
Abstract
Background and Purpose:
Fluorescence cystoscopy (FC) with intravesical instillation of a photosensitizing agent has emerged as an adjunctive and safe diagnostic tool with high sensitivity and reasonable specificity; however, it has not been widely accepted, because it is time-consuming and expensive. The aim of the present study was to determine whether the use of the fluorescent dye pirarubicin [(2″R)-4′-O-tetrahydropyranyl doxorubicin] (THP) in endoscopy can improve detection of nonmuscle invasive urothelial carcinoma of the bladder.
Patients and Methods:
Forty-eight patients with known or suspected bladder urothelial carcinoma were enrolled in this prospective study between January 2008 and April 2009. The Storz D-light system was used to detect fluorescence 15 minutes after intravesical instillation with 30 mg THP. Endoscopic findings, histopathologic evaluation of biopsy lesions, and adverse effects of THP were recorded.
Results:
After THP uptake, the lesions appear bright orange under white light, and produce bright red fluorescence under blue light. Among 238 biopsies evaluated (84 malignant, 20 dysplasia, and 134 benign), sensitivity of overall tumors, carcinoma in situ (CIS), and dysplasia detection using FC was 96% (81/84), 100% (6/6), and 90% (18/20), respectively. The specificity of FC was 74.7% (115/154), and its false-positive rate was 32.5% (39/120). No significant systemic side effects or allergic reactions were observed other than a few cases of mild cystitis.
Conclusion:
THP endoscopy may improve the detection of nonmuscle invasive urothelial carcinoma of the bladder, especially CIS and flat lesions. Results indicate that THP is a promising fluorescent dye for diagnosis and follow-up of nonmuscle invasive bladder carcinoma. Moreover, it is inexpensive, easily available, simple to administer, and is associated with few side effects.
Introduction
The gold standard for detection and follow-up of bladder carcinoma is white light cystoscopy (WLC). 4 Small and flat urothelial malignancies, however, are difficult to visualize and may be missed during conventional WLC; therefore, sensitivity varies from 50% to 75%, depending on the experience of the investigator. In addition, detection by WLC is affected if the bladder is overdistended and trabeculated, or ongoing cystitis is present. 5 Thus, regular WLC and random biopsy are unable to detect all urothelial neoplasms in patients who are at high risk of recurrent bladder cancer. 6
To overcome this problem, photodynamic diagnosis (PDD) allows visualization of malignant cells or tissues by accumulation of photosensitive fluorescent dyes. Since the early 1990s, various studies have reported a higher sensitivity of bladder cancer detection using PDD with 5-aminolevulinic acid (5-ALA)-induced porphyrin fluorescence. 5,7 –10 New fluorescent dyes, such as hexaminolevulinate (HEX, also referred to as HAL) and hypericin, are considered more effective in the detection and diagnosis of bladder cancers. 11,12
The current guidelines of the European Association of Urology recommend fluorescence cystoscopy (FC) as a valuable aid for follow-up and endoscopic treatment of nonmuscle invasive urothelial carcinoma of the bladder. HAL is the only PDD agent approved by respective agencies to date 13 ; however, HAL is commercially available only in Europe, needs longer intravesical dwelling time, and is readily photobleached.
Pirarubicin hydrochloride [(2″R)-4′-O-tetrahydropyranyl doxorubicin] (THP) is an anthracycline anticancer agent that was approved in Japan and China as clinical prophylactic chemotherapy for nonmuscle invasive urothelial carcinoma of the bladder after transurethral resection (TUR). THP is pigmented and selectively absorbed by bladder tumor cells. In a preliminary study, Uchikoba and associates 14 reported the utility of intravesical instillation of THP in the macroscopic detection of flat malignant lesions, such as CIS. THP is similar to the color of the bladder mucosa, however, which can make discrimination of targeted cells difficult, especially when bleeding or cystitis is present. When THP is absorbed by tumor cells, 69% to 74% localizes to the nuclear surface and is metabolized in the nucleus. 15 Fluorescence from THP in the nucleus can be detected by fluorescence microscopy, which enhances the contrast of malignant lesions to normal bladder mucosa urothelium. Through the use of blue light cystoscopy, enhanced visual contrast would make it much easier for the inspector to discriminate targeted lesions.
The aim of the present study was to evaluate whether the use of THP as a fluorescent dye in endoscopy improves detection of nonmuscle-invasive urothelial carcinoma of the bladder.
Patients and Methods
Patients
Between January 2008 and April 2009, we enrolled (Department of Urology, Sun Yat-sen Memorial Hospital) 48 consecutive patients (mean age, 58.8 years; age range 36–86 years; men, n = 40; women, n = 8) suspected of having primary or recurrent bladder cancer as determined by cystoscopy, cytology, and/or ultrasonography. Inclusion criteria were: Primary or recurrent bladder cancer without recent (<6 months) history of intravesical chemotherapy or immunotherapy, age >18 years, declaration of consent, and no anesthesia risk. Exclusion criteria were: Urethral strictures, detrusor instability, small-capacity bladder, pregnancy, renal failure or liver insufficiency, THP allergy, macroscopic hematuria, or mental health problem.
Chemicals and instruments
THP was obtained commercially from Shenzhen Main Luck Pharmaceuticals Inc. (Shenzhen, China). A 300W xenon short arc lamp (D-Light AF system; Karl Storz, Tuttlingen, Germany) was used for white light illumination, and the blue light for excitation was filtered by a band-pass filter (375–440 nm). Illumination and observation of tissues were performed with a modified endoscope integrated with a long-pass filter (cutoff wavelength, 550 nm) to reduce excitation light and improve the contrast of red fluorescing tumors and surrounding tissue. A foot switch regulated the filter for blue or white light. The optical device allowed a 30-degree or 70-degree angle view.
Clinical procedures
Endoscopy was performed under local spinal anesthesia. The bladder was first assessed carefully by WLC to inspect the dome, posterior bladder wall, right lateral wall, left lateral wall, and trigone. Macroscopic WLC findings based on tissue morphology were documented on a bladder map. Bladder mucosa morphology was classified as normal, papillary, or exhibiting nonspecific inflammation (the latter being hypervascularized, erythematous, erosive, or edematous areas of the mucosa). Then the bladder was completely emptied by catheterization. THP (30 mg, freshly dissolved in 40 mL distilled water) was instilled into the bladder and retained for 15 minutes. After emptying the bladder of THP, it was irrigated with 500 mL physiologic saline.
FC was used to examine the bladder with blue light. FC findings were documented on the same map for each bladder site examined. Cold cup biopsies and/or deep biopsies were taken by standard resection from fluorescent and nonfluorescent areas of the bladder under either blue or white light from all five sites of the bladder wall, regardless of whether the bladder mucosa appeared normal. Tumors were staged and graded according to the 2004 World Health Organization diagnostic criteria by a pathologist blinded to endoscopic findings. CIS lesions were classified as high grade. All adverse events related to the drug were described.
Sensitivity and specificity were calculated according to guidelines of the European Agency for the Evaluation of Medicinal Products (EMEA; CPMP/EWP/1119/98). The study was approved by the local ethics committee and was performed in accordance with the Declaration of Helsinki. All patients provided written informed consent before undergoing the procedure.
Results
After THP uptake, the lesions with much THP uptake in the bladder appear bright orange under white light and produce bright red fluorescence under blue light (Fig. 1), interestingly; minor lesions with a little THP uptake also produce red fluorescence under blue light while obscure under white light (Fig. 2). A total of 238 biopsies from 48 patients were evaluated (Table 1). Tumors were categorized as Ta, T1 + T2, or CIS according to the degree of malignancy as determined by histologic findings. There were a total of 84 malignant specimens, 20 cases of dysplasia, and 134 benign specimens (including hyperplasia of the transitional epithelium, glandular cystitis, and nonspecific inflammation).

Endoscopic images of the bladder after instillation of pirarubicin hydrochloride.
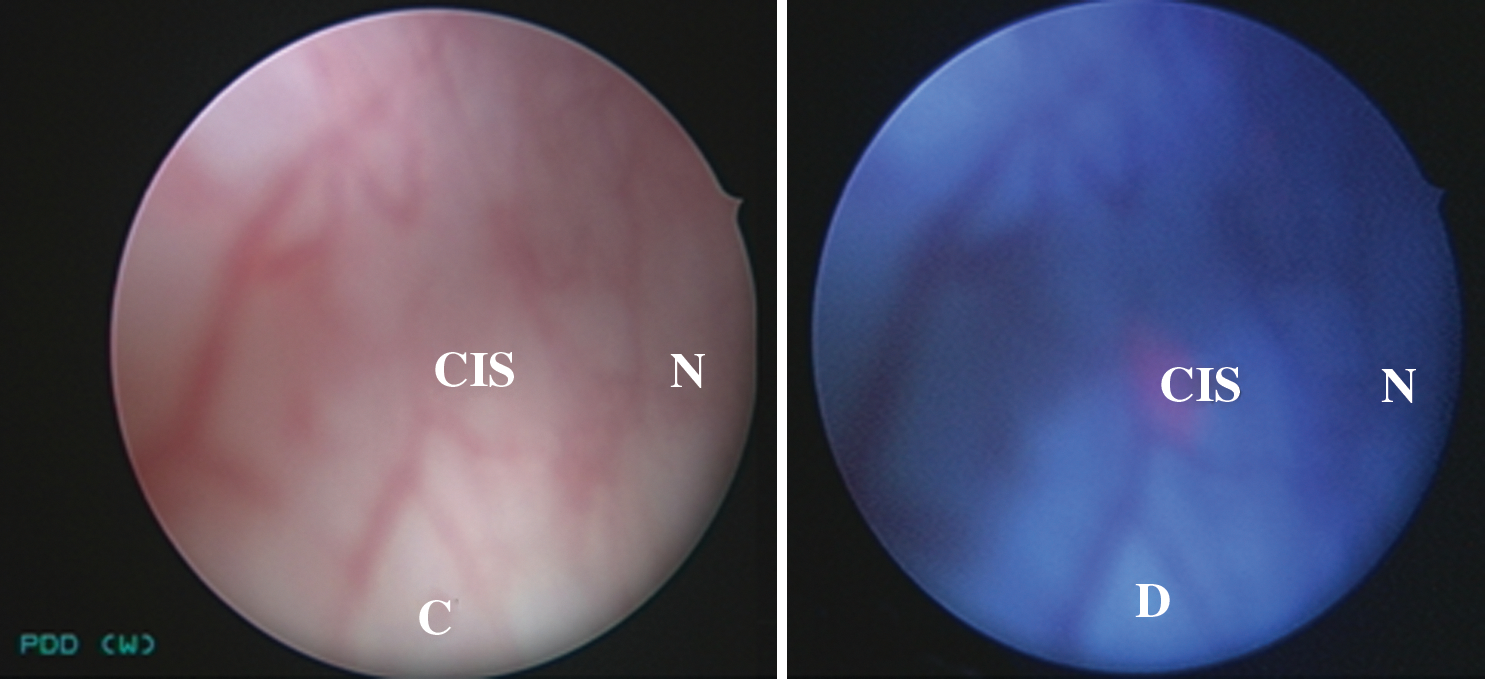
Endoscopic images of the bladder after instillation of pirarubicin hydrochloride. (
THP = (2″R)-4′-O-tetrahydropyranyl doxorubicin, pirarubicin; CIS = carcinoma in situ.
Sixteen malignant lesions in 12 cases were detected only by FC, including three flat malignancies overlooked after THP instillation for WLC (four malignancies in 1 patient, two in 1 patient, and one each in 10 patients); three malignant lesions in 3 patients were missed by FC (Table 2). The sensitivity of overall tumor detection was 96% (81/84) for FC and 82% (69/84) for WLC (Table 3). Six malignancies were classified as CIS. Notably, the sensitivity of FC in detecting CIS was 100%, whereas WLC showed a sensitivity of only 33%; the sensitivity for detection of dysplasia was 90% (18/20) compared with 35% (7/20) for WLC.
FC = fluorescence cystoscopy; WLC = white light cystoscopy.
FC = fluorescence cystoscopy; WLC = white light cystoscopy; CIS = carcinoma in situ.
The specificity of FC was calculated to be 74.7% (115/154) compared with 80.1% (113/141) for WLC. The false-positive rate of FC was 32.5% (39/120) compared with 28.9% (28/97) for WLC. Among 39 false-positive biopsies obtained by FC, 3 were hyperplasia of urothelium; 11 were glandular cystitis; 7 were benign tissue with nonspecific inflammation; 18 were dysplasia. Sensitivity of FC with respect to tumor grading was 92% for low-grade and 100% for high-grade tumors compared with 80% for low- or high-grade tumors for WLC.
Fluorescence remained stable and constant during inspection. No significant systemic side effects or allergic reactions caused by the instillation of THP solution were observed other than a few cases of mild cystitis.
Discussion
Early diagnosis of bladder cancer is crucial to improving treatment outcomes and increasing survival rates. Urinary cytology and conventional cystoscopy with bladder mapping have been the gold standard diagnostic tools for many years. Urine cytology, however, has a sensitivity of less than 60% 16 and cannot provide information regarding the location and extent of the tumor. WLC is reliable for exophytic tumors; however, flat carcinomas (particularly CIS), dysplasia, multifocal growth, and microscopic lesions are much more difficult to detect using this method.
About 15 years ago, the photodynamic agent 5-ALA was first introduced into urology practice, and porphyrin-induced FC has been considered a safe diagnostic method for bladder cancer detection with high sensitivity and considerable specificity. 5,7 –10 5-ALA is unstable at room temperature, needs longer intravesical dwelling time because of its low lipophilicity, and is readily photobleached, so its hexyl ester derivative HAL (more lipophilic, stable at room temperature, less vulnerable to photobleaching, and needs shorter indwelling time) was introduced and is more powerful. Robust evidence from various multicenter, prospective, controlled, or randomized trials on hundreds of patients revealed that photodynamic diagnosis using these agents improves the detection rate of nonmuscle-invasive papillary bladder tumors (Ta-T1 and CIS), and decreases the amount of residual cancer after TUR of the bladder tumor, 17 leading to a reduction in rates of tumor recurrence at 9 months. 18 Up to now, HAL is the sole product that is commercially available in Europe and for which FDA approval is pending in the United States.
In spite of this evidence, PDD cannot be routinely performed because of high start-up expenses (dedicated equipment), cost and availability of fluorescent drugs, and need to plan the procedure in advance. 19 The ideal diagnostic tool for bladder cancer detection and monitoring should be affordable and simple to perform and should provide the highest levels of sensitivity and specificity.
THP is an anthracycline derivative that exerts a stronger antitumor effect than adriamycin. Intravesical instillation of THP after TUR may significantly decrease the recurrence rates of nonmuscle-invasive urothelial carcinoma of the bladder. 20 After absorption by the bladder tumor, THP pigment and anthracene nuclear fluorescence are easily detected. In the present study, papillary and flat lesions were stained orange by THP and easily found macroscopically. Furthermore, inspection under blue light detected additional malignant lesions (especially CIS) by enhancing contrast of abnormal lesions with normal tissues. Dysplasias, which were usually determined to be precancerous lesions, were easily detected as well. THP was taken up by benign lesions including glandular cystitis, hyperplasia, and nonspecific inflammatory urothelia, although fluorescence intensity was low. The sensitivity and specificity of THP uptake for malignant mucosal lesions in our study was 96% and 74.7%, respectively, which is identical to that of previously documented photodynamic diagnosis. 21 Uchikoba and colleagues 14 reported sensitivity and specificity of up to 100% and 97.5%, respectively, using THP for malignant mucosal lesions; however, this difference may be attributed to different samples, diagnostic instruments, and THP dosage and retention time.
THP is quickly and selectively absorbed by tumor cells, 22 and fluorescence intensity is proportional to the level of uptake. In previous studies, THP was absorbed within 3 to 4 minutes, reaching peak absorption in 30 minutes, but retention of THP in the bladder for 5 to 15 minutes using intravesical chemotherapy appears to be a better technique. 23,24 Combining the benefits of preoperative intravesical chemotherapy and enhanced tissue contrast, we injected THP into the urinary bladder for 15 minutes and used the conventional dose of 30 mg, which appears to be the optimal dose with respect to drug efficacy, prevention of side effects, and fluorescence interference.
Protoporphyrin IX fluorescence-PDD exploits the photoactive nature of certain compounds to enhance the visual demarcation between normal and neoplastic tissue. Currently used photosensitizers, such as 5-ALA and its derivative HAL, accumulate preferentially in tumor tissue, with a ratio of around 20:1 compared with normal tissue. The mechanisms are still not fully understood, but studies suggest that accumulation is not from selective uptake by cancerous cells. Rather, 5-ALA is taken up similarly by all cell types, but the processes of conversion and elimination are different in malignant cells, leading to a concentration gradient between neoplastic and normal tissue. 25 For that reason, a relatively long time between drug instillation and FC is needed to obtain adequate concentrations of the photosensitizer. Moreover, fairly rapid photobleaching, the difficult preparation of drug instillation, and high cost limit clinical applicability.
In contrast, THP is quickly and selectively absorbed by tumor cells and does not undergo an intracellular conversion process. Thus, the time between drug instillation and endoscopy is very short and need not interfere with the surgical procedure. THP is commercially available with easy preparation of instillation and low cost. Instillation of THP during the TUR procedure not only improves detection of malignant lesions under white or blue light, but also serves as a preoperative chemotherapy that prevents replantation of tumor cells, which may reduce tumor recurrence and improve treatment outcomes. Although a case of anaphylactic shock induced by intravenous injection of pirarubicin has been reported, 26 early intravesical chemotherapy of pirarubicin with 30 mg after TUR may cause mild or moderate chemical cystitis. including pain with micturation, urinary frequency/urgency, and macroscopic hematuria, 27 but that resolved by conservative management. As we know, a severe adverse side effect such as anaphylactic shock caused by intravesical instillation with THP has not been reported to date.
In the present study, no serious side effects were observed with 30 mg THP intravesical injection, and it demonstrated high sensitivity and specificity for detecting bladder cancer. Thus, we recommend THP instillation to correctly diagnose flat or papillary bladder carcinoma.
Conclusions
THP endoscopy may improve the detection of nonmuscle-invasive urothelial carcinoma of the bladder, especially CIS and flat lesions. Results indicate that THP is a promising fluorescent dye for diagnosis and follow-up of nonmuscle-invasive bladder carcinoma. Moreover, it is inexpensive, easily available, simple to administer, and is associated with few side effects.
Footnotes
Acknowledgments
We thank Ms. Li for language revising assistance for the preparation of this article.
Disclosure Statement
No competing financial interests exist.