
Abstract
Objectives:
The aim of this study was to determine the impact of percutaneous nephrolithotomy (PCNL) and tract dilatation methods on global and regional renal function using quantitative single-photon emission computed tomography (QSPECT) of technetium-99m–dimercaptosuccinic acid (99mTc-DMSA).
Methods:
Seventy-five patients undergoing PCNL between May 2008 and April 2009 were included in this randomized study. Of the 75 patients, 50 were evaluated by QSPECT of 99mTc-DMSA examinations before and at 3 to 6 months after surgery. This group of patients were categorized into three groups according to the dilatation technique used: group I (balloon dilator, n = 12 [24%] patients), group II (metal dilator, n = 14 [28%] patients), and group III (Amplatz dilator, n = 24 [48%] patients).
Results:
Of 50 renal units, new focal cortical defects on 99mTc-DMSA scan were seen in nine patients (18%). In six of these kidneys the site of focal defect corresponded to the access site for tract formation during PCNL (two in group II and four in group III). Total relative uptake and total area of treated kidney, for the entire group, increased from 42.2% and 42.3% preoperatively to 44.12% and 43.9% postoperatively. There was no statistically significant differences between the groups for total uptake and area of the treated kidneys before and after the procedure (p > 0.05 for each parameter).
Conclusions:
QSPECT of 99mTc-DMSA confirms that renal function is preserved or often improved after percutaneous stone removal, and nephrostomy tract dilatation methods have similar effects on renal function.
Introduction
The postoperative measurements of renal function indicate that patients tolerate PCNL well, but the immediate effects on renal function are unknown. In clinical practice, technetium-99m–dimercaptosuccinic acid (99mTc-DMSA) scintigraphy, a noninvasive procedure, has been used to evaluate the impact of various pathological processes on the renal cortex, including cortical functional integrity and quantitation of differential renal function. 5 Planar and quantitative single-photon emission computed tomography (QSPECT) techniques have been used for measurement of the percentage uptake of injected radioactivity by the kidneys. QSPECT measurement of DMSA uptake by the kidneys is a reproducible method that can reliably be used to monitor serial changes in individual renal function. 5 –8 To our knowledge, QSPECT of 99mTc-DMSA has not been used previously to the compare the effects of tract dilatation methods on renal function. In this study, we prospectively investigated the impact of PCNL and most commonly applied dilatation techniques on renal function and morphology in chronic situations using the QSPECT of 99mTc-DMSA.
Patients and Methods
Patients
Seventy-five patients undergoing PCNL between May 2008 and April 2009 were included in this randomized study. Patients were randomly divided into three groups according to the dilatation technique used: group I (balloon dilator, n = 25 patients), group II (metal dilator, n = 25 patients), and group III (Amplatz dilator, n = 25 patients). Of the 75 patients, 50 patients (12 [24%] in group I; 14 [28%] in group II; and 24 [48%] in group III) were evaluated by QSPECT of 99mTc-DMSA examinations at 1 day before and at 3 to 6 months after surgery. The remaining patients were either lost to follow-up or assessed elsewhere because of the distance to our center. The indications for PCNL included a stone burden of ≥2 cm (≥1.5 cm for lower pole stones) in length and failure of extracorporeal shockwave lithotripsy (SWL) treatment.
Surgical technique
All procedures were performed with the patient under general anesthesia. A 6F ureteral catheter is placed, and the bladder is drained with a 16F Foley catheter. After ureteral catheter insertion, patients were placed in the prone position and percutaneous access was achieved under fluoroscopic guidance using an 18-gauge needle and guidewire. Tract dilatation was accomplished using Amplatz, metal, or balloon dilators of up to 28F or 30F. Fragmentation and stone removal were accomplished in all patients using pneumatic or ultrasound energy and retrieval graspers through rigid 26F nephroscopes. A holmium laser and nitinol basket catheter were used through flexible nephroscopes for locations unreachable using the rigid instruments. Stone clearance was determined by a combination of fluoroscopy and rigid or flexible nephroscopy at the end of the procedure, sometimes with a plain radiograph or CT postoperatively if there was no confidence in the intraoperative assessment. The operations were completed when residual fragments were not detected on fluoroscopic imaging and rigid or flexible nephroscopic control. Patients with postoperative residual fragments of <4 mm were accepted to be stone free (clinically insignificant residual fragments). After completion, 16F reentry catheter or, alternatively, an 18F Foley catheter as nephrostomy tube was inserted in all patients.
Data analysis
Patient demographics, stone characteristics, operative findings, including size of tract, using devices, tract number, operative time, time to access the collecting system, and fluoroscopy time, success rate, complications, and preoperative and postoperative QSPECT of 99mTc-DMSA scan findings were documented in detail and compared in each group. Statistical analysis was performed using the chi-square test and Student's t-test with p < 0.05 considered significant.
Results
Fifty patients (37 men and 13 women) with a mean age of 43.6 years (range 14–67 years) were evaluated prospectively for any alteration of renal morphology and function after endourologic treatment for nephrolithiasis. PCNL was performed on 22 right and 28 left kidneys. Mean stone burden was 38.1 mm. There were no differences between the three groups in age, sex, stone burden, and laterality. Table 1 lists patient demographics and stone characteristics.
PCNL was performed using a single tract in 44 patients and two tracts in 6 patients (1 in group I, 2 in group II, and 3 in group III). Of the 56 access tracts, inferior caliceal access was created in 29 patients, middle-posterior tracts in 16, and superior caliceal tracts in 11 (supracostal in 3). The time for tract creation from needle puncture to establishment of the tract for lithotripsy was usually <15 minutes and it was similar for each group. There were no major complications and deaths in our series. The majority of the complications were pain, bleeding, urinary leakage after removal of the nephrostomy tube, and postoperative fever. No patient (0%) in group I, but one patient (7.1%) in group II and two patients (8.4%) in group III needed blood transfusion. The stone-free rates after PCNL was 91.2% in group I, 85.7% in group II, and 87.5% in group III. These rates increased to 100%, 92.9%, and 91.7% for groups I, II, and III, respectively, after a second intervention (shockwave lithotripsy and flexible ureterorenoscopy). Mean operative time, fluoroscopic screening time, nephrostomy removal times, and hospitalization times were similar for each group (p > 0.05 for each parameter). Perioperative and postoperative findings are summarized in Table 2.
QSPECT of 99mTc-DMSA scan was performed at a median time of 4 months after the procedure (mean 4.6 months, range 3–6 months). Of 50 renal units, new focal cortical defects on 99mTc-DMSA scan were seen in nine patients (18%). In six of these kidneys the site of focal defect corresponded to the access site for tract formation during PCNL (two in group II and four in group III). Total relative uptake was preserved in 37 (74%) patients. A change in renal function was defined greater than a 3% increase or decrease in the differential function from the preoperative measurement. Five (one in group I, two in group II, two in group III; 10%) patients had a decrease in renal function (Fig. 1), and an improvement in renal functions occurred in eight (two in group I, two in group II, four in group III; 16%) patients (Fig. 2). Total relative uptake of treated kidney increased from 42.2% to 44.1% and total area of treated kidney increased from 42.3% to 43.9% postoperatively, for the entire groups. There were no statistically significant differences between the groups for total uptake and area of the treated kidneys before and after the procedure (Table 3, p > 0.05 for each parameter). Mean creatinine before PCNL in these patients was 1.19 ± 0.46 mg/dL (0.9–1.7) compared with 1.18 mg/dL (0.7–1.5) by the end of the follow-up period with no statistical significance (p > 0.05). Postoperatively, creatinine levels reached normal values (<1.5 mg/dL) in these patients and they were discharged home with stable creatinine levels. The mean creatinine levels and glomerular filtration rate (GFR) were similar in the three groups pre- and postoperatively. The number of patients with hypertension before PCNL was five and by the end of follow-up there was no new onset hypertension.
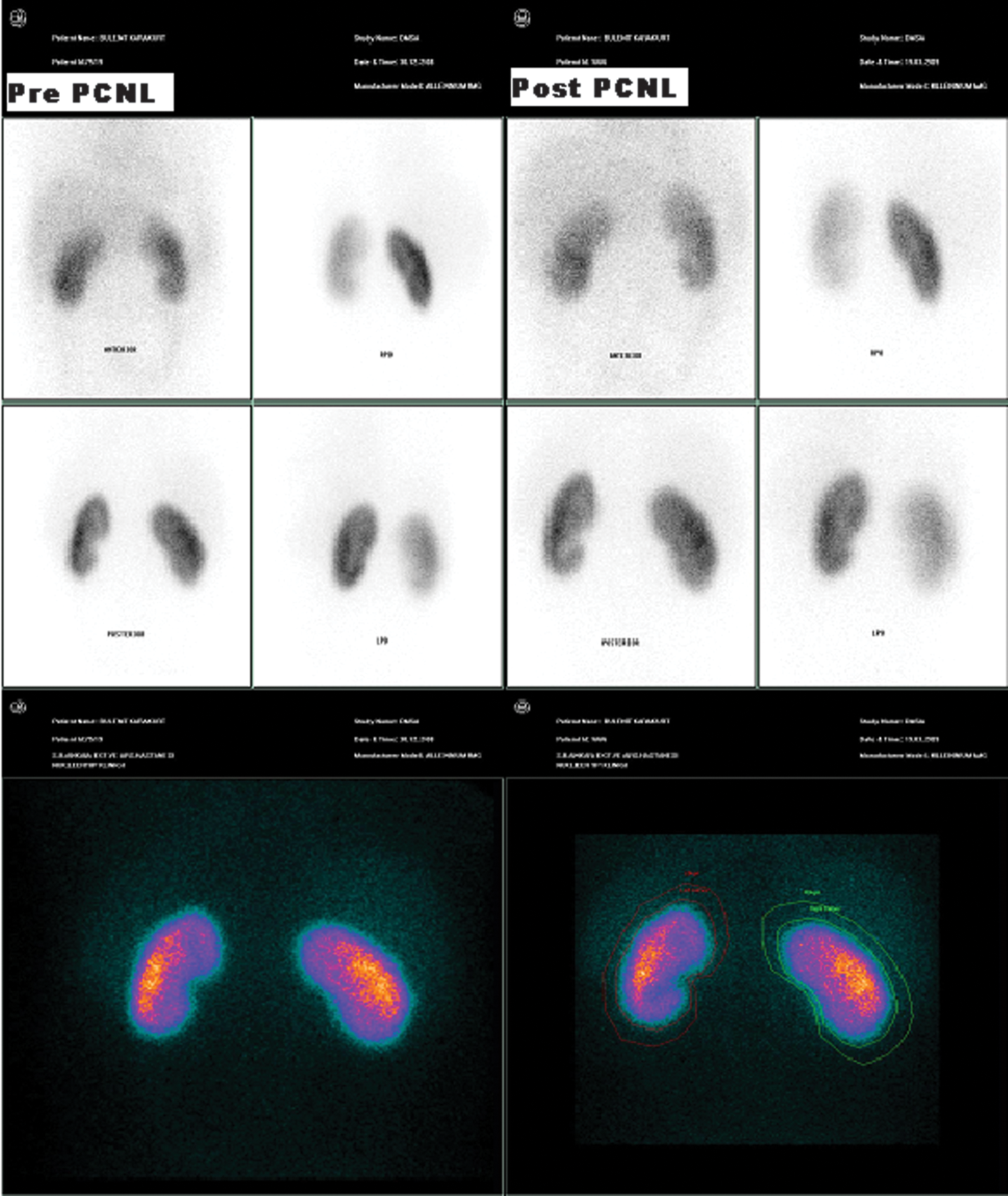
Preprocedure 99mTc-DMSA scan showing posterior-inferior scar in left kidney. Decreased uptake is seen in the lower pole corresponding to the location of the stone. Scan at 3 months after left PCNL and right SWL shows persistent scar, without any new scar formation. LPO = left posterior oblique; PCNL = percutaneous nephrolithotomy; RPO = right posterior oblique; SWL = extracorporeal shockwave lithotripsy; 99mTc-DMSA = technetium-99m–dimercaptosuccinic acid.
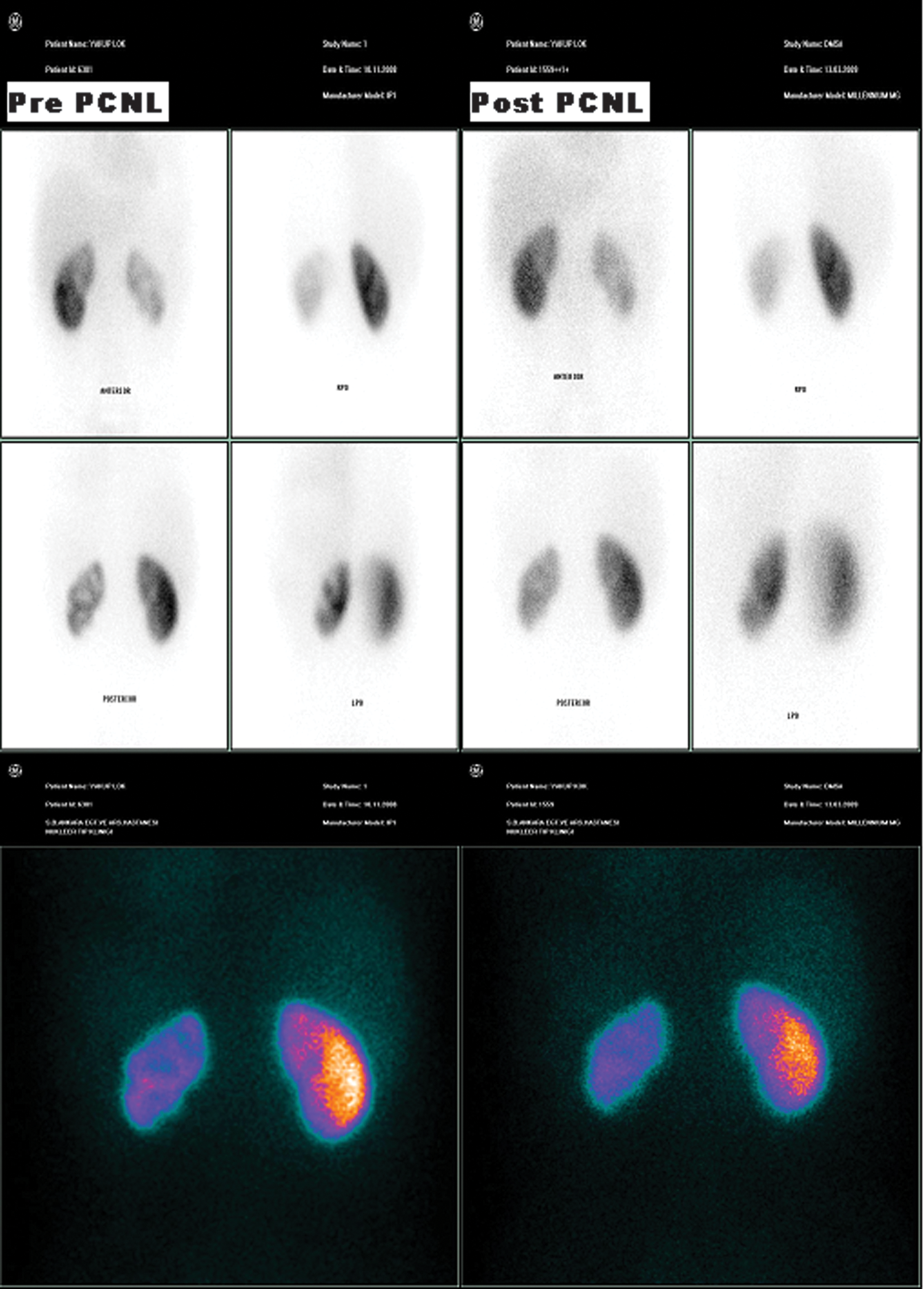
Patient with pretreatment radionuclide abnormality. These DMSA scans before and after PCNL show photopenic renal parenchyma secondary to pelvicaliceal calculus causing caliectasis and cortical thinning and scarring. Scan at 4 months after left PCNL shows improvement in renal uptake, without any new scar formation.
Discussion
Goodwin and associates 9 first described percutaneous nephrostomy in 1955. However, percutaneous renal surgery became an acceptable technique in the early 1970s owing to the pioneering work of Stables et al. 10 The maximal stone clearance with nephron preservation is the primary objective in the treatment of renal calculi with this technique. The postoperative measurements of renal function indicate that patients tolerate PCNL well, but the immediate effects on renal function are unknown. To determine the deleterious effects, if any, of PCNL and tract dilatation methods on renal function, we opted to use QSPECT of 99mTc-DMSA to assess our patients prospectively. To our knowledge, QSPECT of 99mTc-DMSA has not been used previously to the compare the effects of tract dilatation methods on renal function.
The QDMSA study is a reproducible method for monitoring serial changes in individual renal function. It is a noninvasive way to measure the functioning renal-cortical volume. 7 99mTc-DMSA binds the proximal renal tubules similarly to 99mTc–glucoheptonate, resulting in imaging of the renal cortex without effective assessment of renal perfusion or glomerular filtration. 11 Previous investigators have evaluated the effect of SWL and percutaneous and open renal surgeries for renal calculi on renal function, using 99mTc-DMSA. 7,11 –15 Morey et al, 13 in their series, used 99mTc-DMSA scans and demonstrated a relative decrease in renal function after anatrophic nephrolithotomy for staghorn calculi, although it was probably not significantly different statistically. Several studies have evaluated the renal parenchymal effects of SWL using 99mTc-DMSA renal scan. Scarring has been observed in kidneys with calculi treated with SWL at about 3 months after treatment, the degree of scarring depending on the number of shockwaves administered. However, some of these lesions have been found to be reversible. 14,16,17 The use of 99mTc-DMSA scans to assess parenchymal damage after SWL in children was initially reported by Lottmann et al. 17 The authors demonstrated SWL to be a safe modality with no permanent sequelae in children. Renal parenchymal injury, as evidenced by enzyme markers and 99mTc-DMSA scan, may occur in the early period after SWL but has been shown to be reversible with time.
There is a lack of quantitative knowledge regarding the effect of PCNL on global and regional kidney function. Early experimental studies carried out in dogs did not reveal any significant alteration in the morphology or function of the kidney attributable to PCNL. 18 Subsequent studies assessing the effect of PCNL on renal function and growth have found no significant alterations postoperatively. 19 Mor et al 20 performed radioisotope scans on 10 children before and after PCNL and found no change in differential function and no evidence of significant scarring. Moskovitz and colleagues 7 measured the effect of PCNL on renal function in adult patients using SPECT measurement of DMSA uptake by the kidneys. Although no significant alteration of global uptake was noted, the total functional volume of the treated kidney was decreased slightly. Interestingly, regional assessment revealed a statistically significant decrease in the functional volume at the PCNL site of entry. In another series, Dawaba et al performed 99mTc-DMSA scans to detect renal scarring and 99mTc-DTPA scans to determine selective glomerular filtration rates after PCNL in 65 children (72 renal units). 21 There was no evidence of renal scarring in any renal unit, and stabilization or improvement of selective glomerular filtration rate was observed in all but four renal units. Three of these four units showed improvement over time.
Although these studies were considerably relieved to note the absence of cortical scars at the access sites in their patients, in view of the possibly more sensitive quantitative SPECT, DMSA scan showed some local functional loss at the site of entry. 19 A single PCNL procedure produces a small but permanent parenchymal scar at the site of the nephrostomy tract after several weeks. However, tissue adjacent to, as well as relatively distant from, the tract is also injured during PCNL. Such injury, and any associated interstitial inflammation, may resolve but may also progress to fibrosis and scarring. 2 Further, none of these studies has compared the effects of tract dilatation methods on renal function. In our series, we compared the effects of tract dilation methods on global and regional renal function using QSPECT of 99mTc-DMSA. New focal cortical defects on 99mTc-DMSA scan were seen in nine patients (18%). In six of these kidneys the site of focal defect corresponded to the access site for tract formation during PCNL (no patient in balloon dilation group; two in group II; four in group III). We did not observe difficulties in establishing the tract in these six patients who had focal defect in site of tract formation. There were no significant intraoperative problems except in one patient, who had bleeding from an infundibular tear attributable to torquing (in group III). The hemoglobin drop was 3.2 g/dL, necessitating blood transfusion. One patient had prolonged hospital stay because of urinary leakage from nephrostomy tract after the removal of the tube. It resolved spontaneously in 4 days without intervention. An another patient in group III had fever postoperatively and required antibiotic treatment because of positive urine culture. In the other three renal units who had unrelated site defects on isotope scans, the reason of focal defects could be due to other factors, for example, infection, intraoperative instrumental injury, bleeding, or SWL treatment.
Total relative uptake was preserved in 37 (74%) patients. Five (one in group I; two in group II; two in group III; 10%) patients had a decrease in renal function, and an improvement in renal functions occurred in eight (two in group I; two in group II; four in group III) patients. However, there were no statistically significant differences between the groups for total uptake and area of the treated kidneys before and after the procedure. None of the patients in group I, but one patient in group II and two in group III needed blood transfusions. We believed that using the balloon dilator has the advantage of less operative time and results in less trauma to the tract. Because the inflated balloon supplies constant pressure, rather than a shearing force, on the access tract, the balloon dilator is less traumatic and results in less bleeding and scar formation. 22 The effect of various methods of nephrostomy tract dilatation on blood loss during PCNL has been the subject of several clinical studies. Davidoff and Bellman 23 reported a significantly lower blood transfusion rate in 143 of their patients in whom the tract were dilated using the balloon compared with those in whom Amplatz fascial dilators were used.
Possible changes in renal function as an indicator of renal damage have also been studied. Serum creatinine and blood pressure were determined before and after treatment, and there was no significant difference between any of the parameters before and after PCNL.
Conclusion
The results suggest that QSPECT of 99mTc-DMSA is a noninvasive method that is able to assess changes in individual renal function. QDMSA confirms that renal function is preserved or often improved after percutaneous stone removal. Balloon dilatation technique provides urologists with a better surgical alternative to the other dilatation methods, resulting in minimal renal damage from the formation of the nephrostomy tract and lower transfusion rates.
Footnotes
Disclosure Statement
No competing financial interests exist.