
Abstract
Background and Purpose:
Vascular pseudoaneurysm is a well-documented complication that results after injury to an arterial wall. We review the urologic literature for all reported postprocedural and post-traumatic cases of pseudoaneurysm.
Methods:
A comprehensive review of the peer-reviewed literature was performed for reported cases of vascular pseudoaneurysm, with emphasis on clinical presentation and treatment options.
Results:
Vascular pseudoaneurysm is a high-pressure collection of blood that communicates directly with an arterial vessel. The clinical presentation varies, depending on the location and size of the lesion, and can be quite dramatic and potentially life threatening. There may be an increasing incidence of pseudoaneurysms after minimally invasive and laparoscopic techniques. Selective and superselective embolization is the preferred treatment for patients with vascular pseudoaneurysms.
Conclusions:
Vascular pseudoaneurysm is an important but rare complication that is increasingly reported after minimally invasive urologic surgery. This diagnosis necessitates a high index of suspicion and radiologic acumen. Treatment is individually tailored to each patient, but selective embolization appears to be the standard of care.
Introduction
Vascular pseudoaneurysms are a common cause of delayed hemorrhage after several surgical procedures. Pseudoaneurysms result from subtotal injury to an arterial wall, allowing protrusion of the inner layers of the arterial wall under pressure, resulting in a “pulsatile hematoma” that can dissect tissue planes and fill potential spaces. Rupture of a pseudoaneurysm is potentially a fatal event, particularly pseudoaneurysms that occur in large visceral arteries.
The incidence of reported cases of this relatively rare complication is on the rise, and treatment for patients with pseudoaneurysms has become commonplace in the field of interventional radiology. Given the recent surgical trend in urology and other surgical specialties to adopt minimally invasive procedures, their incidence will likely grow. For these reasons, it is essential to understand the diagnostic hallmarks and treatment options for pseudoaneurysms.
In this article, we will discuss the natural history of pseudoaneurysms, in general and within the context of a urologic practice, as well as how best to diagnose and manage them.
Methods
PubMed and MEDLINE searches were performed in May 2008 using the terms pseudoaneurysm, false aneurysm, pulsatile hematoma, and pulsatile mass. Only titles in English were considered. All abstracts were reviewed and assessed for relevance to the topic. Appropriate manuscripts were collected electronically or by hand. The rarity of the diagnosis resulted in no prospective investigations; therefore, stringent application of data quality was not applied to this analysis, particularly in the arena of pseudoaneurysm diagnosis and management.
Results
Etiology
Pseudoaneurysms are pulsatile hematomas that result from an injury to the outermost layer of an arterial wall (tunica adventitia). The inner layers (tunica intima and tunica media) of the arterial wall protrude through the defect, resulting in a pressurized sac that can dissect into potential spaces and through tissue planes. Continuity with the arterial lumen is maintained via the aneurysmal neck that can be variable in width. They differ from true vascular aneurysms (whose diverticular protrusions are composed of all three wall layers) and therefore are termed pseudoaneurysms, false aneurysms, pulsatile hematomas, or pulsatile masses.
Pseudoaneurysms can occur to any artery after physical injury or inflammation to the vessel wall. 1 Iatrogenic pseudoaneurysms are significantly more common than primary pseudoaneurysms. The most common iatrogenic etiology is femoral arterial access with a large-bore catheter for various endovascular procedures, such as cardiac catheterization. 2 Pseudoaneurysms, however, have been widely reported after both vascular and nonvascular surgical procedures; within the field of urology, they have been reported after percutaneous nephrolithotomy (PCNL), partial nephrectomy, radical nephrectomy, radical prostatectomy, and radical cystectomy. 3 –11 Surgery can result in a pseudoaneurysm directly or indirectly if a postoperative infection or abscess develops. Noniatrogenic etiologies are less common and include vasculitis, inflammation, or infection of an adjacent organ (eg, pancreatitis) or trauma (both blunt and penetrating). 1
Incidence and clinical impact
The true incidence of pseudoaneurysms is not known. They are the cause of more than 50% of delayed hemorrhage after PCNL and partial nephrectomy. 3 Not all pseudoaneurysms are symptomatic and subsequently may never be identified. As in the case of renal masses, pseudoaneurysms are increasingly being found incidentally on imaging that is performed for another indication. 1,2
Pseudoaneurysms can follow three general courses: Thrombosis, symptomatic progression/enlargement, and rupture. Unstable pseudoaneurysms that occur within large potential spaces (eg, the retroperitoneum) may enlarge, resulting in compression of adjacent organs or nervous structures. These pseudoaneurysms are at high risk of rupture. Small, stable pseudoaneurysms typically occur in close spaces and are capable of spontaneous thrombosis. Such thrombosis can predispose to vascular thromboembolism. Lastly, pseudoaneurysms can also become infected, which poses a particularly difficult clinical dilemma. 12
General clinical characteristics
Pseudoaneurysms can be divided simply into superficial and deep visceral pseudoaneurysms. By far, superficial pseudoaneurysms after arterial catheterization predominate. These small, postcatheterization pseudoaneurysms are typically managed differently because of their size and accessibility. 1,2 For the purposes of this review, we will focus on deep visceral pseudoaneurysms.
The clinical diagnosis of a deep visceral pseudoaneurysm can be challenging. The classic palpable pulsatile mass, with an audible thrill, may be found on abdominal examination, but its absence certainly does not exclude the diagnosis. In fact, very few pseudoaneurysms are diagnosed in this manner. Pseudoaneurysms can grow significantly, creating a mass effect that can compress abdominal and retroperitoneal structures and resulting in referred pain or organ dysfunction (eg, hydronephrosis, bowel obstruction), vague abdominal symptoms (eg, nausea, anorexia, colic), or ischemic necrosis of the surrounding tissues. 1,2
Patients most commonly present with signs and symptoms of hemorrhagic shock several days after a surgical procedure. Gross hematuria after renal surgery is a sensitive indicator of pseudoaneurysm formation, but its absence does not rule out the diagnosis. 3,4,6,7 The diagnosis is usually confirmed on radiographic imaging.
Rupture, fistulization, and local compression are the most common complications that are associated with the diagnosis. Compared with true aneurysms, pseudoaneurysms are significantly more likely to be symptomatic, associated with clinically detectable hemorrhage, and necessitate medical or surgical intervention. 2,13 Pseudoaneurysm rupture is the most catastrophic of these complications, with associated mortality rates ranging from 40% to 100% when affecting deep visceral arteries. 1,2,14 Depending on the location of the pseudoaneurysm, rupture typically results in pain, evidence of hemorrhage (eg, hematuria, hematochezia, or hematemesis), and hemodynamic instability. Pseudoaneurysm fistulization is a rare occurrence, but fistulae with adjacent ureters, bowel, and gynecologic structures have been reported.
Pseudoaneurysms in urology
Pseudoaneurysm formation complicates percutaneous renal surgery and partial nephrectomy most commonly because of the plentiful microvasculature intrinsic to the renal parenchyma. After these procedures, pseudoaneurysm is the most common cause of delayed hemorrhage. 3,4,6,7
Major hemorrhage after PCNL is a rare event that affects approximately 1% to 3% of patients undergoing the procedure. Patients typically present with gross hematuria, retroperitoneal hematoma, bleeding from the nephrostomy tube or tract, and symptoms that are consistent with hypovolemia. 3,15 In the majority of cases, delayed bleeding can be managed expectantly with fluid resuscitation and blood transfusion as needed. Only persistent or symptomatic hemorrhage necessitates treatment. In the largest single institution series, Richstone and associates 3 found 57 cases of major postoperative hemorrhage out of nearly 4700 (1.2%) patients treated with percutaneous renal surgery, and pseudoaneurysm was the most common etiology, found in 53%, followed by renal vessel laceration and arteriovenous (AV) fistula (25% each). The vast majority of these patients (95%) were successfully treated with selective embolization (SE). Large stone size appears to be the only preoperative predictor of delayed hemorrhage and pseudoaneurysm formation after PCNL. 4
Delayed bleeding is a rare complication after partial nephrectomy, slightly more so when performed laparoscopically (4%–6%) than via an open approach. 15 Pseudoaneurysm formation is a common cause of postoperative hemorrhage in patients who are undergoing partial nephrectomy. 6,7 Most episodes of delayed bleeding occur 1 week to 5 months postoperatively and present in a nearly identical manner as post-PCNL hemorrhage. 7 Diagnosis of a pseudoaneurysm in the nephrectomy bed is dependent on the size of the pseudoaneurysm, and most pseudoaneurysms cannot be positively identified except on contrast angiography.
Albani and Novick 6 reported an incidence of pseudoaneurysm formation within the partial nephrectomy bed of 0.43% in their series of 698 open procedures, compared with 1.7% after a laparoscopic approach reported by Singh and Gill. 7 Although the same operative steps are followed for both procedures, laparoscopic suturing is technically more difficult and can result in inferior tension applied to transected vessels compared with hand suturing. Also, overreliance on prothrombotic materials after laparoscopic partial nephrectomy, such as Floseal,® may result in incomplete physical ligation and predispose to pseudoaneurysm formation. Indiscriminate placement and replacement of suture needles into the renal parenchyma may also inadvertently injure deep vessels, resulting in pseudoaneurysm formation. Lastly, partial nephrectomy commonly necessitates hilar clamping with Satinsky or bulldog clamps, which can result in renal artery injury and pseudoaneurysm formation. 16
Delayed hemorrhage after radical nephrectomy occurs less commonly than after partial nephrectomy, but pseudoaneurysm has been reported as a rare complication. 9,10,16 Bluebond-Langner and colleagues 10 reported on persistent hemorrhage from an intercostal artery pseudoaneurysm that resulted from injury during port placement for a retroperitoneal radical nephrectomy. Another group reported on an adrenal bed pseudoaneurysm after laparoscopic nephroureterectomy that formed after arteriolar injury from a poorly applied surgical clip, eventually resulting in patient death. 9
Pseudoaneurysms after pelvic surgery are much less common than after renal surgery, and typically result from collateral damage during the operation. Hampson and coworkers 8 reported a pseudoaneurysm of the common iliac artery 2 weeks after radical cystectomy and pelvic lymphadenectomy for muscle invasive transitional-cell carcinoma. The patient presented in abdominal pain with evidence of hypovolemia; the diagnosis was confirmed on contrast imaging, and the lesion was controlled with SE. Beckley and associates 11 reported an accessory obturator artery pseudoaneurysm after robot-assisted radical prostatectomy, and we have recently seen a prostatic pedicle pseudoaneurysm after the same procedure (Fig. 1). Prolonged gross hematuria developed in both patients, resulting in repeated episodes of clot retention. After expectant management failed in both cases, angiography successfully identified the vascular lesion and SE successfully controlled the hemorrhage.
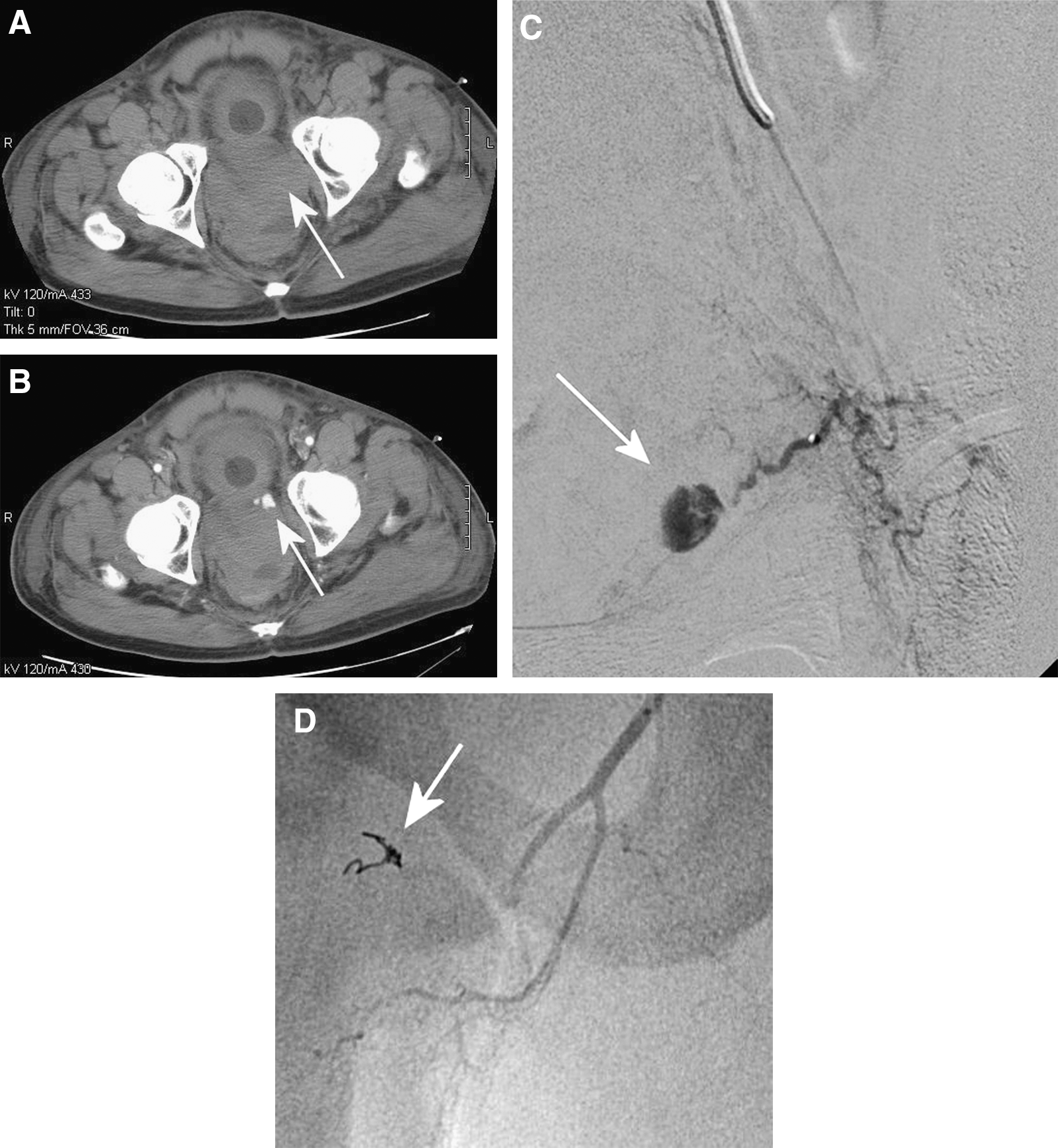
(
Trauma commonly results in bleeding complications, including pseudoaneurysm formation. 17 –19 Renal artery pseudoaneurysm has been reported after both penetrating and blunt trauma. These patients commonly present several days after the initial injury with persistently but slowly developing anemia and signs of hypovolemia. Gross hematuria is not always present, but should increase suspicion for a renal pseudoaneurysm.
Diagnosis. Currently, the vast majority of pseudoaneurysms are diagnosed radiographically on imaging performed for suspected delayed hemorrhage. Important clinical hallmarks of the diagnosis include evidence of bleeding, hypotension, tachycardia, localized pain, palpable pulsatile mass, and anemia. 1,2 In addition to surgery and percutaneous biopsy, risk factors include anticoagulant use, antiplatelet therapy, liver dysfunction, alcoholism with history of pancreatitis, and autoimmune vasculitis syndromes, such as Behçets syndrome, polyarteritis nodosa, and lupus. 1
By far, deep visceral pseudoaneurysms are most commonly diagnosed by contrast CT angiography. Suspected pseudoaneurysms can then be confirmed with Doppler ultrasonography. CT angiography is quick, nonoperator dependent, and can provide a three-dimensional reconstruction of the hematoma, affected vasculature, and adjacent organs. A large hematoma is differentiated from a pseudoaneurysm on CT by the presence of confined enhancement within the hematoma during the arterial phase. The entire hematoma may not enhance completely. The pseudoaneurysm may contain a significant volume of clot formation; therefore, evidence of even a small area of enhancement of the hematoma should raise the suspicion of a pseudoaneurysm. Pseudoaneurysms of small arterioles and intraparenchymal pseudoaneurysms (eg, after partial nephrectomy) can be more challenging to diagnose on CT, and differentiation from an AV fistula is not always possible (Fig. 2). MRI is an expensive alternative to CT that necessitates a substantial amount of time to perform and is poorly suited in the diagnosis of a suspected pseudoaneurysm. 2
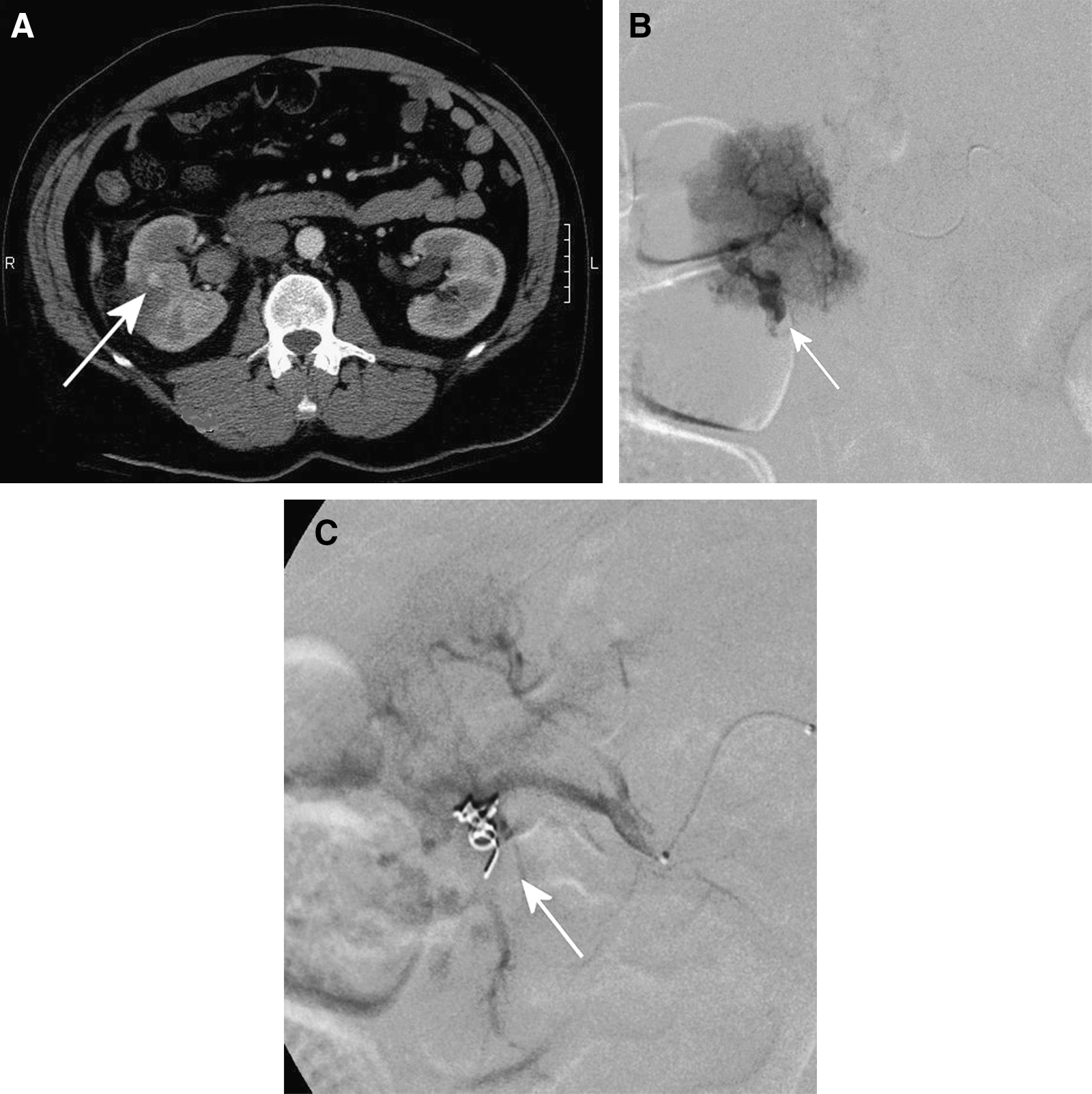
(
Doppler ultrasonography is a sensitive method to confirm the presence of a pseudoaneurysm. 1,2,18 The hematoma can be identified in B-mode as a poorly defined collection with mixed echogenicity, and the pseudoaneurysm will appear as a central hypoechoic cystic-like lesion immediately adjacent to an artery (Fig. 3A). Doppler ultrasonography allows for detection of arterial flow within the cystic lesion. Classically, pseudoaneurysms demonstrate a yin-yang flow pattern, whereby arterial inflow during systole is followed immediately by outflow during diasystole (Fig. 3B). Sensitivity and specificity of Doppler ultrasonography for the detection of pseudoaneurysms in most studies is in excess of 90%, respectively. 1,2,13,18 The primary disadvantage of the technology is the operator-dependent nature of ultrasonography.
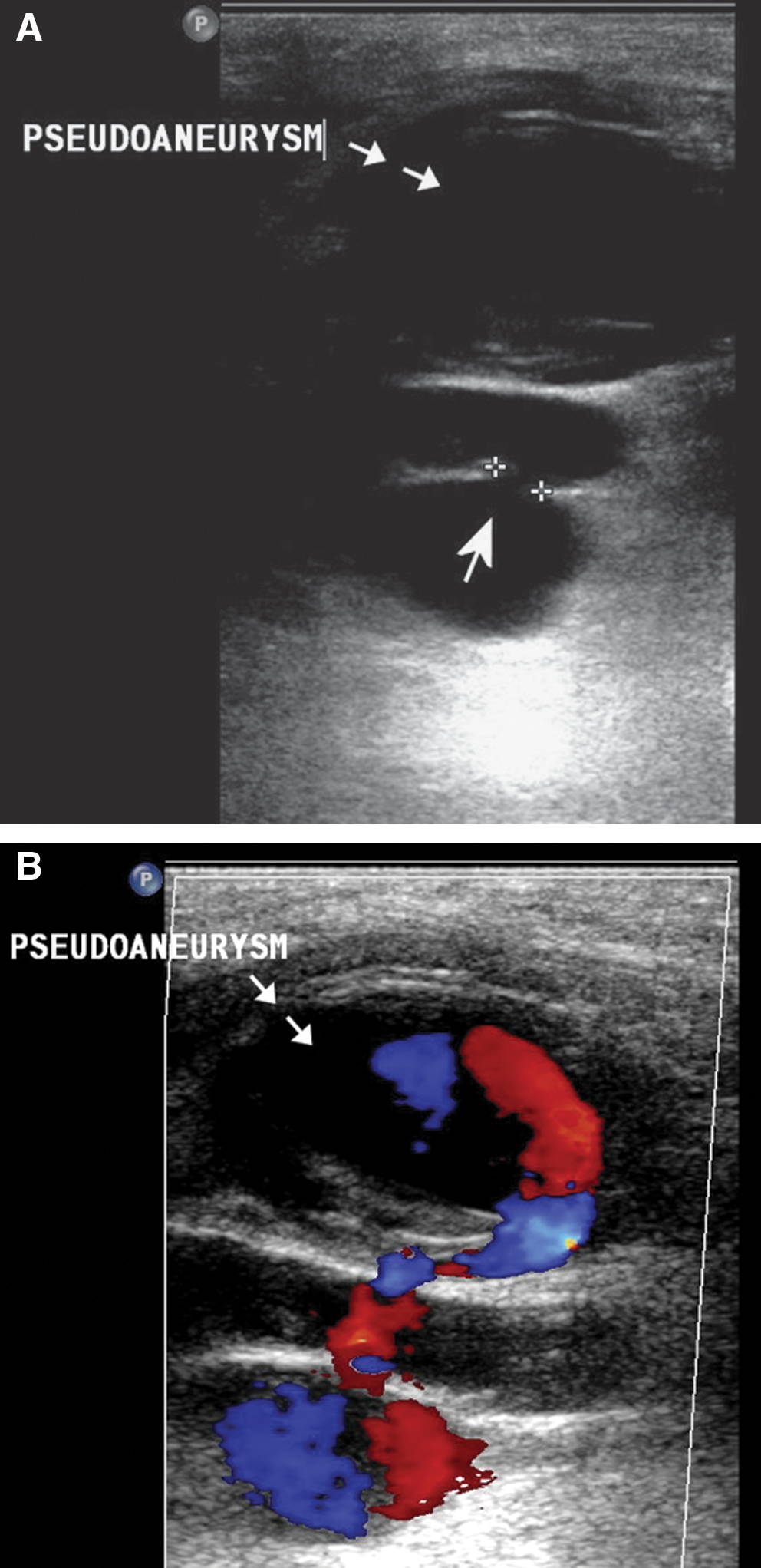
(
The gold standard study for the detection of pseudoaneurysms is standard contrast angiography. The advantage to angiography is that it allows for real-time estimation of arterial collateralization to the affected vessel, and it allows for concurrent therapeutic SE. Angiography is typically more sensitive than other modalities and can identify additional vascular lesions at the time of the procedure. The diameter of the pseudoaneurysm neck can also be established with angiography, which is an important factor in treatment planning. The disadvantages to angiography include the invasive nature of the technique with its own associated morbidity and the necessity of using potentially nephrotoxic contrast material. In general, contrast angiography should be used once the diagnosis is made or suspected on initial abdominal imaging.
Treatment. It is evident that not all pseudoaneurysms need treatment. Spontaneous thrombosis does occur and probably results in the underestimation of the incidence of this complication. It is generally recommended that small (<1 cm), asymptomatic, parenchymal pseudoaneurysms that are incidentally found be observed and treated only if they become symptomatic, do not resolve on further imaging, or enlarge. 2 All symptomatic and extravisceral pseudoaneurysms should be treated because of the risk of spontaneous rupture and mortality.
Traditionally, the treatment of pseudoaneurysms consisted of open surgical ligation with arterial bypass when necessary. This procedure can be technically difficult because of the potential for uncontrolled bleeding, which can obscure the vascular anatomy. This was particularly true for small, parenchymal pseudoaneurysms that commonly ultimately result in complete extirpation.
Percutaneous injection of thrombin as a treatment for pseudoaneurysm was first used by Cope and Zeit 20 using ultrasonographic guidance. Currently, 0.5 to 1.0 mL of a 1000 IU/mL concentration of thrombin is slowly injected directly into the center of the pseudoaneurysm until thrombosis of the pseudoaneurysm is confirmed with ultrasonography. 21 The success rate of the technique approaches 90%, and it can be used in the setting of systemic anticoagulation or antiplatelet therapy. It is used largely to treat postcatheterization-induced pseudoaneurysms, but has also been described for deep visceral pseudoaneurysms with success and pseudoaneurysms that are not accessible with current SE techniques. 21,22 Thromboembolism is the most significant complication of pseudoaneurysm thrombin injection, and it is recommended that the treating physician be capable of distal thrombolytic injection if necessary.
Percutaneous SE and superselective embolization is the contemporary standard of care for most pseudoaneurysms. 1 –3,13,23 –26 As stated, digital subtraction angiography allows for excellent identification of the pseudoaneurysm as well as collateralization to the affected vessel, in addition to the vascular defects such as AV fistulas and vascular stenosis. Current SE techniques are associated with a better morbidity profile than traditional surgical management. Several different thrombotic materials, such as coil deployment and gelfoam, can be used to tailor treatment based on the unique features of the given pseudoaneurysm. Alternatively, coated vascular stents can be used to isolate the pseudoaneurysm from the arterial lumen.
The nuances of SE are beyond the scope of this article but are well described in recent reviews. 1,2,14,23,24 The critical parameters necessary to successfully treat pseudoaneurysms with SE include the pseudoaneurysm size, the width of the pseudoaneurysm neck, evidence of collateral arterial supply to the affected artery, and the expendability of the affected artery (Table 1). Percutaneous direct embolization of the pseudoaneurysm is best used when the affected artery cannot be sacrificed (eg, renal artery) or the lesion cannot be accessed via an endovascular approach. 22,23 If the pseudoaneurysm arises from an expendable artery, thrombosis of the artery distal to the pseudoaneurysm is preferred. In the setting of arterial collateralization, complete exclusion of the pseudoaneurysm both proximal and distal to the neck is recommended.
Authors report treatment of both pseudoaneurysms and true aneurysms that in some instances ruptured.
SE = selective embolization.
Outcomes of SE. Successful vascular control with a single SE procedure has been reported to range from 89% to 100%. 1 –3,13,23 –26 Initial failure from recanalization is a rare event but can usually be salvaged with a second SE procedure. SE is well tolerated with few treatment-related complications; however, these patients commonly have complications from the hemorrhage itself. Complications of SE include access-site bleeding, infection and pseudoaneurysm formation, contrast toxicity, recanalization of the pseudoaneurysm, and rarely, iatrogenic rupture of the pseudoaneurysm.
Renal function after SE for renal pseudoaneurysm correlates directly with the amount of kidney parenchyma embolized and is typically self-limiting. El-Nahas and associates 27 followed 30 patients who were treated with SE for post-PCNL hemorrhage an average of 3.9 years with intravenous urography and dimercaptosuccinic acid scans. Bleeding was successfully controlled in more than 90% of patients with no long-term evidence of renal dysfunction. Two (7%) patients lost all renal function in the affected kidney. On average, a 10% increase in renal function of the treated renal unit was seen at 30 months. Poulakis and colleagues 28 studied five patients with iatrogenic and trauma-related renal pseudoaneurysm who were treated with SE. Bleeding was controlled in all patients. Post-SE azotemia (measured by serum creatinine) resolved in all patients within 10 days of the procedure, and the average percentage of photopenia demonstrated on diethylene triamine pentaacetic acid scan was 9% (0%–20%) 6 months after the procedure.
As expected, the management of pseudoaneurysm formation in a solitary kidney poses the greatest risk to renal function. 3,27,28 There is no generally accepted approach to this clinical situation. Vascular stent placement or surgical ligation and bypass should be considered for large pseudoaneurysms of the main renal artery because of the risk of thromboembolism or renal infarction after SE.
Conclusions
Pseudoaneurysms are a rare but potentially lethal complication of urologic surgery whose incidence appears to be increasing as our field embraces minimally invasive techniques. Pseudoaneurysms account for the most common etiology of delayed hemorrhage after percutaneous renal surgery and partial nephrectomy. SE is the most appropriate initial management strategy, followed by percutaneous injection of thrombin. Surgical management is reserved for SE failures and patients with clinically unstable hemorrhage. Meticulous vascular control with surgical clips or suture followed by a clean ligation of isolated vessels and vascular pedicles is the best method to prevent iatrogenic pseudoaneurysm formation.
Footnotes
Disclosure Statement
Thomas W. Jarrett, consultant, Gyrus/ACMI; Jason D. Engel, investigator, Vivus. No competing financial interests exist for the other authors.