
Abstract
Purpose:
To report our experience in the laparoscopic extravascular management of the nutcracker syndrome.
Patients and Methods:
Three patients (two men and one woman) between the ages of 20 and 35 years (mean 25.7 y) underwent laparoscopic extravascular stent placement in the left renal vein for management of the nutcracker syndrome that is associated with severe recurrent gross hematuria and left gonadal vein varices. The postoperative follow-up was 16 to 37 months (mean 25.3 mos).
Results:
All patients met the criteria for establishing the diagnosis of the nutcracker syndrome. Ultrasonography, CT, and MRI revealed visible entrapment of the left renal vein between the superior mesenteric artery and aorta. Bleeding from the left ureteral orifice was detected by urethrocystoscopy and ureterorenoscopy. We attempted a novel laparoscopic method to manage this anatomic anomaly. No complications occurred during surgery. Total relief was achieved in two men without a relapse of symptoms, and abnormalities were not found in the results of the urine test. There is partial relief in a 20-year-old woman because of microhematuria after the operation.
Conclusions:
The indications for surgical management with the nutcracker syndrome depend on the severity of the symptoms, and laparoscopic extravascular stent placement in the renal vein is a feasible approach for reestablishing free renal venous outflow. This slightly invasive treatment can eliminate the symptoms of the condition. Longer follow-up and more experience are necessary to make conclusions about its feasibility in contemporary practice, however.
Introduction
The most frequently reported procedure is transposition of the LRV. 1,10 –13 Barnes and associates 3 first reported extravascular stent placement performed by open surgery in 1988. Scultetus and coworkers 14 gave the first brief description of this laparoscopic technique in a single patient in 2001; however, the details of the technique were not provided in the report. To our knowledge, we present the first detailed serial report of a laparoscopic extravascular renal vein stent placement for nutcracker syndrome to relieve the obstruction, and we report our experience of the extravascular treatment.
Patients and Methods
Three patients (two men and one woman) between 20 and 35 years old (mean 25.7 y) had received a diagnosis of nutcracker syndrome between 2006 and 2009. The leading symptom was left-sided varicocele in two and gross hematuria in one, with other symptoms such as left flank pain and orthostatic proteinuria. The woman was anemic with a hemoglobin level of 8.7 mg/dL; the other patients had normal hemogram findings.
A diagnostic algorithm was performed to exclude any other pathologic findings and to confirm the presence of the nutcracker syndrome. Urine cytology, ultrasonography, intravenous urography, CT angiography (CTA), MRI, left renal arteriography, urethrocystoscopy, and ureterorenoscopy were performed. Ultrasonography showed the inner diameter ratio between the hilar portion and the aortomesenteric portion of the LRV was more than 3. CTA demonstrated entrapment of the LRV between the aorta and the SMA with proximal dilation (Fig. 1). Renal MRI showed severe dilation of the LRV. The delayed venous phase of the left renal arteriogram demonstrated abnormal dilation of the LRV and engorged gonadal vein varices (Fig. 2). The last step for confirmation of the nutcracker syndrome was bleeding from the left ureteral orifice that was detected by urethrocystoscopy and ureterorenoscopy. Based on the above findings, three patients with persistent gross hematuria, severe left spermatic vein varices, and intermittent left flank pain were scheduled for surgery (Table 1).

CT angiography demonstrated visible entrapment of the left renal vein (LRV) between the aorta (AO) and the superior mesenteric artery (SMA) with proximal dilation of the LRV.

Delayed venous phase of a left renal arteriogram shows: (
US = ultrasonography; LRV = left renal vein; CT = computed tomography angiography; MRI = magnetic resonance imaging; LERVS = laparoscopic extravascular renal vein stent placement; ePTFE = polytetrafluoroethylene.
The patients were placed in the lateral decubitus position under general anesthesia. A standard four-port transperitoneal technique was used. Incision of the splenocolic ligament followed to mobilize the spleen along with the colon. Careful dissection should be performed for the prevention of injury to the spleen and venous collaterals.
The fibrous bundle between the aorta and SMA was divided and the LRV was freed. Intraoperatively, the renal vein became flat when the SMA was elevated, and the proximal renal vein was found to be engorged when we put down the artery. This laparoscopic observation further confirmed the nutcracker syndrome. Whether the left gonadal vein, adrenal central vein, and lumbar veins were preserved or transected depended on different situations.
An externally reinforced ePTFE (polytetrafluoroethylene) graft (REF F4008, Bard Peripheral Vascular, Inc.) of 8 mm diameter was selected to form an external stent around the LRV to relieve the compression. Intraoperatively, we estimated and cut the graft to an appropriate length to fit between the inferior vena cava and the gonadal vein or longer. The graft was wrapped around the renal vein and sewn together at each ring (Fig. 3). The stent was then fixed to the adventitia of the abdominal aorta to prevent potential displacement. We sewed the vasculoneural sheaths around the SMA to fascia with 4.0 polyglactin suture.

Intraoperative photograph demonstrates the graft wrapped around the renal vein.
The follow-up period was 16 to 37 months (mean 25.3 mos).
Results
All patients met the criteria for establishing the diagnosis of the nutcracker syndrome. Diagnostic imaging, such as ultrasonography and CT, revealed entrapment of the LRV between the SMA and the aorta. In addition, surgery revealed visible entrapment of the LRV between the aorta and the SMA with proximal dilation. No complications occurred during the laparoscopic procedure. The patients recovered from the operation without complication and were discharged from the hospital on postoperative day 5.
In the 16 to 37 months (mean 25.3 mos) of follow-up, color Doppler ultrasonography showed that the blood outflow was smooth, the inner diameter and flow velocity of the aortomesenteric portion of the LRV were both decreased, and the gonadal vein varices had diminished in diameter, without any clot formation or stenosis (Figure 4). Total relief was achieved in two men without a relapse of symptoms, and abnormalities were not found in the urine test. Partial relief occurred in a 20-year-old woman; she was asymptomatic and free of gross hematuria but had microhematuria during the 20 months since the operation (See Table 1.).
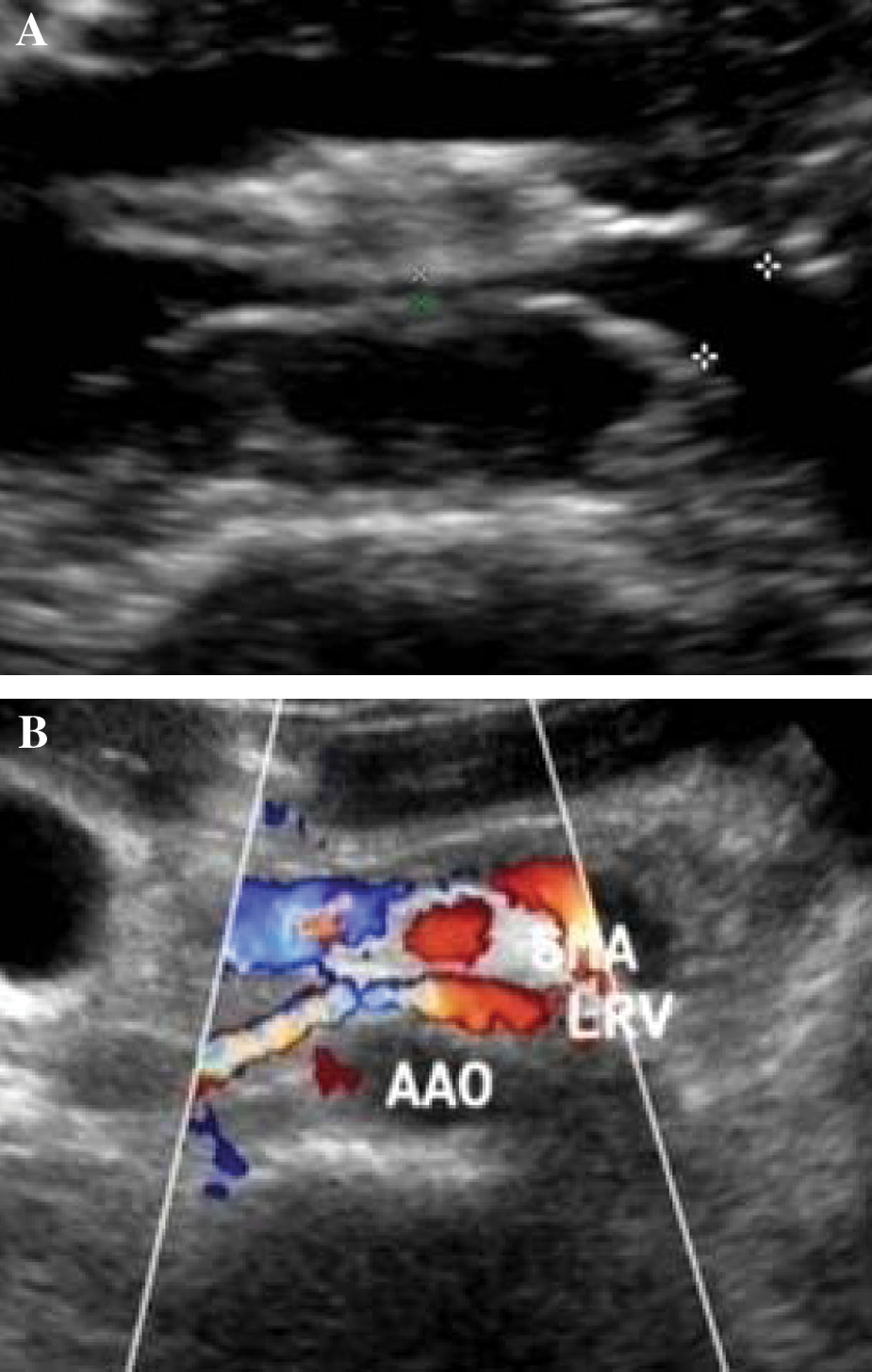
(
Discussion
Nutcracker syndrome is caused by abnormal compression of the LRV between the abdominal aorta and SMA where it passes through the fork formed at the bifurcation of surrounding arteries. It is proposed that an abnormality within the configuration of the origin of the SMA from the aorta induces the congenital cause of this syndrome. 5,12,15 Patients with the syndrome typically present with gross or microscopic hematuria, with or without left flank pain, orthostatic proteinuria, flank and abdominal pain, leftsided varicocele, and chronic fatigue.
The primary diagnostic test should therefore be the clinical examination. Doppler ultrasonography can be used as the diagnostic test in patients with suspected nutcracker syndrome. 2,16 –18 The sensitivity and specificity of color Doppler ultrasonography has been reported as 78% and 100% for diagnosis of the nutcracker syndrome. 19 Zhang and coworkers 16 noted that the inner diameter ratio between the hilar portion and the aortomesenteric portion of the LRV is more than 3. Recently, Doppler ultrasonography with color flow has improved functional diagnostic capabilities by showing the blood flow velocity of the LRV, 20 and the acceleration is more obvious after standing for 15 minutes, which is more than 100 cm/s. 16
Meanwhile, CTA is noninvasive and has excellent diagnostic yield. 2,21 In recent years, it has become the investigation of choice in many centers. Bleeding from the left ureteral orifice could be detected by urethrocystoscopy and ureterorenoscopy. 5,22 Stenosis is not always well highlighted by angiography. 7 In fact, the final diagnosis should depend on intraoperative visible entrapment of the LRV, so our laparoscopic surgery is carried out not only as a treatment procedure but also as an auxiliary examination.
The indications for surgical treatment with the nutcracker syndrome continue to be debated. 23,24 We are cautious about the indications for surgical treatment, especially for adolescents and children, because of the occurrence of spontaneous resolution of the nutcracker syndrome by physical development. In our series, it depends on the severity of the symptoms. Mild and tolerable symptoms can be managed conservatively. Main indications, including significant recurrent gross hematuria, severe flank pain, and severe left gonadal vein varices should necessitate surgery. 1,4,16,17,25
Once the diagnosis has been reached, treatment may be considered to improve the symptoms. Vascular bypass procedures, renal autotransplantation, and nephropexy have been performed successfully. Currently, open surgery for management of the nutcracker syndrome has been focused on LRV transposition. In a series of eight patients, excellent outcomes with an 87.5% success rate were reported by Hohenfellner and colleagues. 1 Shokeir and associates 26 performed autotransplantation of the left kidney with satisfying results. The left kidney was reimplanted into the left iliac fossa, and hematuria ceased in all patients. Simply nephropexy with excision of varicosities has become the last choice, because it failed to address the primary pathologic finding. 2
All of these therapeutic options have been performed with open surgery. These methods resolve the symptoms but are relatively invasive. More recent reports raise enthusiasm for endovascular treatment modalities for the nutcracker syndrome. Although endovascular stent placement is a simple and attractive option, it causes venous thrombosis, 14 and patients need long-term antiplatelet therapy. 8
Currently, laparoscopic surgery for management of the nutcracker syndrome has evolved. 14,27,28 Application of laparoscopic extravascular stent placement for the nutcracker syndrome has been limited. Only one such case has been described in English published reports by Scultetus and coworkers 14 in 2001. The details of the technique were not provided in the report.
The stents have been used extensively, and results have been optimistic. Open extravascular stent plcement was described first by Barnes and associates. 3 The novel laparoscopic method to manage this anatomic anomaly was selected because it avoids the high risk of the more complex reconstruction of venous bypass. Some technical points should be emphasized. For patients who have passed puberty with severe gross hematuria, surgery should be early to avoid alteration in the blood vessel architecture. Considering these facts and the previously confirmed finding that renal venous outflow obstruction is caused by an abnormal branching of the SMA, we chose this method. Although intravascular and open surgical interventions are effective, the laparoscopic extravascular stent placement is minimally invasive and makes allowance for the next potential treatment. For young patients without left gonadal vein varices, the graft was fixed between the inferior vena cava and left gonadal vein. Patients with a thick gonadal vein could be candidates for simultaneous surgery. Excessive fibrous tissue found at the origin of the SMA, which may contribute to the compression of the LRV, needs to be excised for adequate decompression of the LRV. 2 In general, we transect the left adrenal central vein to facilitate surgical exposure and to fix the graft. Meanwhile, we should try to preserve the left gonadal vein unless there is difficult exposure of the left renal vein.
Postoperative drug treatment is an important issue, but no guidelines for drug therapy exist. 7,14 We only gave patients fluindione to avoid postoperative bleeding, and no heparin was used.
It is a straightforward procedure with an acceptable risk of complications. Actually, this may justify the use of laparoscopic extravascular techniques as a feasible alternative approach in the management of the nutcracker syndrome in the future. 11 Longer follow-up and more experience are necessary to make conclusions about its feasibility in contemporary practice.
Conclusions
For patients who need surgical treatment for the nutcracker syndrome, laparoscopic extravascular stent placement in the renal vein is a feasible approach for reestablishing free renal venous outflow. This slightly invasive treatment can eliminate the symptoms of the condition. In some cases, however, microhematuria may persist despite the removal of the obstruction of the left renal vein. Further studies should report if this method can be accepted and if such an approach has adverse effects.
Footnotes
Acknowledgments
We thank Drs. Li-jun Wan and Yan-yu Tong from the Department of Urology, Qu Zhou People's Hospital, Zhejiang, China, and Dr. Weixing Zhang from the Department of Urology, Shao Xing Second People's Hospital, Zhejiang, China, for collaboration in the study and their outstanding illustrations.
Disclosure Statement
No competing financial interests exist.