, SA is a better choice in TURBT. 8,9
When the patient is receiving SA and TUR of the tumor in the posterolateral wall of the bladder is planned, ONB is highly recommended. 3 –6
The obturator nerve is a mixture of both motor and sensory nerves. To prevent adductor muscle contraction during TUR procedures, it is necessary to block its motor neurons distal to the site of stimulation. 8 Therefore, ONB should be considered when the patient is receiving SA to minimize adductor muscle spasm.
Different techniques for local blockade of the obturator nerve have been introduced, but they are either difficult to perform or unreliable. 3 –6 ONB in the obturator canal by local anesthesia is one of these techniques. The success rate of the ONB using the ‘‘blind anatomic approach’’ has been reported to be 83.8% to 85.7%. 3 –6
Some authors recommend neuroelectrical stimulation to confirm ONB. They have shown that obturator reflex is trivial by this method. No single adductor contraction has been demonstrated in studies in which electrostimulation was used to block the obturator nerve in relatively large numbers of patients. 10 –13
Several methods and modifications have been introduced in the medical literature to promote the success rate in ONB. Some articles even have proposed using ultrasonographic landmarks to determine the obturator nerve. 14 Recently, bipolar TUR of bladder tumors has offered suitable results in preventing obturator nerve reflex. 15
Until now, the transperineal approach has been the predominant approach of ONB. Transperineal ONB is performed by anesthetists. It is a time-consuming and technically challenging procedure, and most anesthetists do not have enough experience in this procedure.
In this study, we showed that the transvesical injection of lidocaine, as described, is an effective and safe procedure. It is not time consuming, and every urologist can perform it easily.
Using endoscopic procedures to conduct peripheral nerve block can be considered an innovation in the field of nerve block.
In this study, we performed ONB in all the patients in the intervention group. Considering the low incidence of adductor spasm without ONB (16%), it can be a nice idea to block the obturator nerve when adductor spasm happens, as recommended by Tatlisen and associates. 3 In this method, we can guess the exact site of obturator nerve without wasting time using nerve stimulation.
Conclusion
Injection of lidocaine during cystoscopy across the posterolateral bladder wall is an effective and safe method of ONB. It can prevent adductor contraction and bladder perforation in patients with tumors in the posterolateral bladder wall and bladder neck.
Footnotes
Disclosure Statement
No competing financial interests exist.