
Abstract
Robot-assisted laparoscopic prostatectomy is rapidly gaining favor as a minimally invasive method to surgically address prostate cancer. The sophisticated equipment and unique positioning requirements of this technology require exceptional preparation and attention to detail to minimize the chance of surgical complications. We present the case of a 57-year-old man who developed left calf compartment syndrome after (robot-assisted laparoscopic prostatectomy) requiring fasciotomies. We use this example to highlight specific areas of risk unique to the da Vinci Surgical System® using intraoperative photos to show danger areas as well as review basic positioning requirements common to all prolonged pelvic surgeries performed in Trendelenburg position.
Introduction
Part of the debate over surgery versus watchful waiting focuses on the potential risks and complications of surgery, such as erectile dysfunction or urinary incontinence. Dr. Patrick Walsh developed the anatomical radical retropubic approach to minimize these side effects. 4,5 The success of the anatomical radical retropubic prostatectomy led to the application of laparoscopic tools to this operation. 6 The laparoscopic approach has yielded equivalent oncological results with improvements in cosmesis, but the learning curve of this technique is significant. The application of the da Vinci Surgical System® combined the minimally invasive approach inherent to laparoscopic surgery with the three-dimensional advantages of open surgery. 7 Large case series have demonstrated the viability of this approach and highlight the reduction in blood loss and improvements in potency and continence rates in comparison to open radical retropubic prostatectomy while maintaining identical oncological outcomes. 8 –10 As the popularity of this approach for prostate cancer treatment continues to increase, the need for an awareness of rare but potentially devastating complications unique to the technique as well as a reminder of basic positioning common to all pelvic surgery performed in the Trendelenburg position is paramount.
Case Report
A 57-year-old man was referred to our institution for consideration of robot-assisted laparoscopic prostatectomy (RALP). On routine screening, his PSA was noted to have risen from 2.4 to 3.9 ng/mL over the course of a year. Transrectal ultrasound-guided prostate biopsy showed Gleason 3 + 3 = 6 adenocarcinoma involving 50% of the prostatic tissue from the left mid-biopsies, 10% of the prostatic tissue from the right mid, and 60% of the prostatic tissue from the right lateral apex. On presentation, the patient denied any bone pain, weight loss, or significant urinary symptoms although he was taking tamsulosin (0.4 mg per os [by mouth] daily) for weak urinary stream with minimal improvement in symptoms. The patient's medical history was significant for hypertension, arthritis, and a previous neurological work-up for possible transient ischemic attacks with a normal bilateral carotid ultrasound but concern over atherosclerotic end cerebral arteries. He also reported a work-related accident in the early 1980s, which resulted in left-sided rib fractures but no known long-term sequelae. His surgical history was significant for appendectomy and knee surgery in 1992 as well as an ureteroscopic lithotripsy procedure in 2000, all of which he tolerated without complications. He had no family history of prostate cancer. He quit smoking 1 month before surgery after having smoked one to one and a half packs of cigarettes per day for 44 years.
On physical examination, he was a healthy-appearing man with a body mass index of 27. His prostate was smooth, without nodularity, and ∼40 g. His neurological examination results were normal. His peripheral pulses were not examined though his extremities had no evidence of cyanosis or edema.
After discussing his surgical options, he was consented and taken to the operating room where he underwent an uneventful RALP. General anesthesia was induced and the patient was placed on a Maquet split-leg operating table with care to pad his legs and arms. The Maquet operating table maintains the legs straight and split at ∼30 degrees without lithotomy, allowing the robot to be brought between them. Straps are used at the level of the calves and mid thighs with padding between them and the patient. Heparin was not used intraoperatively, but sequential compression boots were employed. The patient's position was tested in Trendelenburg before draping. He was placed in a 10-degree Trendelenburg position, and the procedure was begun using a Veress needle followed by placement of four robotic ports. The da Vinci S four-arm robot was docked and positioned. He was then placed in steep Trendelenburg position (defined as 25 degrees), and the remainder of the procedure was completed. The total operating room time was 317 minutes, whereas the robot-docked time was 238 minutes. The primary surgeon performed the key portions of the case, but a resident surgeon performed the majority of the case. Blood loss was 100 mL. There were no noted episodes of intraoperative hypotension. He was brought to the recovery room and then transferred to the surgical floor.
A few hours after arriving on the floor, he complained of significant left leg pain starting above his knee and radiating down to his foot. He also complained of a knot-like sensation on his left calf and a loss of sensation on his left medial thigh and all of his left toes. On examination, he was noted to have limited dorsi and plantar flexion of his ankle. He was able to flex and extend his knees and hips without difficulty. There were no bruises or discolorations noted on his left leg or hip. He had no shortness of breath or chest pain. His left calf was painful to palpation but not swollen. He had palpable posterior tibial and dorsalis pedalis pulses. He was given pain medication and re-examined 2 hours later, at which point he reported improvement in his ability to dorsi and plantar flex his ankle and return of his sensation of his medial thigh. He continued to have some loss of sensation involving his left toes and had pain involving his left lower leg; however, this was improved from before. Overnight, he was hypertensive with systolic pressures in the mid-160s requiring IV medications, and he continued to require intermittent pain medication. At approximately 4:30 the following morning, 6 hours after he was last seen, he reported chest discomfort. An electrocardiogram (EKG) was ordered and troponins were drawn. He was transferred to the cardiac unit for continuous EKG monitoring. His EKG showed sinus tachycardia and his troponins were normal. At this point it was also noted that his left calf was now significantly larger than his right and that he had again lost the ability to dorsi or plantar flex his left ankle. Vascular surgery was consulted for consideration of a lower extremity ultrasonography to rule out deep venous thrombosis. Before the ultrasonography could be completed, the swelling in his left calf worsened, the calf became very tight, and he lost all distal pulses in the left leg.
Vascular surgery ordered compartment pressure measurements, which were significantly elevated, at 78 mmHg (normal range 0–15 mmHg) for the left superficial compartment and 114 mmHg for the left lateral/anterior compartment (normal range 0–15 mmHg). Ankle to brachial indexes were also abnormal, showing monophasic flow in the left calf. Compartment syndrome was diagnosed and he was emergently taken to the operating room for fasciotomies. He tolerated the procedure well and his pain was significantly improved. Neurology was consulted, and magnetic resonance imaging and magnetic resonance angiography (MRA) of the leg was ordered. The magnetic resonance imaging showed no immediate signs of pathology. The MRA, however, showed occlusion of the left common iliac artery (Fig. 1). Given the extensive degree of collateralization present, both vascular surgery and radiology felt this represented a chronic condition possibly related to his work accident 25 years ago. He had wound vacuums placed on his fasciotomies and 7 days later returned to the operating room to have his wounds partially closed. Seven days later (14 days after his prostatectomy) he elected surgical repair of his left common iliac occlusion. Vascular surgery was planned for a bypass procedure, but during the procedure it was noted that the obstructed segment of artery appeared more acute, so a balloon thrombectomy was completed, which demonstrated a clot that by physical examination was suspicious for an acute to subacute injury. This was a surprise given the extensive collateralization present on his prevascular surgery MRA suggesting an acute on chronic etiology for the clot.
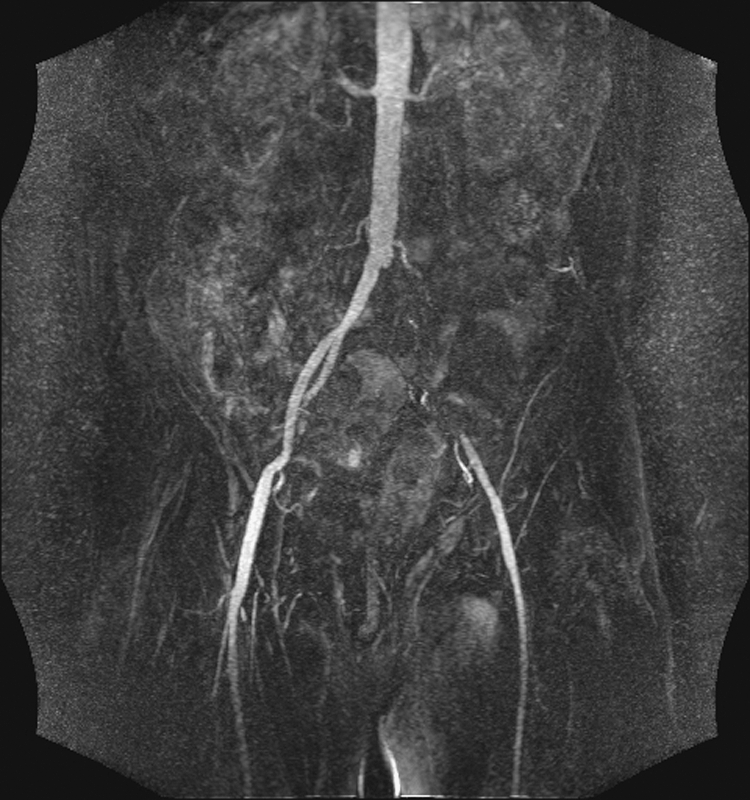
Coronal magnetic resonance angiography images showing significant occlusion of the left common iliac artery with collateral revascularization present.
Regarding his neuromotor status, by postoperative day 2 after RALP, he regained sensation to his toes but not to an area on the medial aspect of his foot. By 1 week postoperatively, he had plantar flexion but still had limited dorsi flexion of his ankle. The final pathology of his prostate showed Gleason 3 + 4 = 7 adenocarcinoma of the prostate involving both sides. His catheter was removed on postoperative day 18 in conjunction with the vascular surgery team. He later underwent skin grafts to the fasciotomy site without complications. Six months after his operation, he has regained all sensation on his leg except for a 2-inch strip of numb skin, just proximal to his left toes, extending up the dorsal aspect of the foot and anterior lower leg to the level just below the lateral skin graft. He has complete plantar flexion but can only dorsiflex to ∼90 degrees. He continues to work with physical therapy and has returned to work. His PSA remains undetectable.
Discussion
To our knowledge, this is the first reported case of lower extremity compartment syndrome after RALP and only the second case ever reported of compartment syndrome involving the da Vinci Surgical System. In 2005, Palese et al. 11 reported an example of gluteal compartment syndrome during one of their early cases of robotic pyeloplasty. The patient was morbidly overweight and the case took over 300 minutes. Although it is not specifically stated in the article, the implication is that the excess weight combined with a long operation in a less than optimal position led to the complication. Our operating room (OR) time of nearly 4 hours, while less than Palese's case, was clearly sufficient in a patient with unknown preexisting vascular insufficiency to cause acute worsening of his underlying iliac artery disease.
Potential risk factors that could increase the risk of compartment syndrome can be divided into those related to the patient, those related to operating room positioning, and those unique to the use of the robot. Regarding patient-specific factors, excess patient size and preexisting vascular abnormalities may increase a patient's risk of compartment syndrome. Diabetes can also contribute to reduced peripheral vascular perfusion. During an RALP, the patient must be placed in a very specific position and held there for duration of the case. The patient's legs must be abducted to allow the robot to be brought into the operative field and safely docked with the ports. The patient is also placed in a steep Trendelenburg position to allow the bowels to fall away from the surgical field, maximizing vision. Specific causes, not necessarily in this case, that may lead to compartment syndrome include Excessively tight compression from the pneumatic boots or straps on the lower extremities Excessive elevation or Trendelenburg position coupled with systemic hypotension or preexisting vascular abnormalities Pressure from weight of the lower extremity against the edge of the bed or leg holder Excessive flexion of knees or hips Excessive popliteal pressure from a stirrup if lithotomy position is used Pressure from one of the arms of the robot or surgical assistant
Prevention and the Robotic Timeout
After our intra-department discussion of this case, its management, and the risk factors that may have contributed, we elected to document our experience, with specific attention to patient positioning, in an effort to maximize dissemination of the lessons we learned from this unfortunate complication. Although we do not believe patient positioning was the sole cause of the complication in this case, we cannot be certain that it did not contribute to the complication. To ensure that patient positioning does not contribute to similar complications in the future, we reviewed patient positioning during an actual RALP and took photos to highlight one specific area of concern. As previously described, the patient is placed on a Maquet split-leg table in which the legs are maintained straight without lithotomy (Fig. 2). After anesthesia is induced, the patient is placed in steep Trendelenburg (25 degrees down), and the robot is docked to the trocars. Figure 3 shows the approximate degree of Trendelenburg. Figure 4 shows the robot being docked in a mock situation; the normal operating room drapes hide the patient's position. The steep Trendelenburg without lithotomy and the position of the robot to the patient is visible. During our discussion we considered docking the robot to the patient from the side, but felt that access to the robot and the patient was improved if the robot was docked between the patient's legs.

Mock patient on Maquet split-leg table. Note that legs are spread and straight; no lithotomy position is used.

Mock patient in steep Trendelenburg position with legs split but straight. Securing straps normally placed at the level of the calves and mid thighs bilaterally (with padding between them and the patient) were not used in this mock patient to prevent obscuring the position of the legs.

Mock patient with robot being docked between patient's legs. Notice legs are straight, patient is in Trendelenburg, and the robotic arm to the patient's left is in proximity to the patient's left leg.
Care is taken to avoid any contact between the arms of the robot and the patient during docking. Once the robot's arms are successfully docked to the trocars, the robot's arms are re-positioned to allow complete mobility of the robot during the case.
At this point the surgeon must ensure that no pressure points exist between the robot arms and the patient. One specific area of danger exists between the robot's fourth arm and the patient's left leg. Minimal clearance exists and it must be monitored for potential compression. Figure 5 shows the surgeon checking for clearance at this location by passing his hand between the patient and the robot. This step is repeated at regular intervals throughout the case by the assistant given the mobility of the robot's arms during the procedure.
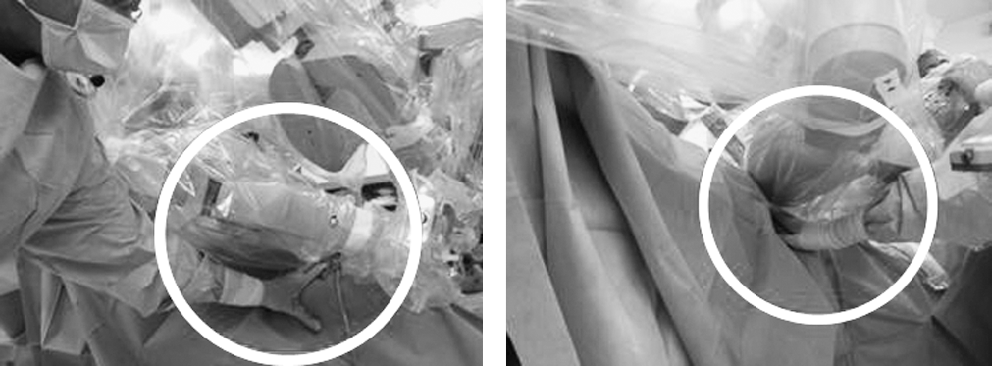
Surgeon checking space between patient's left lower leg and the robot's fourth arm during actual procedure.
To formalize the maneuvers previously described, we instituted a robot timeout, which is now used in every case. The robot timeout is a checklist that ensures that the following steps are appropriately followed during every case. Each step is documented and inspected after the robot has been docked, before all instrumentation are placed in the robot, and before the surgeon begins operating at the robot console. These steps are completed by the primary surgeon though physical examination ensures that the robot is not improperly contacting the patient. The content of our checklist is listed below: Position of extremities Type and location of restraints, positioning aids, and padding materials Position changes made during procedure (e.g., lowering or raising legs, and supine to lithotomy to supine) Use and location of warming and cooling blankets or devices
On a more general note, the majority of these steps are applicable to cases other than RALP. Further, compartment syndrome itself is an uncommon but not rare complication of many surgeries as well as trauma. Surgeons commonly perform pelvic surgery with patients in the Trendelenburg position, and with the exception of checking for improper contact between the robot and the patient, all of these steps apply to all surgical fields that use similar patient positioning. It is important for all surgeons to maintain a high degree of suspicion for compartment syndrome in any patient after prolonged Trendelenburg position regardless of the underlying pathology.
Conclusions
In this specific case, we feel that an unsuspected injury to the patient's left common iliac artery (likely related to his work-related injury many years previous though possibly related to an unknown vasculitis such as Burger's syndrome, which can cause chronic arterial narrowing) predisposed him to an acute thrombotic episode during prolonged surgery in the Trendelenburg position. We do not believe that there was pressure on the patient's left leg from the robot's fourth arm given the lack of discoloration or bruising and the significant collaterals present on postevent MRA. This case highlights the inherent risk of the Trendelenburg position and the need for careful postoperative monitoring of patients.
RALP is a safe, effective, and minimally invasive method to surgically treat prostate cancer and its use will likely continue to increase. The technological challenges of this procedure should not be minimized or overlooked, however, as the potential complications are significant. We hope that by highlighting one specific area of danger—the proximity of the fourth robot arm to the patient's left lower leg and recommending a formal robot timeout procedure—we can minimize the risk of complications during this procedure.
Footnotes
Disclosure Statements
No competing financial interests exist for any of the authors.