
Abstract
Background:
Few studies have addressed the effect of skin-to-stone distance (SSD) on the success of extracorporeal shockwave lithotripsy (SWL). Nevertheless, the effect of the two components of SSD, that is, the fat SSD (FSSD) and nonfat SSD (NFSSD) components, was not previously investigated.
Methods:
In this prospective study, all patients (n = 113) who had single radio-opaque kidney stones and underwent SWL for the first time between January 2006 and June 2007 were recruited. SSD, FSSD, and NFSSD were measured by noncontrast CT scan at 0°, 45°, and 90° and the average was calculated. The outcome was defined as successful (completely stone free or residual fragments ≤3 mm) or unsuccessful (residual fragments >3 mm or complete failure of fragmentation).
Results:
Sixty-nine (61%) patients had successful treatment. On univariate analysis, SSD, FSSD, and NFSSD were significantly lower in the successful group compared with those with unsuccessful outcome (71.9 ± 13.3 vs. 86.2 ± 25.1 mm [p = 0.001], 27.2 ± 10.3 vs. 36.1 ± 17.3 mm [p = 0.011], and 44.7 ± 7.2 vs. 50.1 ± 13.9 mm [p = 0.02], respectively). The muscle component of the NFSSD was also lower in the successful group (21.5 ± 4.1 vs. 25.2 ± 10.0 mm [p = 0.01]). On multivariate analysis, factors that independently predicted treatment success were SSD, stone attenuation, and stone size but not the FSSD or NFSSD.
Conclusions:
Although the total SSD appeared to be a significant predictor of SWL success, its fat and nonfat components did not independently predict the final outcome and only appeared to be important through their contribution to the total SSD.
Introduction
Few studies, mainly retrospective, have addressed the effect of SSD on the success of SWL. 8 –12 Nevertheless, the effect of the two components of SSD (fat SSD [FSSD] and nonfat SSD [NFSSD] components) was not investigated previously. The aim of this research was, thus, to study the relationship between the width of each component and treatment outcome.
Methods
This prospective study was performed between January 2006 and June 2007. All patients who had single radio-opaque renal stones and had NCCT scan as part of their diagnostic work-up were considered for the study. Other inclusion criteria included having SWL as the initial stone treatment. In our institute, the decision to have an NCCT scan versus other imaging modalities such as an ultrasound scan in the diagnostic work-up was generally based on every physician's practice preferences and not on factors related to patients or stones. All patients agreed to participate in this study, which complied with the ethical regulations of our institute.
During the study period, a total of 198 patients with urinary tract stones underwent SWL at our institute. Of those, 116 patients were fit to be included in the study as per the inclusion criteria. Three patients failed to attend during their follow-up; thus, only 113 patients were included in this study. Of these 113 patients, there were 87 men (77%) and 26 women (23%), with a mean age of 41.9 years (range: 18–68 years).
SWL was performed using Dornier Lithotripter S II at a rate of 70 shocks per minute and fluoroscopy was used for stone localization. The lithotripter has a penetration depth of 150 mm and an average focus size of 24 × 38 mm. During the first 100 shocks, the energy level was set at 10% of the maximum level. The energy level was then increased gradually and stepwise to reach 70% to 80% of the maximum level at 1000 shocks and maintained at this level thereafter. In our institute, patients with kidney stones usually receive a maximum of 4500 shockwaves unless the stone has shown evidence of good fragmentation as decided from the intraoperative fluoroscopy at which case the patient receives a smaller number of shockwaves. Patients were instructed to sieve their urine post-SWL and to collect stone fragments for analysis.
Stone size was defined as the greatest diameter on NCCT. The stone Hounsfield density was calculated by dividing the peak HU by the maximum stone diameter (stone size). 13 The average SSD was defined using the same principles as described previously. 8 Briefly, measurements were taken in millimeters at 0°, 45°, and 90° from the stone to the skin on the NCCT, regardless of the stone type and location. The average SSD was then calculated from these readings. The decision to take the average of these three measurements was based on the fact that the lithotripter head is usually placed obliquely with an angle from the vertical line that may vary depending on various factors such as the exact position and body habitus of the patient. Further, using this way to calculate the SSD makes it easier to compare our findings with the other studies in this field that used this methodology.
In the present study, we measured the distance between the skin to the nearest stone surface and not to the center of the stone as previously described. This distance is composed of FSSD and NFSSD components (Fig. 1). The fat component is composed of the peri- and para-renal fat in addition to the subcutaneous fat. The NFSSD is composed mainly of muscles and renal tissues. All these distances were measured at 0°, 45°, and 90° and the average was calculated. In addition, the fat-to-nonfat components ratio was calculated by dividing the FSSD by NFSSD.
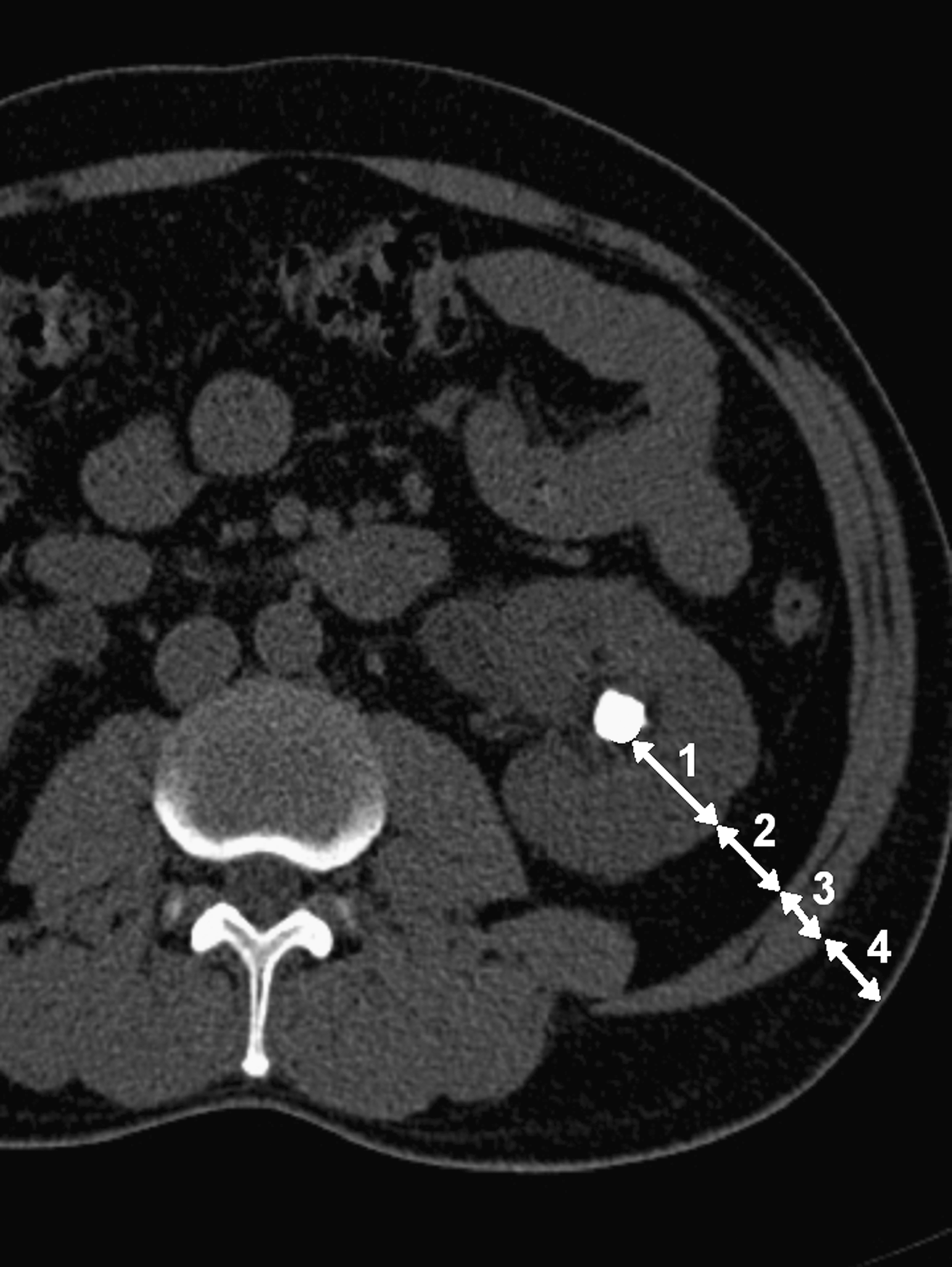
Noncontrast CT demonstrating the measurements of fat and nonfat components of the skin-to-stone distance in a patient with left renal stone. Distance (1) represents renal tissue, (2) peri- and para-renal fat, (3) abdominal muscles, and (4) subcutaneous fat. The fat component was calculated by adding (2) and (4), whereas the nonfat component was calculated by adding (1) and (3). In this demonstration, the measurements of these components were shown only at 45°. Similar measurements were also taken at 0° and 90° and the average was calculated.
The BMI was also measured and calculated by dividing the patient weight (kg) by height square (m2).
Patients' radiological follow-up included plain radiography at 1 day post-SWL. In addition, plain radiography and NCCT were performed at 4 to 6 weeks after SWL. However, all the measurements including the SSD, FSSD, and NFSSD as well as the initial stone size and the residual fragments were obtained from the NCCT.
In the present study, only data related to the first SWL session were collected. The data collected included patients demographics (e.g., age, sex, height, and weight), stone-related characteristics (e.g., size, density, and location including the presence of double-coil ureteral stent), SSD, FSSD, NFSSD, and data related to the SWL procedures and their outcomes.
The patients were categorized according to the final outcome depending on the radiological investigations up to 6 weeks post-SWL. The outcome was defined as successful (completely stone free or residual fragments ≤3 mm) or unsuccessful (residual fragments >3 mm or complete failure of fragmentation). Completely stone free was defined as the lack of any visible stone fragments on NCCT up to 6 weeks after SWL.
Statistical analysis
Statistical analysis was performed using SPSS V15.0 (Chicago, IL). In this study, univariate analysis to compare different variables in the successful and unsuccessful outcome groups was performed using Student's t-test for continuous data and Fisher's exact test for categorical data. Multivariate logistic regression analysis was then performed to determine the significant independent predictors of treatment outcome. The multivariate analysis was used because, oftentimes, some factors that could be significant predictors on univariate analysis may be so through their relations with other factors. The multivariate analysis has the power to exclude such factors and predict the independent predictors. A p-value of <0.05 was considered statistically significant. The results were expressed in mean ± standard deviation.
Results
Of the 113 patients who participated in the study, 69 patients (61%) had successful outcome after the first session of SWL (Table 1). Of them, 47 patients (42%) had complete stone fragmentation and 22 patients (19%) had residual fragments ≤ 3 mm in diameter. The remaining 44 (39%) patients failed the treatment. Thirteen patients (12%) had no sign of fragmentation, whereas the remaining 31 patients (27%) had residual fragments of >3 mm in diameter. There was no difference in the sex or laterality of stones between patients with either successful or unsuccessful outcome (Table 1). In addition, the average number of shockwaves and total energy used in the two groups were not different.
p-Value represents the significance as determined by univariate analysis. For multivariate analysis, please refer to the text.
SD, standard deviation.
The mean SSD for all patients was 77.7 ± 21.1 mm. In patients with successful outcome, the mean SSD was significantly lower than that in patients with unsuccessful outcome (71.9 ± 13.3 vs. 86.2 ± 25.1 mm, p = 0.001). Similarly, both FSSD and NFSSD of SSD were lower in the first group (27.2 ± 10.3 vs. 36.1 ± 17.3 mm [p = 0.011] and 44.7 ± 7.2 vs. 50.1 ± 13.9 mm [p = 0.02], respectively). The FSSD/NFSSD ratio in the two groups did not show any significant difference (Table 1). Comparing the muscle width in the two groups revealed a lower value in the successful group (21.5 ± 4.1 vs. 25.2 ± 10.0 mm, p = 0.01). However, there was no significant difference in the renal tissue width between the two groups as shown in Table 1.
The mean BMI for all patients in the study was 26.2 ± 4.7 kg/m2. Similar to SSD, BMI was also significantly lower in patients with successful treatment (25.5 ± 4.7 vs. 27.4 ± 3.9 kg/m2, p = 0.02).
On univariate analysis (Table 1), other factors that affected the treatment success include stone size, stone HU density, presence of double-coil stent, and stone location. As demonstrated in Table 1, compared with stones in other locations, stones in the lower pole were more likely to fail the SWL. This difference in outcome was not due to differences in SSD, FSSD, or NFSSD as shown by the lack of any statistical significant difference in these variables between the lower pole stone compared with stones in other locations when grouped together (78.5 ± 15.2 vs. 77.0 ± 19.3 mm [p = 0.09], 31.5 ± 12.4 vs. 30.4 ± 16.9 mm [p = 0.10], and 46.4 ± 12.1 vs. 46.9 ± 9.7 mm [p = 0.19], respectively).
On multivariate analysis of all the factors that significantly determined treatment outcome on univariate analysis (Table 1), the factors that independently predicted treatment success were SSD [β: − 0.061, SE: 0.038, Exp(β): 0.932, p = 0.032], stone HU density [β: 0.134, SE: 0.059, Exp(β): 1.144, p = 0.023], and stone size [β: − 0.035, SE: 0.029, Exp(β): 0.975, p = 0.04]. Using a similar logistic regression model but replacing the SSD with its two components, that is, fat and nonfat components, had shown that neither the fat nor the nonfat components of the SSD independently predicted the final outcome (p = 0.12 and p = 0.31, respectively).
Of the 100 patients who had either complete (n = 47) or partial (n = 53) stone fragmentation, stone analysis data were available in 74 patients. The stone composition was as follows: calcium oxalate (n = 41), calcium oxalate and calcium phosphate (n = 18), calcium phosphate only (n = 11), uric acid with minor elements of calcium oxalate (n = 2), and struvite (n = 2).
Most patients (104 patients; 92%) tolerated the procedure well with sedation, and the rest had general anesthesia.
Discussion
The present study addressed directly the effect of fat and nonfat components of SSD on the treatment outcome of SWL and has demonstrated that none of these components independently predicted the final outcome of SWL but rather contributed to the total SSD, which was shown to be a significant independent predictor of the SWL success.
Few studies have addressed the effect of SSD on the success of SWL. 8 –11 For instance, El-Nahas and colleagues, 11 in one of the very few prospective studies in this field, demonstrated that SSD was a significant predictor of SWL failure based on univariate (but not on multivariate) analysis. Similar findings were confirmed by multivariate analysis in retrospective studies. 8,9,12 Nevertheless, the effects of various components of SSD (FSSD and NFSSD) were not investigated previously in the clinical setup.
In vitro studies have demonstrated that the propagation of sound waves in a particular media is affected by that media. 14,15 As the sound waves pass through a medium, some of its energy gets absorbed and, hence, attenuated. The degree of attenuation of a sound wave with certain frequency depends predominantly on the macromolecular composition of the media. 15 Among the main components of SSD, muscles result in the highest and the kidney tissue in the lowest degree of shockwave absorption, with the fat being in the middle. 14 Despite these in vitro variations, it is not known if these differences in the propagation of shockwaves in the fat and nonfat components of SSD would affect the final outcome of SWL in the clinical setup. This point may be clinically important as the proportion of fat to nonfat components is variable among different individuals. For example, in athletes, because of the bulky muscles, the proportion of nonfat component is higher than that in obese patients who has a higher proportion of fat, although both may have the same SSD. Therefore, if both fat and nonfat components have different effect on shockwaves, the treatment success may differ in the athletic and obese patients with the same SSD. Similar disproportionate relationship between fat and nonfat components may also be found in children and patients with hepatic and renal failure or even among different races such as Asians when compared with Caucasians. 16 Hence, it is important to investigate the contribution of various components of the SSD to the final outcome of SWL. Obviously, one way of approaching this question would be to compare the treatment success in a cohort of obese and athletic patients with matched SSD and stone characteristics. Nevertheless, in the present study, the fat-to-nonfat ratio in our patients has ranged from 0.31 to 1.79, indicating that we have included patients with both high (more obese) and low (more athlete) fat-to-muscle ratios.
One of the very few studies that attempted to address the effect of body fat content on SWL outcome was the one reported by Akay and colleagues. 17 The authors investigated the effect of BMI, body fat percentage, and body fat mass on SWL outcome. However, the last two parameters were calculated using BMI, which is an indirect measure of the body fat content and distribution; hence, these parameters may be false indicators of the actual body fat content in some patients such as athletes, children, and those with hepatic or renal failure. Further, there was no attempt to investigate the effect of the nonfat component of the SSD on treatment outcome.
In the present study, SSD was defined as the distance from the skin to the stone surface and not to the stone center as previously described. 8 This appears to be more appropriate, especially in the present study, because the distance from the stone surface to the stone center was excluded from the measurement of the NFSSD, which, therefore, included only muscle and kidney tissues. The inclusion of this distance would have been inappropriate in the present study because this distance, which was composed of the stone material, has already been accounted for when considering the stone density as a predictor of SWL outcome. Other issue related to calculating the SSD is the fact that once the shock head was placed onto the patient's flank, there would be a slight compression of the tissues in that axis, which may result in slight decrease in the subcutaneous fat width and probably also in the muscle width but to a lesser extent. However, this would be difficult to measure unless patients were CT scanned during SWL procedure.
In the present study, the renal width was slightly lower in the successful group but this did not reach statistical significance. Whether this indicates that the muscle is the main component that contributes to the total effect of the nonfat component is difficult to ascertain from the present study. One possible explanation could be related to the fact that the renal width was measured as the distance from the renal capsule to the stone surface. Obviously, a small portion of this distance was composed of little amount of urine located between the renal tissue and the stone. This distance would have been difficult to measure and probably varies slightly from time to time with the occasional movement of the stone. The inclusion of this urine distance in the calculation of renal width might have caused the amelioration of the calculated effect of renal tissues on the shockwaves. However, further research is required in this field.
In the present study, in addition to SSD, other factors that independently predicted SWL success included stone Hounsfield density and stone size. This was in agreement with the findings of other researchers who also used multivariate analysis to determine the independent factors that affect the SWL final outcome. 9 –11
In the present study, 12% of the stones did not show any evidence of fragmentation after the first SWL session. Eight of these 13 stones were composed of calcium oxalate as proven by stone analysis after subsequent SWL sessions and the remaining 5 stones had a high stone HU density (>106 HU/mm) and long SSD (>119 mm). These findings in this particular group of patients were in agreement with the findings of the present study and other studies in this field. 9,11,12
In conclusion, although we have demonstrated that the total SSD was a significant independent predictor of the SWL success, its fat and nonfat components did not independently predict the final outcome in the clinical setup and only appeared to be significant through their contribution to the total SSD.
Footnotes
Disclosure Statement
No competing financial interests exist.